
 PDF下载 ( 1559 KB)
PDF下载 ( 1559 KB)

Advances in the application of artificial liver in liver failure
-
摘要: 肝衰竭是各种肝病发展的严重阶段,病情发展快且危重,病死率高。人工肝不仅可以清除患者体内的有害物质,补充必需物质,为肝细胞再生及肝功能恢复创造机会,而且能延长患者等待肝移植的时间,是肝移植前的桥接。但如今人工肝治疗的广泛开展面临重重困难,如血源紧张、细胞来源困难、疗效不够理想、价格昂贵等,迫切需要创新及改进人工肝治疗方法。近年来发展的新型非生物型人工肝模式,如双重血浆分子吸附系统、分子吸附再循环系统、连续白蛋白净化系统、血浆滤过透析等多种模式的联合应用,在保证疗效的同时节省了血浆用量,减少了副作用。生物型及混合型人工肝具有肝特异性解毒、生物合成及转化功能,有巨大的应用潜能,但细胞来源、细胞培养及生物反应器是其临床应用主要的局限因素。阐述了人工肝在肝衰竭治疗中的现状及应用进展,并为人工肝的发展指出了研究方向。Abstract: Liver failure is a serious stage in the development of various liver diseases, with rapid progression, critical conditions, and a high mortality rate. Artificial liver can eliminate toxic substances in the body, supplement essential substances, and create opportunities for hepatocyte regeneration and liver function recovery, and in addition, it can also prolong the waiting time for liver transplantation and thus acts as a bridge to liver transplantation. However, the wide application of artificial liver is facing many difficulties nowadays, such as shortage of blood sources, difficulties in cell sources, a lack of satisfactory effects, and high costs, and therefore, artificial liver treatment needs innovation and improvement. New non-bioartificial liver systems developed in recent years, such as double plasma molecular absorption system, molecular absorbent recirculating system, continuous albumin purification system, and plasma diafiltration, can help to achieve a good clinical outcome and meanwhile reduce the amount of plasma used and minimize side effects. Biological artificial liver and hybrid artificial liver systems have the functions of specific detoxification, biosynthesis, and transformation and thus have great potential in clinical application, which is limited by cell source, cell culture, and bioreactor. This article elaborates on the current status and advances in the application of artificial liver in the treatment of liver failure and provides research directions for the development of artificial liver.
-
Key words:
- liver failure /
- liver, artificial
-
慢性HBV感染者如不接受有效的抗病毒治疗可能会发展为肝硬化,代偿期乙型肝炎肝硬化患者中位生存期约为12年,而当病情发展至失代偿期乙型肝炎肝硬化,患者的中位生存期仅有2年左右[1]。研究[2-3]证实有效的抗病毒治疗可以改善失代偿期乙型肝炎肝硬化患者的肝功能,使部分患者达到再代偿状态。国外有研究[4]对使用替诺福韦抗病毒治疗的失代偿期乙型肝炎肝硬化患者进行了随访,发现有48.6%的患者在抗病毒治疗2年后出现肝功能逆转,实现再代偿。但是目前对于失代偿期乙型肝炎肝硬化再代偿的影响因素尚不完全明确,笔者对核苷类药物治疗的初次失代偿期乙型肝炎肝硬化患者进行了回顾性分析,以期了解患者再代偿的影响因素。
