
 PDF下载 ( 779 KB)
PDF下载 ( 779 KB)

肝外胆管恶性狭窄的鉴别诊断
DOI: 10.12449/JCH240433
利益冲突声明:本文不存在任何利益冲突。
作者贡献声明:孟春艳负责数据收集,论文撰写;王菁负责文献查询,研究指导;王波负责论文撰写及修改。
-
摘要: 引起肝外胆管狭窄的病因很多,其中良性狭窄可以通过药物治疗及内镜干预获得较好的疗效。恶性狭窄如能早期诊断,并及时行手术治疗有望延长患者的生存期。然而,肝外胆管恶性狭窄的鉴别诊断迄今为止仍然较为困难。本文就血清学、影像学、内镜相关技术及人工智能技术在肝外胆管恶性狭窄鉴别诊断中的进展进行综述,以期为制订临床诊疗方案提供策略和参考。
-
关键词:
- 胆管, 肝外 /
- 胰胆管造影术, 内窥镜逆行 /
- 人工智能 /
- 诊断, 鉴别
Abstract: There are various etiologies for extrahepatic bile duct stenosis, and pharmacotherapy and endoscopic intervention can achieve a good clinical effect in benign stenosis. Early diagnosis and timely surgical treatment of malignant stenosis may prolong the survival time of patients. However, there are still difficulties in the differential diagnosis of malignant bile duct stenosis. This article reviews the application of serology, radiology, endoscopic techniques, and artificial intelligence in the differential diagnosis of malignant bile duct stenosis, so as to provide strategies and references for formulating clinical diagnosis and treatment regimens. -
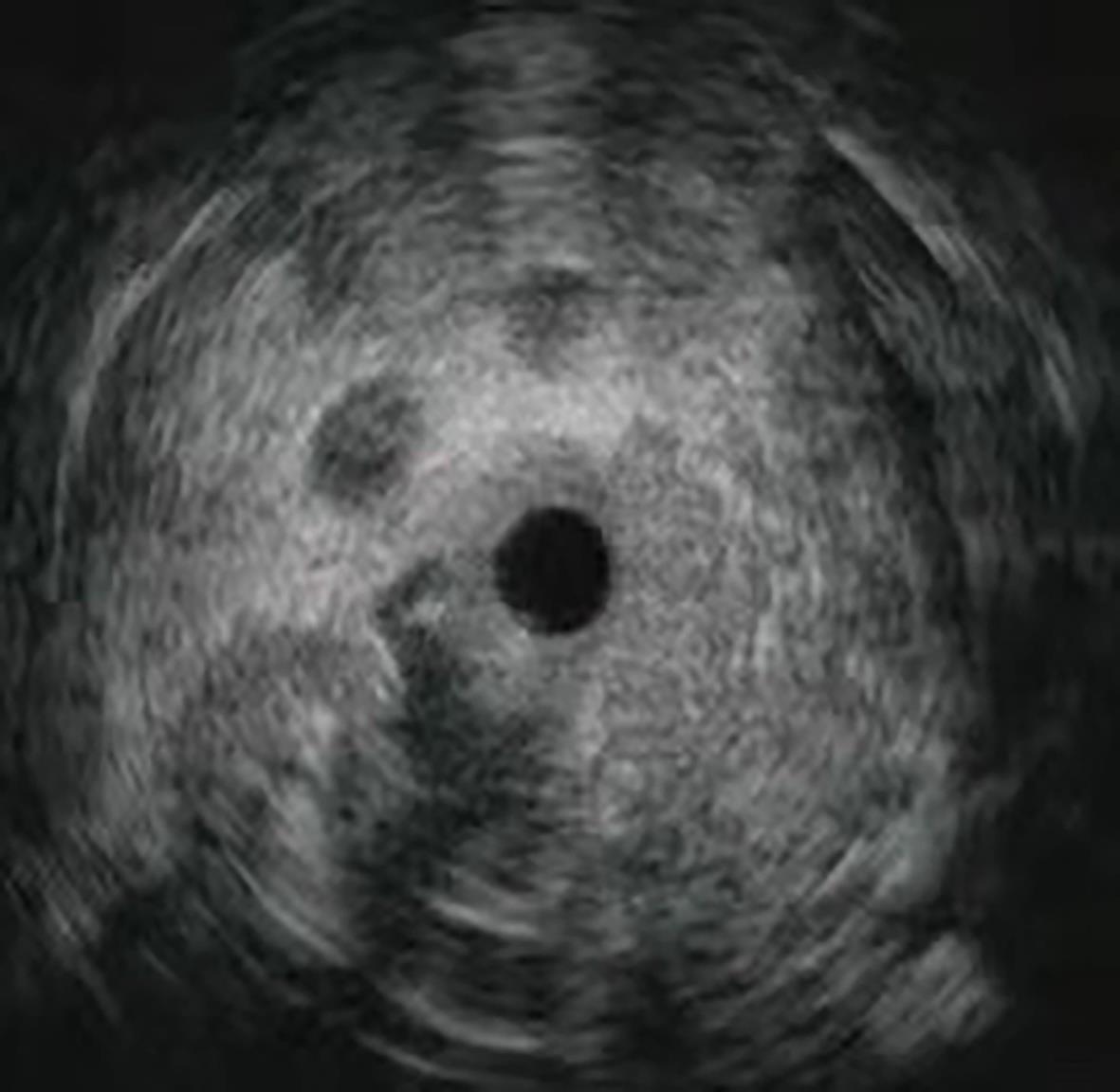
图 1 肝外胆管恶性狭窄的IDUS表现
Figure 1. Intraductal ultrasonography findings of malignant extrahepatic bile duct stenosis
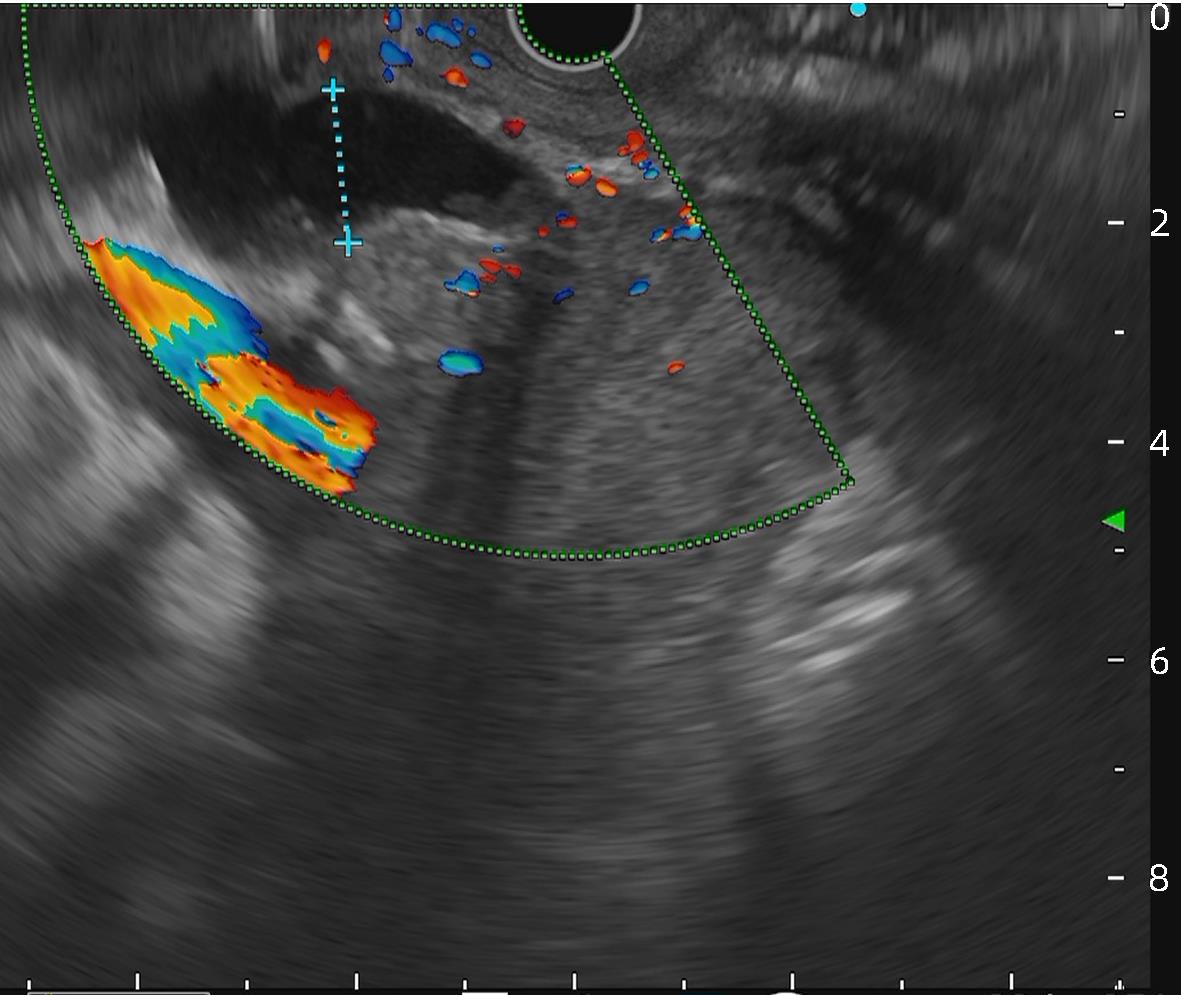
图 2 肝外胆管恶性狭窄的EUS表现
Figure 2. Endoscopic ultrasound imaging of malignant extrahepatic bile duct stenosis
-
[1] ELMUNZER BJ, MARANKI JL, GÓMEZ V, et al. ACG clinical guideline: Diagnosis and management of biliary strictures[J]. Am J Gastroenterol, 2023, 118( 3): 405- 426. DOI: 10.14309/ajg.0000000000002190. [2] BANALES JM, MARIN JJG, LAMARCA A, et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management[J]. Nat Rev Gastroenterol Hepatol, 2020, 17( 9): 557- 588. DOI: 10.1038/s41575-020-0310-z. [3] WANG JJ, XIA MX, JIN YB, et al. More endoscopy-based brushing passes improve the detection of malignant biliary strictures: A multicenter randomized controlled trial[J]. Am J Gastroenterol, 2022, 117( 5): 733- 739. DOI: 10.14309/ajg.0000000000001666. [4] WANG GX, GE XD, ZHANG D, et al. MRCP combined with CT promotes the differentiation of benign and malignant distal