1. 资料与方法
1.1 研究对象
本研究纳入2011年9月1日—2019年12月31日就诊于本院的首次失代偿期乙型肝炎肝硬化住院患者,根据随访结束时患者的结局分为再代偿组和持续失代偿组。纳入标准:(1)年龄≥18周岁;(2)所有患者均在首次失代偿事件发生前3个月内或第1次发生后立刻使用核苷类药物抗病毒治疗;(3)失代偿期乙型肝炎肝硬化诊断符合《慢性乙型肝炎防治指南(2019年版)》[5];(4)再代偿乙型肝炎肝硬化符合《肝硬化诊治指南》[6],即失代偿期乙型肝炎肝硬化患者经过有效的病因治疗及对症治疗后失代偿并发症(腹水,消化道出血,肝性脑病,自发性腹膜炎及肝衰竭)消失并维持超过1年;(5)持续病毒学应答(SVR)(即HBV DNA持续低于检测下限)符合本文作者所在单位检测标准,2018年6月前HBV DNA检测下限为500 IU/mL,2018年6月后检测下限为20 IU/mL。排除标准:(1)除HBV外合并其他嗜肝病毒感染;(2)合并自身免疫性肝病、酒精性肝病、药物性肝病等其他肝脏疾病;(3)既往有肝细胞癌病史或首次入院后6个月内诊断为肝细胞癌患者;(4)同时患有其他显著影响患者生存率的疾病,包括其他血液病、免疫性疾病或恶性肿瘤等其他重大疾病;(5)有脾切除手术史,经颈静脉肝内门体分流术史或随访过程中行肝移植手术的患者。
1.2 数据收集及随访
人口统计学资料来自于电子病历系统。实验室检查资料为患者住院期间首次检查的临床或生物化学资料,根据患者门诊和住院记录及出院后电话随访记录患者情况。以患者首次因失代偿期乙型肝炎肝硬化入院时间为起始时间,患者死亡、失访以及研究结束时(2020年12月31日)仍生存为截尾数据。
1.3 观察指标
一般情况包括性别、年龄、家族史,抗病毒药物有阿德福韦(正大天晴药业集团股份有限公司),替比夫定(北京诺华制药有限公司),恩替卡韦(中美上海施贵宝制药有限公司,正大天晴药业集团股份有限公司),替诺福韦(正大天晴药业集团股份有限公司、葛兰素史克有限公司),丙酚替诺福韦(吉利德科学公司);实验室指标包括血常规,肝功能,肾功能,电解质,HBV DNA定量(检测法:Taqman实时荧光定量PCR法,试剂:厦门安普利乙型肝炎病毒检测试剂盒,检测灵敏度:2018年6月前为500 IU/mL,2018年6月后为20 IU/mL),国际标准化比值(INR)和甲胎蛋白(AFP);肝功能评价指标包括CTP评分和终末期肝病模型(MELD)评分。
1.4 统计学方法
采用SPSS 23.0对数据进行统计分析。所有计量资料均为非正态分布,采用M(P25~P75) 表示,2组间比较采用Mann-Whitney U检验。计数资料组间比较采用χ2检验。Cox风险比例回归模型用于分析与再代偿相关的影响因素。采用Kaplan-Meier法绘制生存曲线,log-rank检验生存曲线。P<0.05为差异有统计学意义。
2. 结果
2.1 一般资料
本研究共纳入患者438例,平均年龄51(44~62)岁,男282例(64.4%),女156例(35.6%)。73例有乙型肝炎家族史。首次失代偿事件为腹水有300例(68.5%),消化道出血99例(22.6%),肝性脑病41例(9.4%),自发性腹膜炎37例(8.4%)。所有患者初次失代偿事件仅有1件的有366例(83.6%)。随访过程中实现SVR患者261例(59.6%)。101例(23.0%)患者最终死亡,其中78例(77.2%)患者死于肝硬化失代偿并发症,23例(22.8%)患者死于原发性肝癌。
2.2 再代偿患者基本临床特征
如表 1所示,438例首次失代偿期乙型肝炎肝硬化患者中实现再代偿患者199例(45.4%),男127例(63.8%),女72例(36.2%)。
表 1 再代偿患者与持续失代偿患者临床基线资料比较Table 1. Clinical baseline data for recompensated patients and persistent decompensation patients项目 再代偿组(n=199) 持续失代偿组(n=239) 统计值 P值 男/女(例) 127/72 155/84 χ2=0.005 0.941 年龄(岁) 50(44~59) 51(44~64) Z=4.797 0.101 随访时间(月) 23.0(15.0~45.0) 20.5(9.0~60.8) Z=-0.227 0.820 家族史[例(%)] 32(16.1) 41(17.2) χ2=0.009 0.764 SVR(例) 162/37 99/140 χ2=72.093 <0.001 首次失代偿事件 单个/多个并发症(例) 179/20 187/52 χ2=9.834 0.002 腹水[例(%)] 145(72.9) 155(64.9) χ2=3.299 0.072 消化道出血[例(%)] 34(17.1) 65(27.2) χ2=6.346 0.012 肝性脑病[例(%)] 13(6.5) 28(11.7) χ2=0.438 0.064 自发性腹膜炎[例(%)] 14(7.0) 23(9.6) χ2=0.941 0.332 Scr(μmol/L) 59(49~70) 62(51~76) Z=-1.035 0.011 INR 1.44(1.23~1.62) 1.46(1.23~1.64) Z=-0.545 0.461 Alb(g/L) 32.4(29.2~36.7) 31.7(27.7~36.4) Z=0.793 0.119 TBil(μmol/L) 32.5(21.0~60.7) 30.7(18.3~54.8) Z=-1.423 0.590 Na(mmol/L) 140.0(137.7~142.0) 139.0(136.6~141.6) Z=-1.606 0.019 WBC(×109/L) 3.6(2.7~5.0) 3.7(2.6~5.6) Z=-0.735 0.620 Hb(g/L) 116(99~133) 112(88~127) Z=1.455 0.006 NLR 2.06(1.36~3.53) 2.28(1.51~4.40) Z=-0.965 0.087 PLT(×109/L) 69(49~102) 64(46~96) Z=-0.312 0.332 ALT(U/L) 56(32~110) 41(23~70) Z=-2.194 <0.001 AFP(ng/mL) 11.30(3.49~71.84) 10.25(3.19~70.46) Z=-2.032 0.243 MELD评分 10.42(6.66~14.29) 10.77(7.18~15.50) Z=0.384 0.251 CTP评分 7(6~9) 7(6~9) Z=-0.085 0.160 CTP分级[例(%)] χ2=4.297 0.117 A级 83(41.7) 77(32.2) B级 74(37.2) 106(44.4) C级 42(21.1) 56(23.4) 注:Scr,血清肌酐;NLR, 中性粒细胞与淋巴细胞比值。 进一步分析,在首次失代偿后第1年即获得再代偿的患者有45例(22.6%),在第2、3、4、5年获得再代偿的患者分别有71例(35.7%)、23例(11.6%)、24例(12.1%)、18例(9.0%),首次失代偿超过5年才出现再代偿的患者有18例(9.0%)。
同时发现,199例再代偿患者中,78例再次失代偿。首次失代偿后第2、3、4、5年发生再次失代偿的患者分别有28、18、12、10例,再代偿组患者2、3、4、5年的累积再次失代偿率分别为14.1%、23.1%、29.1%、34.2%。78例再次失代偿的患者再代偿持续时间18(16~22)个月。
2.3 再代偿患者与持续失代偿患者的比较
如表 1所示,239例持续失代偿患者中位随访期为20.5个月(9.0~ 60.8个月),与再代偿患者随访时间无明显差异。199例再代偿患者中达到SVR的有162例,基线仅有1个并发症的患者有179例,239例持续失代偿患者达到SVR的有99例,基线并发症数量1个的患者有187例,两组患者的SVR率(81.4% vs 41.4%, P<0.001)及并发症数量(92.5% vs 82.0%,P=0.002)有显著差异。再代偿患者Scr值显著低于失代偿组患者(P=0.011),而Hb、ALT及血钠水平显著高于失代偿组患者(P值均<0.05)。
2.4 再代偿的相关影响因素分析
Cox多因素回归分析显示,SVR、ALT及Scr是再代偿的独立影响因素(P值均<0.05)。其中,SVR及ALT是再代偿的保护因素,Scr是实现再代偿的危险因素(表 2)。
表 2 再代偿相关影响因素的多因素分析Table 2. Multivariate analysis of the influencing factors related to recompensation自变量 β值 SE Wald OR 95%CI P值 ALT 0.002 0.001 6.802 1.002 1.000~1.003 0.009 单个并发症 -0.412 0.354 1.358 0.662 0.331~1.324 0.244 SVR 1.751 0.235 55.516 5.760 3.634~9.129 <0.001 Scr -0.010 0.005 3.955 0.990 0.981~1.000 0.047 Hb 0.004 0.004 1.065 1.004 0.996~1.012 0.302 2.5 不同代偿状态对患者长期生存率的影响
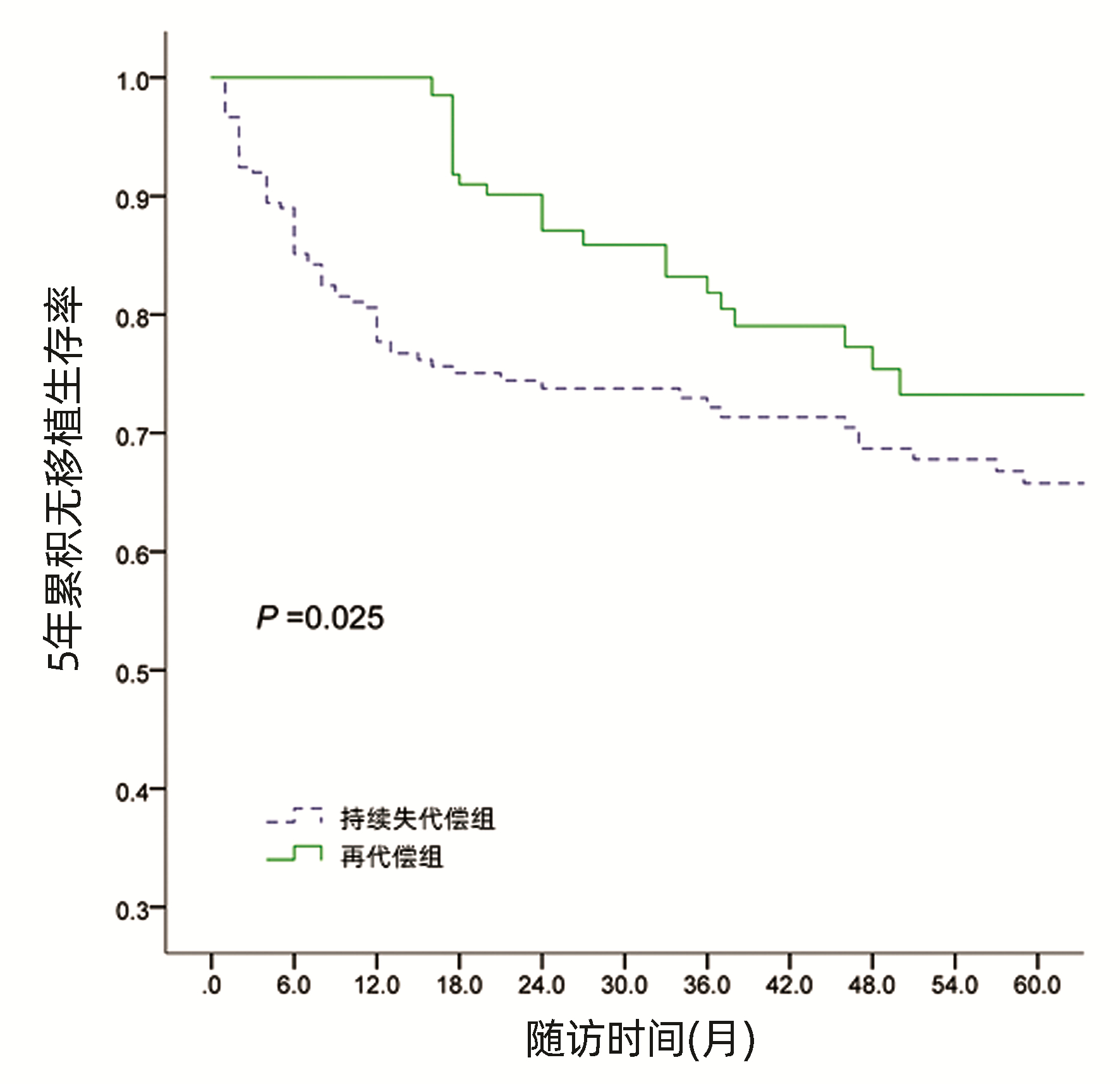
经Kaplan-Meier生存曲线分析显示,再代偿患者5年累积无移植生存率87.9%,显著高于持续失代偿组5年累积无移植生存率72.0%(χ2=9.886,P=0.025)(图 1)。
 图 1 不同代偿状态患者5年累积无移植生存率Figure 1. The 5-year cumulative transplant free survival rate of patients with different compensated states
图 1 不同代偿状态患者5年累积无移植生存率Figure 1. The 5-year cumulative transplant free survival rate of patients with different compensated states3. 讨论
目前已有较多研究证实失代偿期乙型肝炎肝硬化患者经过包括抗病毒治疗在内的综合治疗后生存期显著改善[7-8],部分患者可逆转为再代偿状态[9],但对实现再代偿的相关影响因素仍未完全明确。
本研究对438例首次失代偿期乙型肝炎肝硬化患者进行回顾性分析,结果显示199例患者获得再代偿,再代偿率45.4%,第1年再代偿率22.6%。而另一项与本研究同样针对初治失代偿期乙型肝炎肝硬化的研究[10]显示,1年再代偿率49%,高于本研究,考虑这一差异可能与再代偿的定义不同有关。该研究定义再代偿为抗病毒治疗1年后CTP评分下降至少2分。这也提示需统一失代偿期肝硬化获得再代偿的评判标准,为后期关于再代偿的研究提供参考。