bile duct strictures[J]. Front Oncol, 2021, 11: 683869. DOI: 10.3389/fonc.2021.683869. [5] ZHANG YZ, JIANG QW, WANG Q, et al. Predicting malignancy of biliary stricture with a nomogram in patients with a non-malignant endoscopic tissue diagnosis: A retrospective study[J]. Cancer Manag Res, 2021, 13: 7735- 7745. DOI: 10.2147/CMAR.S333333. [6] XING HB, WANG J, WANG YL, et al. Diagnostic value of CA 19-9 and carcinoembryonic antigen for pancreatic cancer: A meta-analysis[J]. Gastroenterol Res Pract, 2018, 2018: 8704751. DOI: 10.1155/2018/8704751. [7] XIE CC, ALOREIDI K, PATEL B, et al. Indeterminate biliary strictures: A simplified approach[J]. Expert Rev Gastroenterol Hepatol, 2018, 12( 2): 189- 199. DOI: 10.1080/17474124.2018.1391090. [8] BOYD LNC, ALI M, KAM L, et al. The diagnostic value of the CA19-9 and bilirubin ratio in patients with pancreatic cancer, distal bile duct cancer and benign periampullary diseases, a novel approach[J]. Cancers, 2022, 14( 2): 344. DOI: 10.3390/cancers14020344. [9] MUTTILLO EM, CIARDI A, TROIANO R, et al. Pancreatic ductal adenocarcinoma and distal cholangiocarcinoma: A proposal of preoperative diagnostic score for differential diagnosis[J]. World J Surg Oncol, 2021, 19( 1): 10. DOI: 10.1186/s12957-021-02120-w. [10] DRAZILOVA S, VESELINY E, LENARTOVA PD, et al. IgG4-related sclerosing cholangitis: Rarely diagnosed, but not a rare disease[J]. Can J Gastroenterol Hepatol, 2021, 2021: 1959832. DOI: 10.1155/2021/1959832. [11] MADHUSUDHAN KS, DAS P, GUNJAN D, et al. IgG4-related sclerosing cholangitis: A clinical and imaging review[J]. AJR Am J Roentgenol, 2019, 213( 6): 1221- 1231. DOI: 10.2214/AJR.19.21519. [12] VOIGTLÄNDER T, METZGER J, HUSI H, et al. Bile and urine peptide marker profiles: Access keys to molecular pathways and biological processes in cholangiocarcinoma[J]. J Biomed Sci, 2020, 27( 1): 13. DOI: 10.1186/s12929-019-0599-5. [13] MACIAS RIR, MUÑOZ-BELLVÍS L, SÁNCHEZ-MARTÍN A, et al. A novel serum metabolomic profile for the differential diagnosis of distal cholangiocarcinoma and pancreatic ductal adenocarcinoma[J]. Cancers, 