本研究发现199例再代偿患者最终仍有78例出现再次失代偿,占再代偿患者的39.1%。同时还发现再次失代偿多发生在再代偿后的第2年,这提示对已经获得再代偿的患者也要积极治疗,密切监控相关指标,预防患者再次失代偿。
本研究发现了基线ALT、Scr水平及是否达到SVR与失代偿期乙型肝炎肝硬化患者实现再代偿密切相关。ALT是失代偿期乙型肝炎肝硬化患者实现再代偿的独立影响因素。Chang等[11]研究发现初次失代偿期肝硬化ALT≥5倍正常值上限的患者比ALT正常的患者长期预后更好。其原因可能与ALT水平高的患者抗HBV免疫反应活跃并且再代偿能力更强有关。Scr是失代偿期乙型肝炎肝硬化患者实现再代偿的另一个独立影响因素。Scr可以有效的预测失代偿期肝硬化患者的预后,有研究[12-13]发现Scr水平高的患者更易于发生慢加急性肝衰竭及肝肾综合征,预后不佳,这与本研究结果基本一致。笔者前期研究[14]表明实现SVR的失代偿期乙型肝炎肝硬化患者长期预后较好。本文进一步发现实现SVR的患者更容易实现再代偿。有研究[15-16]发现失代偿期乙型肝炎肝硬化患者中,与未达到SVR的患者相比,达到SVR的患者长期生存率更高且5年肝癌发生率更低。说明抗病毒治疗实现SVR的患者肝功能得到进一步改善,进而促进患者实现再代偿。
令人感兴趣的是,既往有研究[17]认为MELD评分与失代偿期肝硬化患者实现再代偿相关,而本研究未观察到该结果。这一差异可能与再代偿的评判标准及患者的病因不一致等因素有关。
本研究尚存在一些不足。如单中心回顾性临床研究,样本量较少,病例存在偏倚等,后期笔者团队将采取前瞻性研究,进一步证实本研究结果的可靠性。
综上所述,初次失代偿期乙型肝炎肝硬化患者经过综合治疗后能否实现再代偿与基线ALT、Scr水平及是否达到SVR密切相关。其中,实现SVR和基线ALT高水平的患者更容易实现再代偿,而基线高Scr的患者不易实现再代偿。临床上应关注以上指标,对于失代偿期肝硬化患者,密切观察病情,规范治疗管理,防止并发症发生。
-
[1] Liver Failure and Artificial Liver Group, Chinese Severe Liver Disease and Artificial Liver Group, Chinese of Hepatology, CMA.Guideline for diagnosis and treatment of liver failure[J].Chin JClin Infect Dis, 2012, 5 (6) :321-327. (in Chinese) 中华医学会感染病学分会肝衰竭与人工肝学组.中华医学会肝病学分会重型肝病与人工肝学组.肝衰竭诊治指南 (2012年版) [J].中华临床感染病杂志, 2012, 5 (6) :321-327. [2] Liver Failure and Artificial Liver Group, Chinese of Hepatology, CMA.Guideline for non-bioartificial liver support systems in treatment of liver failure:2016 update[J].Chin J Clin Infect Dis, 2016, 9 (2) :97-103. (in Chinese) 中华医学会感染病学分会肝衰竭与人工肝学组.非生物型人工肝治疗肝衰竭指南 (2016年版) [J].中华临床感染病杂志, 2016, 9 (2) :97-103. [3]WANG YY, HUANG JR.Research advances in artificial liver support therapy for liver failure[J].J Clin Intern Med, 2014, 31 (8) :509-512. (in Chinese) 王银银, 黄建荣.人工肝治疗肝衰竭研究进展[J].临床内科杂志, 2014, 31 (8) :509-512. [4]MOREAU R, ARROYO V.Acute-on-chronic liver failure:a new clinical entity[J].Clin Gastroenterol Hepatol, 2015, 13 (5) :836-841. [5]XU X, LIU X, LING Q, et al.Artificial liver support system combined with liver transplantation in the treatment of patients with acute-on-chronic liver failure[J].PLo S One, 2013, 8 (3) :e58738. [6]LIU YY, HUANG JR.Changes and perspectives of non-biological artificial liver treatment[J].Chin J Hepatol, 2017, 25 (9) :646-650. (in Chinese) 刘月英, 黄建荣.非生物型人工肝治疗的变迁与展望[J].中华肝脏病杂志, 2017, 25 (9) :646-650. [7]LI RH, FU L, HUANG Y, et al.Clinical research of double plasma molecular absorption system in treatment of liver failure[J].China J Modern Med, 2018, 28 (1) :78-82. (in Chinese) 李荣华, 傅蕾, 黄燕, 等.双重血浆分子吸附治疗肝衰竭的临床研究[J].中国现代医学杂志, 2018, 28 (1) :78-82. [8]ZHANG BW, YANG XF, LUO XJ, et al.Comparison of clinical effects of double plasma molecular adsorption system, plasma bilirubin adsorption and plasma exchange in liver failure[J].China JModern Med, 2016, 26 (12) :103-106. (in Chinese) 张宝文, 阳学风, 罗湘俊, 等.双重血浆吸附、胆红素吸附及血浆置换治疗肝衰竭的疗效比较[J].中国现代医学杂志, 2016, 26 (12) :103-106. [9]WAN YM, LI YH, XU ZY, et al.Therapeutic plasma exchange versus double plasma molecular absorption system in hepatitis B virus-infected acute-on-chronic liver failure treated by entercavir:A prospective study[J].J Clin Apher, 2017, 32 (6) :453-461. [10]OLIN P, HAUSKEN J, FOSS A, et al.Continuous molecular adsorbent recirculating system treatment in 69 patients listed for liver transplantation[J].Scand J Gastroenterol, 2015, 50 (9) :1127-1134. [11]HANISH SI, STEIN DM, SCALEA JR, et al.Molecular adsorbent recirculating system effectively replaces hepatic function in severe acute liver failure[J].Ann Surg, 2017, 266 (4) :677-684. [12]SPONHOLZ C, MATTHES K, RUPP D, et al.Molecular adsorbent recirculating system and single-pass albumin dialysis in liver failure-a prospective, randomised crossover study[J].Crit Care, 2016, 20:2. [13]GERTH HU, POHLEN M, THLKING G, et al.Molecular adsorbent recirculating system can reduce short-term mortality among patients with acute-on-chronic liver failure-a retrospective analysis[J].Crit Care Med, 2017, 45 (10) :1616-1624. [14]BANARES R, NEVENS F, LARSEN FS, et al.Extracorporeal albumin dialysis with the molecular adsorbent recirculating system in acute-on-chronic liver failure:The RELIEF trial[J].Hepatology, 2013, 57 (3) :1153-1162. [15]DONG QH, GUO LM, WANG Y, et al.Clinical study of continuous albumin purification system in the treatment of patients with liver failure[J].J Pract Hepatol, 2009, 12 (5) :352-354. (in Chinese) 董庆华, 郭利民, 王宇, 等.CAPS人工肝治疗肝衰竭的临床研究[J].实用肝脏病杂志, 2009, 12 (5) :352-354. [16]KOMARDINA E, YAROUSTOVSKY M, ABRAMYAN M, et al.Prometheus therapy for the treatment of acute liver failure in patients after cardiac surgery[J].Kardiochir Torakochirurgial Pol, 2017, 14 (4) :230-235. [17]LIU XH, GUO HQ.Progress in technology and clinical application of non-bioartificial liver support system[J].J Clin Hepatol, 2013, 29 (9) :661-665. (in Chinese) 刘晓慧, 郭海清.