2020, 12( 6): 1433. DOI: 10.3390/cancers12061433. [14] LE LARGE TYS, MEIJER LL, PALECKYTE R, et al. Combined expression of plasma thrombospondin-2 and CA19-9 for diagnosis of pancreatic cancer and distal cholangiocarcinoma: A proteome approach[J]. Oncologist, 2020, 25( 4): e634- e643. DOI: 10.1634/theoncologist.2019-0680. [15] LEE DH, KIM B, LEE ES, et al. Radiologic evaluation and structured reporting form for extrahepatic bile duct cancer: 2019 consensus recommendations from the Korean society of abdominal radiology[J]. Korean J Radiol, 2021, 22( 1): 41- 62. DOI: 10.3348/kjr.2019.0803. [16] SHABANIKIA N, ADIBI A, EBRAHIMIAN S. Diagnostic accuracy of magnetic resonance cholangiopancreatography to detect benign and malignant biliary strictures[J]. Adv Biomed Res, 2021, 10: 38. DOI: 10.4103/abr.abr_137_20. [17] ZHU Y, JIN HL, MAO YF, et al. Unexplained distal obstructive biliary dilatation: A magnetic resonance cholangiopancreatography(MRCP)-based model to discriminate malignant from benign origins[J]. J Clin Gastroenterol, 2022, 56( 8): 724- 730. DOI: 10.1097/MCG.0000000000001614. [18] NAVANEETHAN U, NJEI B, LOURDUSAMY V, et al. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: A systematic review and meta-analysis[J]. Gastrointest Endosc, 2015, 81( 1): 168- 176. DOI: 10.1016/j.gie.2014.09.017. [19] KOBAYASHI M, RYOZAWA S, ARAKI R, et al. Investigation of factors affecting the sensitivity of bile duct brush cytology[J]. Intern Med, 2019, 58( 3): 329- 335. DOI: 10.2169/internalmedicine.1551-18. [20] ROTH GS, BICHARD P, FIOR-GOZLAN M, et al. Performance of bile aspiration plus brushing to diagnose malignant biliary strictures during endoscopic retrograde cholangiopancreatography[J]. Endosc Int Open, 2016, 4( 9): E997- E1003. DOI: 10.1055/s-0042-108854. [21] KATO A, KATO H, NAITOH I, et al. Use of endoscopic scraper and cell block technique as a replacement for conventional brush for diagnosing malignant biliary strictures[J]. Cancers, 2022, 14( 17): 4147. DOI: 10.3390/cancers14174147. [22] GONDA TA, VITERBO D, GAUSMAN V, et al. Mutation profile and fluorescence