非生物型人工肝技术及其临床应用新进展[J].临床肝胆病杂志, 2013, 29 (9) :661-665. [18]XING HQ, LIU JW, WANG KL, et al.Analysis of clinical effect of continuous plasma diafiltration for the therapy of liver failure[J].BME Clin Med, 2013, 17 (2) :152-155. (in Chinese) 邢汉前, 刘俊微, 王开利, 等.持续缓慢血浆透析滤过治疗肝功能衰竭的临床疗效分析[J].生物医学工程与临床, 2013, 17 (2) :152-155. [19]KOMURA T, TANIGUCHI T, SAKAI Y, et al.Efficacy of continuous plasma diafiltration therapy in critical patients with acute liver failure[J].J Gastroenterol Hepatol, 2014, 29 (4) :782-786. [20]YANG XS, ZHOU L, LI L, et al.Influence of duration of plasma diafiltration on therapeutic outcome of liver failure[J].J Clin Hepatol, 2018, 34 (5) :1052-1054. (in Chinese) 杨仙珊, 周莉, 李璐, 等.血浆透析滤过治疗时间对肝衰竭治疗效果的影响[J].临床肝胆病杂志, 2018, 34 (5) :1052-1054. [21]ZHOU N, LI J, ZHANG Y, et al.Efficacy of coupled low-volume plasma exchange with plasma filtration adsorption in treating pigs with acute liver failure:A randomised study[J].J Hepatol, 2015, 63 (2) :378-387. [22]LI S, CHEN Y.Coping with shortage of plasma-the new therapeutic pattern of non-bioartificial liver[J].J Clin Hepatol, 2017, 33 (9) :1687-1692. (in Chinese) 李爽, 陈煜.血浆紧缺情况下非生物型人工肝治疗新模式的探讨[J].临床肝胆病杂志, 2017, 33 (9) :1687-1692. [23]ZHOU YD, YANG L, HAN QF, et al.Clinical effect of combined artificial extra corporeal liver support therapy for toxic hepatic failure[J].Chin J Ind Hyg Occup Dis, 2017, 35 (1) :51-53. (in Chinese) 周亚东, 杨琳, 韩秋风, 等.组合型人工肝技术治疗中毒性肝功能衰竭的临床研究[J].中华劳动卫生职业病杂志, 2017, 35 (1) :51-53. [24]ZHOU J, WAN H, YANG ZM, et al.Clinical effect of plasma perfusion combined with plasma exchange in treatment of patients with acute-on chronic liver failure[J].J Clin Hepatol, 2017, 33 (4) :715-718. (in Chinese) 周渐, 万红, 杨正茂, 等.血浆灌流联合血浆置换治疗慢加急性肝衰竭的效果观察[J].临床肝胆病杂志, 2017, 33 (4) :715-718. [25]FAN JH, CHEN HY, WANG HT, et al.Plasma exchange combined with plasma perfusion in treatment of patients with liver failure[J].J Pract Hepatol, 2016, 19 (2) :184-187. (in Chinese) 范晶华, 陈红英, 王宏图, 等.血浆置换联合血浆灌流治疗肝衰竭患者临床疗效分析[J].实用肝脏病杂志, 2016, 19 (2) :184-187. [26]WANG GH, LIU KH, ZHANG XY, et al.The clinical efficacy analysis of plasma exchange combined with plasma perfusion in treatment of acute liver failure[J].Chin J Gastroenterol Hepatol, 2017, 26 (11) :1294-1297. (in Chinese) 王盖昊, 刘凯辉, 张潇艺, 等.血浆置换联合血浆灌流治疗急性肝衰竭的临床疗效分析[J].胃肠病学和肝病学杂志, 2017, 26 (11) :1294-1297. [27] LI LJ.Liver failure and the progress of Li’s artificial liver system[J].Chin J Clin Infect Dis, 2017, 10 (2) :91-94. (in Chinese) 李兰娟.肝衰竭与李氏人工肝进展[J].中华临床感染病杂志, 2017, 10 (2) :91-94. [28] SHI XL, GAO Y, YAN Y, et al.Improved survival of porcine acute liver failure by a bioartificial liver device implanted with induced human functional hepatocytes[J].Cell Res, 2016, 26 (2) :206-216. [29]TAO KS, LI X, DOU KF.The history and development of xenogeneic liver transplantation[J].Ogran Transplant, 2017, 8 (2) :85-88. (in Chinese) 陶开山, 李霄, 窦科峰.异种肝移植的历史与发展[J].器官移植, 2017, 8 (2) :85-88. [30]LIU H, YOU S, RONG Y, et al.The newly established human liver cell line:A potential cell source for the bioartificial liver in the future[J].Hum cell, 2013, 26 (4) :155-161. [31]YAN Q, DENG L, ZHAO X, et al.Establishment and characterization of an immortalized human hepatocyte line for the development of bioartificial liver system[J].Cytotechnology, 2018, 70 (2) :665-674. [32]SHI XL, GAO Y, YAN Y, et al.Improved survival of porcine acute liver failure by a bioartificial liver device implanted with induced human functional hepatocytes[J].Cell Res, 2016, 26 (2) :206-216. [33]HUANG P, ZHANG L, GAO Y, et al.Direct reprogramming of human fibroblasts to functional and expandable hepatocytes[J].Cell Stem Cell, 2014, 14 (3) :370-384. [34]DING YT.Bioartificial liver and liver transplantation:New modalities for the treatment of liver failure[J].J Clin Hepatol, 2017, 33 (9) :1693-1698. (in Chinese) 丁义涛.生物人工肝和肝移植:肝衰竭治疗新模式[J].临床肝胆病杂志, 2017, 33 (9) :1693-1698. [35]HOU P, LI Y, ZHANG X, et al.Pluripotent stem cells induced from mouse somatic cells by small-molecule compounds[J].Science, 2013, 341 (6146) :651-654. [36]LI GL, WANG SM.The development and status of bioartificial liver[J].Chin J Surg, 2017, 55 (12) :957-959. (in Chinese) 李刚磊, 王世明.生物型人工肝的发展及现状[J].中华外科杂志, 2017, 55 (12) :957-959. [37]ZHANG S, CHEN L, LIU T, et al.Integration of single-layer skin hollow fibers and scaffolds develops a three-dimensional hybrid bioreactor for bioartificial livers[J].J Mater Sci Mater Med, 2014, 25 (1) :207-216. [38]ZHANG S, ZHANG B, CHEN X, et al.Three dimensional culture in a microgravity bioreactor improves the engraftment efficiency of hepatic tissue constructs in mice[J].J Mater Sci Mater Med, 2014, 25 (12) :2699-2709. [39]VERMA SK, MODI A, BELLARE J.Three-dimensional multiscale fiber matrices:Development