in situ hybridization analyses increase detection of malignancies in biliary strictures[J]. Clin Gastroenterol Hepatol, 2017, 15( 6): 913- 919. e 1. DOI: 10.1016/j.cgh.2016.12.013. [23] SINGHI AD, NIKIFOROVA MN, CHENNAT J, et al. Integrating next-generation sequencing to endoscopic retrograde cholangiopancreatography(ERCP)-obtained biliary specimens improves the detection and management of patients with malignant bile duct strictures[J]. Gut, 2020, 69( 1): 52- 61. DOI: 10.1136/gutjnl-2018-317817. [24] JANG SI, KWON NH, LIM BJ, et al. New staining method using methionyl-tRNA synthetase 1 antibody for brushing cytology of bile duct cancer[J]. Gastrointest Endosc, 2020, 92( 2): 310- 319. e 6. DOI: 10.1016/j.gie.2019.12.017. [25] JANG SI, NAHM JH, KWON NH, et al. Clinical utility of methionyl-tRNA synthetase 1 immunostaining in cytologic brushings of indeterminate biliary strictures: A multicenter prospective study[J]. Gastrointest Endosc, 2021, 94( 4): 733- 741. e 4. DOI: 10.1016/j.gie.2021.04.026. [26] MEISTER T, HEINZOW HS, WOESTMEYER C, et al. Intraductal ultrasound substantiates diagnostics of bile duct strictures of uncertain etiology[J]. World J Gastroenterol, 2013, 19( 6): 874- 881. DOI: 10.3748/wjg.v19.i6.874. [27] SEIFERT H, FUSAROLI P, ARCIDIACONO PG, et al. Controversies in EUS: Do we need miniprobes?[J]. Endosc Ultrasound, 2021, 10( 4): 246- 269. DOI: 10.4103/EUS-D-20-00252. [28] KIM HS, MOON JH, LEE YN, et al. Prospective comparison of intraductal ultrasonography-guided transpapillary biopsy and conventional biopsy on fluoroscopy in suspected malignant biliary strictures[J]. Gut Liver, 2018, 12( 4): 463- 470. DOI: 10.5009/gnl17205. [29] LEE JH, SALEM R, ASLANIAN H, et al. Endoscopic ultrasound and fine-needle aspiration of unexplained bile duct strictures[J]. Am J Gastroenterol, 2004, 99( 6): 1069- 1073. DOI: 10.1111/j.1572-0241.2004.30223.x. [30] PAUSAWASDI N, HONGSRISUWAN P, KAMANI L, et al. Diagnostic value of endoscopic ultrasonography for common bile duct dilatation without identifiable etiology detected from cross-sectional imaging[J]. Clin Endosc, 2022, 55( 1): 122- 127. DOI: 10.5946/ce.2021.122. [31] MALIKOWSKI T, LEVY MJ, GLEESON FC, et al. Endoscopic ultrasound/fine needle aspiration is effective for lymph node staging in patients with cholangiocarcinoma[J]. Hepatology, 2020, 72( 3): 940- 948. DOI: 10.1002/hep.31077. [32] MOURA DTH, de MOURA EGH, MATUGUMA SE, et al. EUS-FNA versus ERCP for tissue diagnosis of suspect malignant biliary strictures: A prospective comparative study[J]. Endosc Int Open, 2018, 6( 6): E769- E777. DOI: 10.1055/s-0043-123186. [33] JO JH, CHO CM, JUN JH, et al. Same-session endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in suspected malignant biliary obstruction: A multicenter experience[J]. J Gastroenterol Hepatol, 2019, 34( 4): 799- 805. DOI: 10.1111/jgh.14528. [34] CHIANG A, THERIAULT M, SALIM M, et al. The incremental benefit of EUS for the identification of malignancy in indeterminate extrahepatic biliary strictures: A systematic review and meta-analysis[J]. Endosc Ultrasound, 2019, 8( 5): 310- 317. DOI: 10.4103/eus.eus_24_19. [35] KULPATCHARAPONG S, PITTAYANON R, KERR SJ, et al. Diagnostic performance of digital and video cholangioscopes in patients with suspected malignant biliary strictures: A systematic review and meta-analysis[J]. Surg Endosc, 2022, 36( 5): 2827- 2841. DOI: 10.1007/s00464-021-08571-2. [36] JANG S, STEVENS T, KOU L, et al. Efficacy of digital single-operator cholangioscopy and factors affecting its accuracy in the evaluation of indeterminate biliary stricture[J]. Gastrointest Endosc, 2020, 91( 2): 385- 393. e 1. DOI: 10.1016/j.gie.2019.09.015. [37] LEE YN, MOON JH, CHOI HJ, et al. Tissue acquisition for diagnosis of biliary strictures using peroral cholangioscopy or endoscopic ultrasound-guided fine-needle aspiration[J]. Endoscopy, 2019, 51( 1): 50- 59. DOI: 10.1055/a-0645-1395. [38] CHEN PT, CHANG DW, WU TH, et al. Applications of artificial intelligence in pancreatic and biliary diseases[J]. J Gastroenterol Hepatol, 2021, 36( 2): 286- 294. DOI: 10.1111/jgh.15380. [39] YAO X, HUANG X, YANG C, et al. A novel approach to assessing differentiation degree and lymph node metastasis of extrahepatic cholangiocarcinoma: Prediction using a radiomics-based particle swarm optimization and support vector machine model[J]. JMIR Med Inform, 2020, 8( 10): e23578. DOI: 10.2196/23578. [40] PENG YT, ZHOU CY, LIN P, et al. Preoperative ultrasound radiomics signatures for noninvasive evaluation of biological characteristics of intrahepatic cholangiocarcinoma[J]. Acad Radiol, 2020, 27( 6): 785- 797. DOI: 10.1016/j.acra.2019.07.029. [41] QIAN XL, ZHOU CW, WANG F, et al. Development and validation of combined Ki67 status prediction model for intrahepatic cholangiocarcinoma based on clinicoradiological features and MRI radiomics[J]. Radiol Med, 2023, 128( 3): 274- 288. DOI: 10.1007/s11547-023-01597-7. [42] ZHANG X, TANG DH, ZHOU JD, et al. A real-time interpretable artificial intelligence model for the cholangioscopic diagnosis of malignant biliary stricture(with videos)[J]. Gastrointest Endosc, 2023, 98( 2): 199- 210. e 10. DOI: 10.1016/j.gie.2023.02.026. [43] SETHI A, TYBERG A, SLIVKA A, et al. Digital single-operator cholangioscopy(DSOC) improves interobserver agreement(IOA) and accuracy for evaluation of indeterminate biliary strictures: The Monaco classification[J]. J Clin Gastroenterol, 2022, 56( 2): e94- e97. DOI: 10.1097/MCG.0000000000001321. [44] AHMAD OF, STASSEN P, WEBSTER GJ. Artificial intelligence in biliopancreatic endoscopy: Is there any role?[J]. Best Pract Res Clin Gastroenterol, 2021, 52-53: 101724. DOI: 10.1016/j.bpg.2020.101724. [45] RIBEIRO T, SARAIVA MM, AFONSO J, et al. Automatic identification of papillary projections in indeterminate biliary strictures using digital single-operator cholangioscopy[J]. Clin Transl Gastroenterol, 2021, 12( 11): e00418. DOI: 10.14309/ctg.0000000000000418. [46] PEREIRA P, MASCARENHAS M, RIBEIRO T, et al. Automatic detection of tumor vessels in indeterminate biliary strictures in digital single-operator cholangioscopy[J]. Endosc Int Open, 2022, 10( 3): E262- E268. DOI: 10.1055/a-1723-3369. -

 下载:
下载:

 本文二维码
本文二维码
图(3)
计量
- 文章访问数: 1313
- HTML全文浏览量: 1029
- PDF下载量: 338
- 被引次数: 0