and characterization for increased Hep G2 functional maintenance for bio-artificial liver application[J].Biomater Sci, 2018, 6 (2) :280-291. [40]SHI XL, HAN B, ZHENG YS, et al.Primary clinical study of a novel multi-layer flat-plate bioartificial liver for patients with liver failure[J].Chin J Organ Transplant, 2012, 33 (4) :212-216. (in Chinese) 施晓雷, 韩冰, 郑以山, 等.新型多层平板型生物人工肝体外支持系统治疗肝功能衰竭的临床研究[J].中华器官移植杂志, 2012, 33 (4) :212-216. [41]PODOLL AS, DEGOLOVINE A, FINKEL KW.Liver support systems-a review[J].ASAIO J, 2012, 58 (5) :443-449. [42]GU JY, SHI XL, REN HZ, et al.Systematic evaluation of extracorporeal bioartificial liver support system for the treatment of liver failure[J].Chin J Tissue Engineer Res, 2013, 17 (18) :149-155. (in Chinese) 顾劲扬, 施晓雷, 任昊帧, 等.体外生物人工肝支持系统治疗肝功能衰竭的系统评价[J].中国组织工程研究, 2013, 17 (18) :149-155. [43]YOU SL, LIU HL, RONG YH, et al.Preliminary investigation of hybrid bioartificial liver support system in treatment of HBV-related acute-on-chronic liver failure[J].J Clin Hepatol, 2013, 29 (9) :685-688. (in Chinese) 游绍莉, 刘鸿凌, 荣义辉, 等.混合型生物型人工肝治疗HBV相关慢加急性肝衰竭患者的初步探讨[J].临床肝胆病杂志, 2013, 29 (9) :685-688. [44]HUANG JR.Current status and perspectives of artificial liver for treatment of acute-on-chronic liver failure[J].Chin J Hepatol, 2016, 24 (12) :935-939. (in Chinese) 黄建荣.人工肝在慢加急性肝衰竭中的应用现状及展望[J].中华肝脏病杂志, 2016, 24 (12) :935-939. [45]YU XP, PAN XP, LI LJ.Research advances in stem cell-derived hepatocytes and their application in bioartificial liver[J].Chin J Infect Dis, 2014, 32 (10) :632-634. (in Chinese) 虞晓鹏, 潘小平, 李兰娟.干细胞来源的肝细胞及其在生物型人工肝中的应用研究进展[J].中华传染病杂志, 2014, 32 (10) :632-634. 期刊类型引用(9)
1. 赵勇娜,谢颖. 不同炎症因子对肝硬化腹水并发腹腔感染的预测效能研究. 中国医学工程. 2024(04): 8-12 .  百度学术
百度学术2. 曹志军,汪晓军. 中西医联合治疗乙肝肝硬化的临床进展. 世界复合医学(中英文). 2024(01): 189-194 . 百度学术3. 石敏,郝彦琴. 失代偿期肝硬化患者发生再代偿的临床研究进展. 中国药物与临床. 2024(08): 539-544 . 百度学术4. 牛日雨,尹伟,王益杰,李成忠. 失代偿期肝硬化再代偿的研究进展. 肝脏. 2024(07): 770-773 . 百度学术5. 荣欣欣,徐缘媛,杨广德,王霞,傅涓涓,李丽,潘修成. 富马酸丙酚替诺福韦治疗首次失代偿期乙型肝炎肝硬化患者的效果和安全性分析. 临床肝胆病杂志. 2024(10): 2008-2013 .  本站查看
本站查看6. 刘晓金,刘晓明,陆旭. 肝硬化失代偿期患者并发肠梗阻的危险因素分析及临床管理对策研究. 黑龙江医学. 2024(24): 2981-2984+2987 . 百度学术7. 钱盈,张笑涵. 血清锌浓度与肝硬化失代偿肝功能损伤程度的关联及对预后的预测效能. 实用医技杂志. 2023(05): 305-309 . 百度学术8. 谢颖,赵勇娜. 肝硬化腹水患者肠道菌群变化对自发性腹膜炎的预测效能分析. 淮海医药. 2023(06): 580-584 . 百度学术9. 宋木生,杨椿,李静,温婷. 慢性乙型肝炎肝硬化失代偿期患者发生医院感染的病原学特点与危险因素分析. 抗感染药学. 2023(11): 1196-1199 . 百度学术其他类型引用(3)
-

 下载:
下载:
 百度学术
百度学术
 下载:
下载:

