
 PDF下载 ( 6486 KB)
PDF下载 ( 6486 KB)

不同运动干预对代谢相关脂肪性肝病患者的影响:系统评价与网状Meta分析
DOI: 10.12449/JCH260213
Effect of different exercise interventions on patients with metabolic dysfunction-associated fatty liver disease: A systematic review and network Meta-analysis
-
摘要:
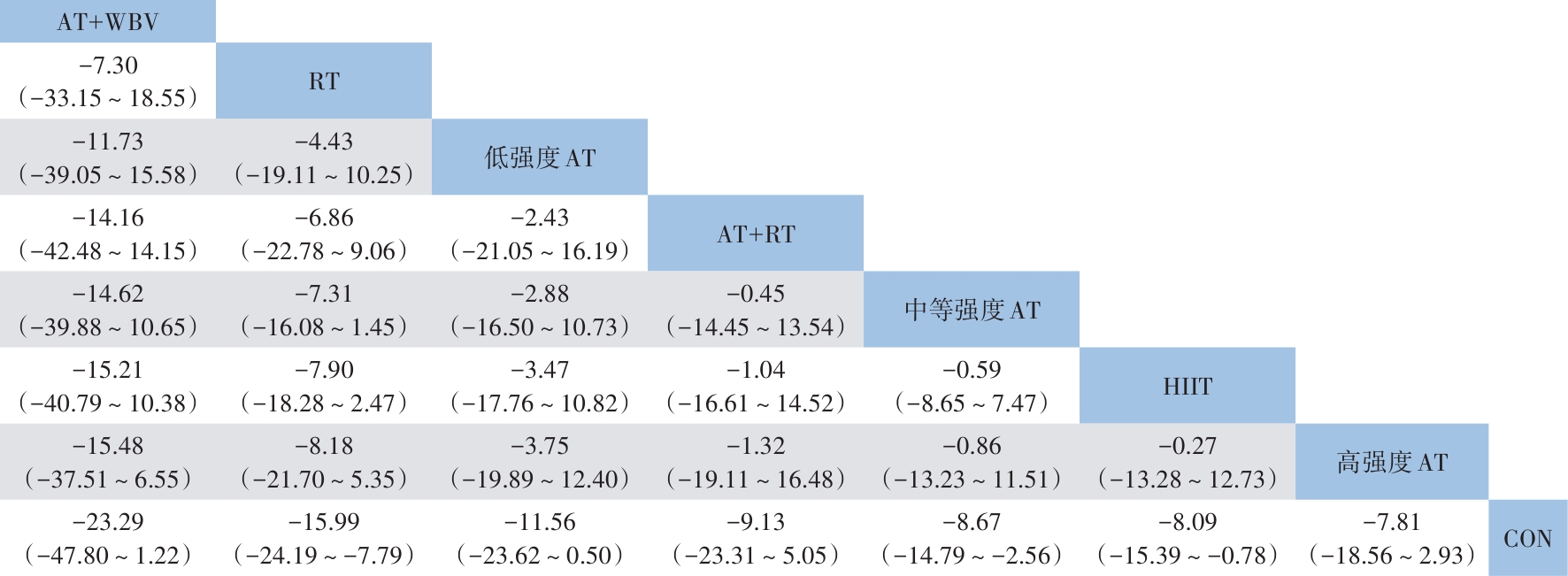
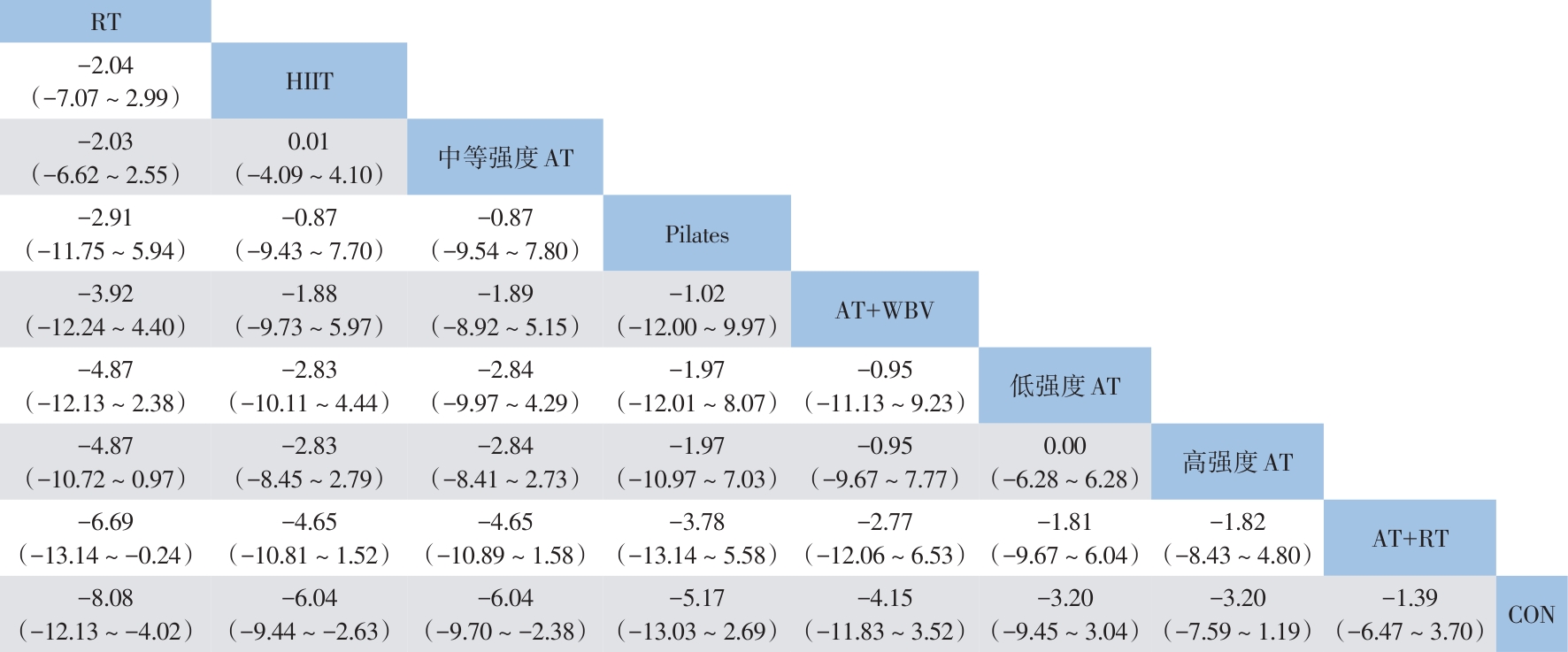
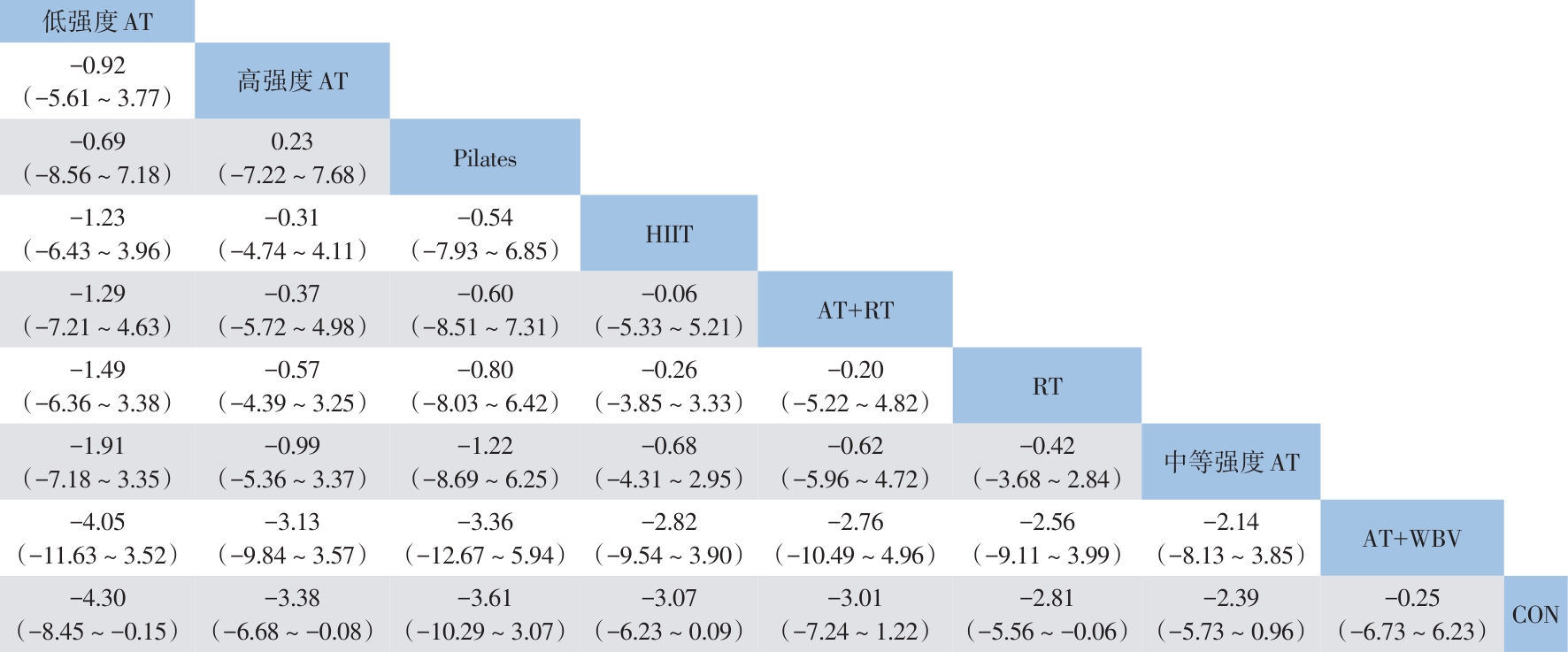
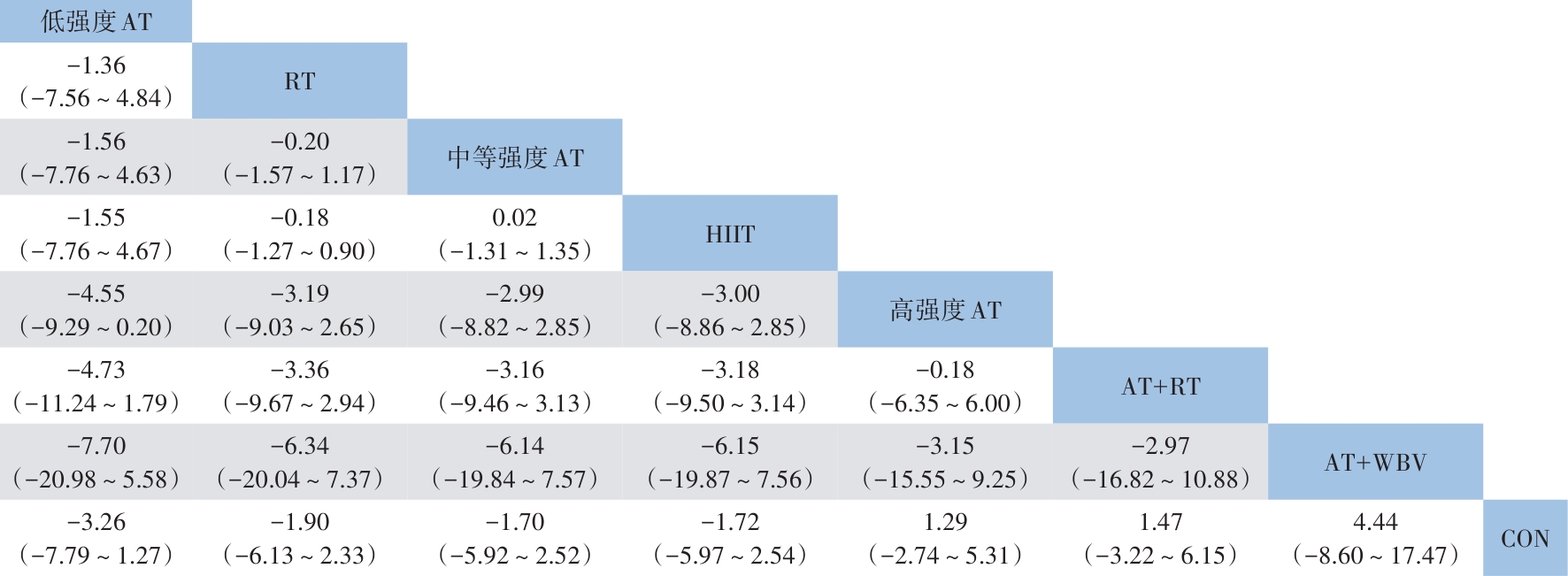
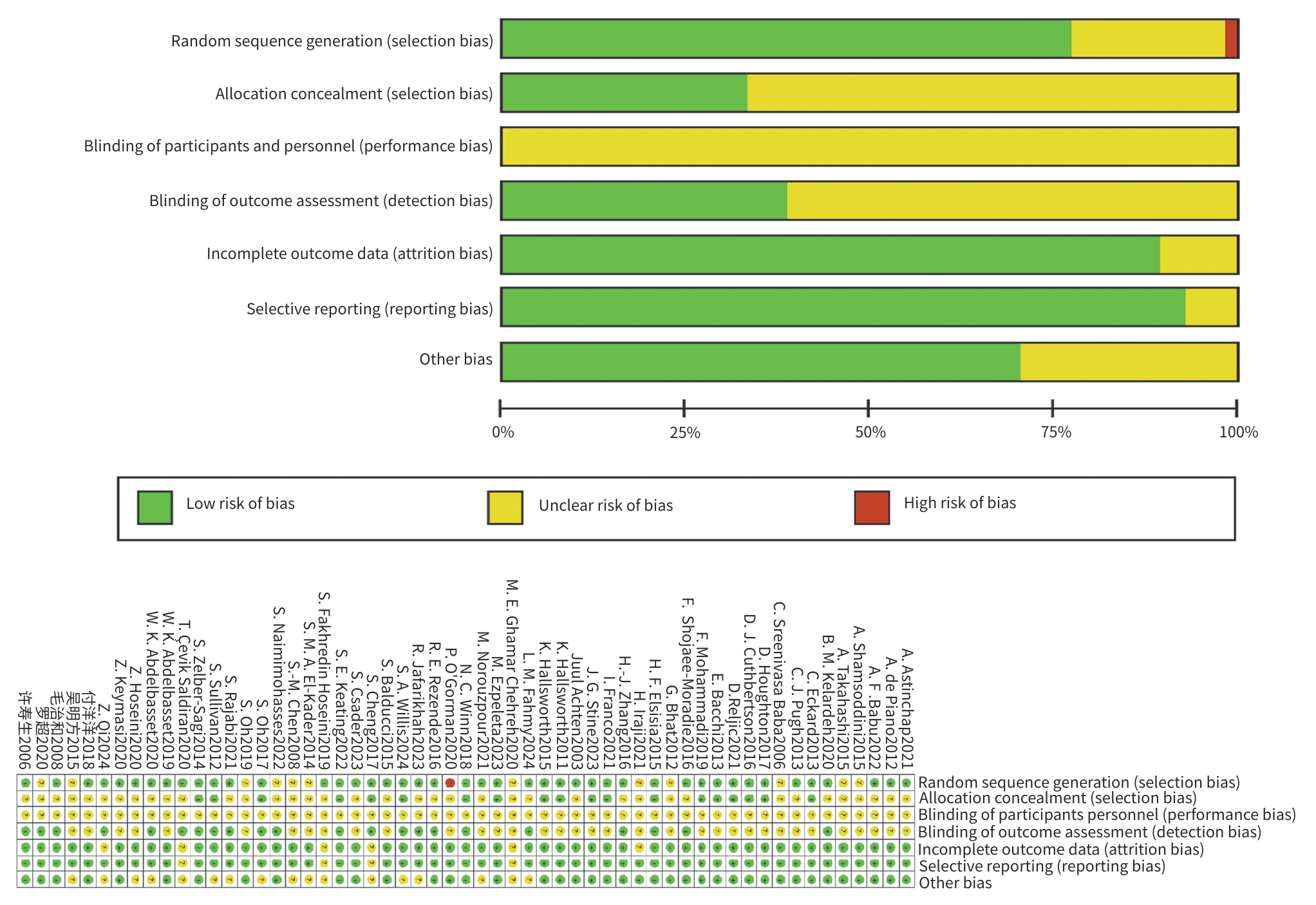
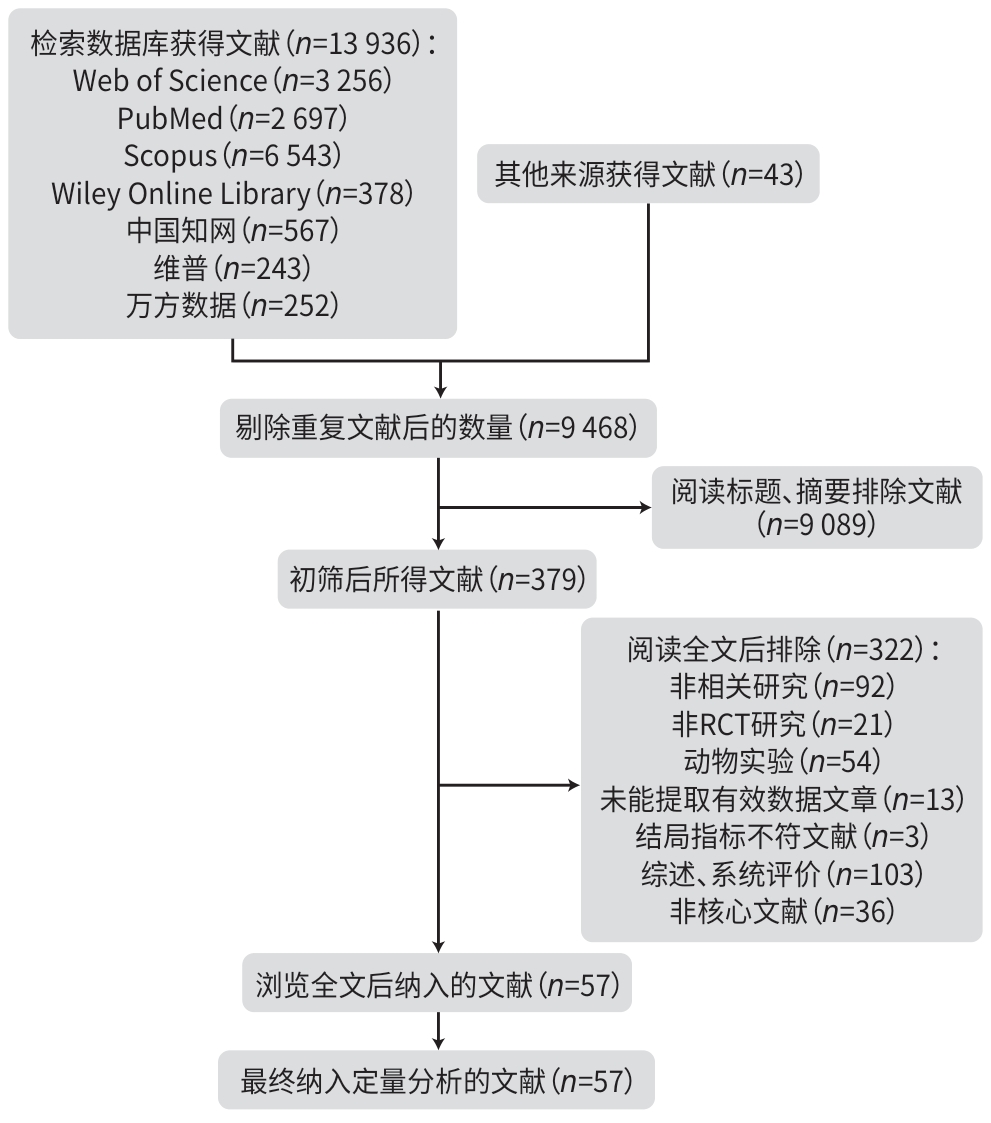
目的 系统评价不同运动干预对代谢相关脂肪性肝病(MAFLD)患者代谢与肝脏指标的影响,为临床运动康复提供循证建议。 方法 依据PRISMA指南开展研究,方案已在PROSPERO平台注册(注册号:CRD42025641717)。检索PubMed、Web of Science、Scopus、Wiley Online Library、中国知网、万方数据、维普等数据库中自建库至2024年9月发表的相关文献,采用Cochrane偏倚风险评估工具评价文献质量,并运用Stata MP 17.0软件进行网状Meta分析。 结果 共 纳入57篇文献,涉及2 648例患者。结果显示,有氧联合抗阻运动在改善体重指数(BMI)[加权均数差(WMD)=-0.97,95%置信区间(CI):-1.66~-0.28,P<0.05,累积排序概率曲线下面积(SUCRA)=85.4]与甘油三酯(WMD=-29.6,95%CI:-46.66~12.54,P<0.05,SUCRA=87.3)方面效果最优;抗阻运动为改善总胆固醇(WMD=-15.99,95%CI:-24.19~-7.79,P<0.05,SUCRA=79.9)和丙氨酸氨基转移酶(WMD=-8.08,95%CI:-12.13~-4.02,P<0.05,SUCRA=87.3)的最优干预方式;低强度有氧运动在改善天冬氨酸氨基转移酶(WMD=-4.3,95%CI:-8.45~-0.15,P<0.05,SUCRA=73.5)、γ-谷氨酰转移酶(WMD=-3.26,95%CI:-7.79~1.27,P>0.05,SUCRA=82.3)、糖化血红蛋白(WMD=-0.6,95%CI:-2.02~0.82,P>0.05,SUCRA=78.8)方面效果最优;中等强度有氧运动则为改善胰岛素抵抗指数(WMD=-0.92,95%CI:-1.51~-0.33,P<0.05,SUCRA=69.4)的最优干预方式。需注意的是,糖化血红蛋白与γ-谷氨酰转移酶的各项运动干预均未呈现统计学差异(P值均>0.05),提示目前尚无足够统计学证据支持运动能够改善上述两项指标。 结论 有氧联合抗阻运动、抗阻运动以及低、中强度有氧运动可能是改善MAFLD患者关键指标的最佳运动方式,针对不同指标可选用针对性的运动方式进行干预,但受原始研究限制,以上结论仍需进一步验证与探究。 Abstract:Objective To investigate the effect of different exercise interventions on metabolism and liver parameters in patients with metabolic dysfunction-associated fatty liver disease (MAFLD), and to provide evidence-based recommendations for clinical exercise rehabilitation. Methods This study was conducted according to the PRISMA guidelines, and the protocol was registered on the PROSPERO platform, with a registration number of CRD42025641717. PubMed, Web of Science, Scopus, Wiley Online Library, CNKI, Wanfang Data, and VIP were searched for related articles published up to September 2024. The Cochrane tool for assessing risk of bias was used to assess the quality of articles, and Stata MP 17.0 was used to perform the network meta-analysis. Results A total of 57 articles were included, involving 2 648 patients. The results showed that aerobic exercise combined with resistance exercise had the best effect in improving body mass index (mean difference [WMD]=-0.97, 95% confidence interval [CI]: -1.66 to -0.28], P<0.05, surface under the cumulative ranking curve [SUCRA]=85.4) and triglycerides (WMD=-29.6, 95%CI: -46.66 to 12.54, P<0.05, SUCRA=87.3); resistance exercise was the optimal intervention method for improving total cholesterol (WMD=-15.99, 95%CI: -24.19 to -7.79, P<0.05, SUCRA=79.9) and glutamine transaminase (WMD=-8.08, 95%CI: -12.13 to -4.02, P<0.05, SUCRA=87.3); low-intensity aerobic exercise had the best effect in improving aspartate aminotransferase (WMD=-4.3, 95%CI: -8.45 to -0.15, P<0.05, SUCRA=73.5), gamma-glutamyl transpeptidase (GGT) (WMD=-3.26, 95%CI: -7.79 to 1.27, P>0.05, SUCRA=82.3), and glycated hemoglobin (HbA1c) (WMD=-0.6, 95%CI: -2.02 to 0.82, P>0.05, SUCRA=78.8); moderate-intensity aerobic exercise was the optimal intervention modality to improve Homeostasis Model Assessment of Insulin Resistance (WMD=-0.92, 95%CI: -1.51 to -0.33, P<0.05, SUCRA=69.4). It should be noted that there were no significant differences in HbA1c and GGT across different exercise interventions (all P>0.05), suggesting that there was currently no sufficient statistical evidence to support that exercise could improve these two indicators. Conclusion Based on the comprehensive league table and cumulative probability ranking, aerobic exercise combined with resistance exercise, resistance exercise, and low- and moderate-intensity aerobic exercise may be the best exercise modality for improving key indicators in MAFLD patients, and targeted exercise modalities should be selected for intervention against different indicators; however, due to limitations of the original studies, further studies are needed for validation and exploration. -
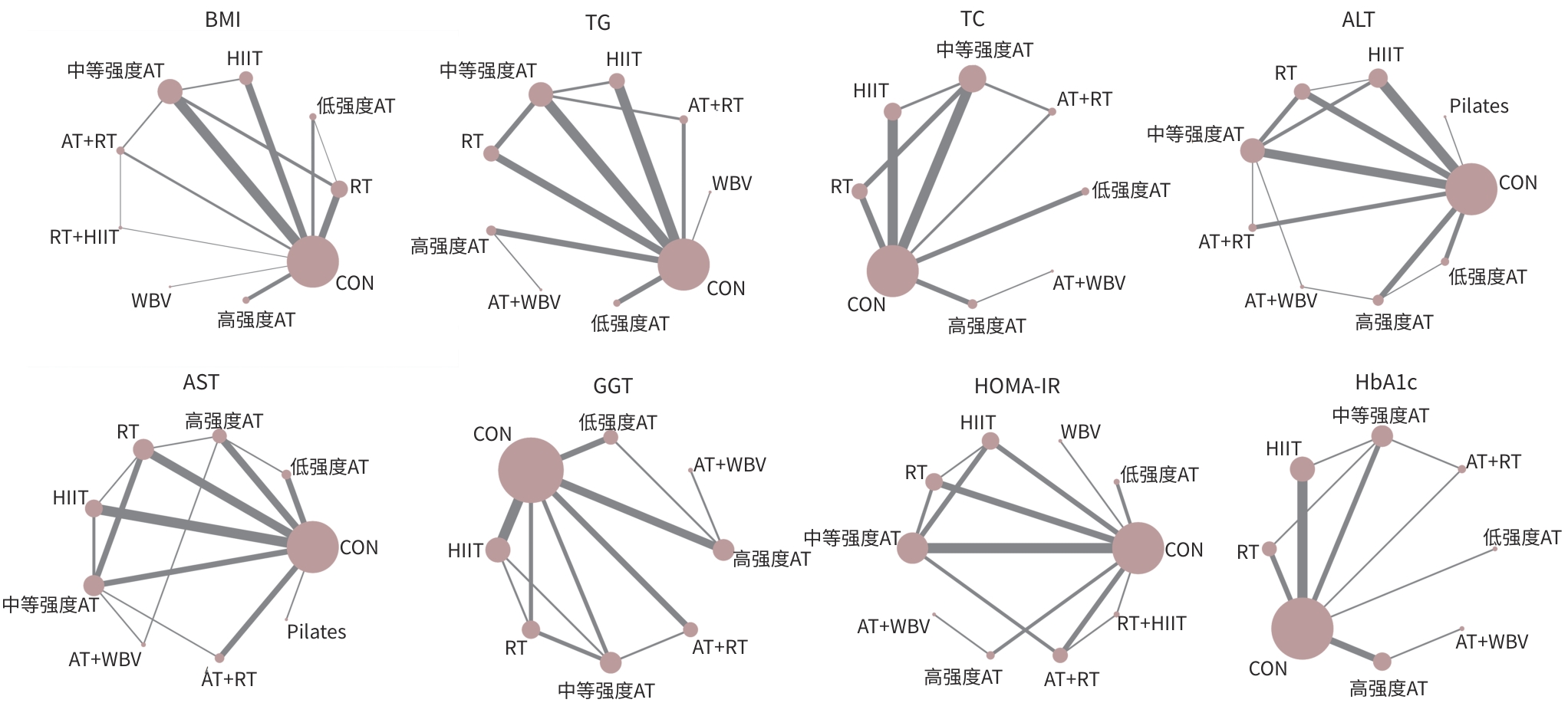
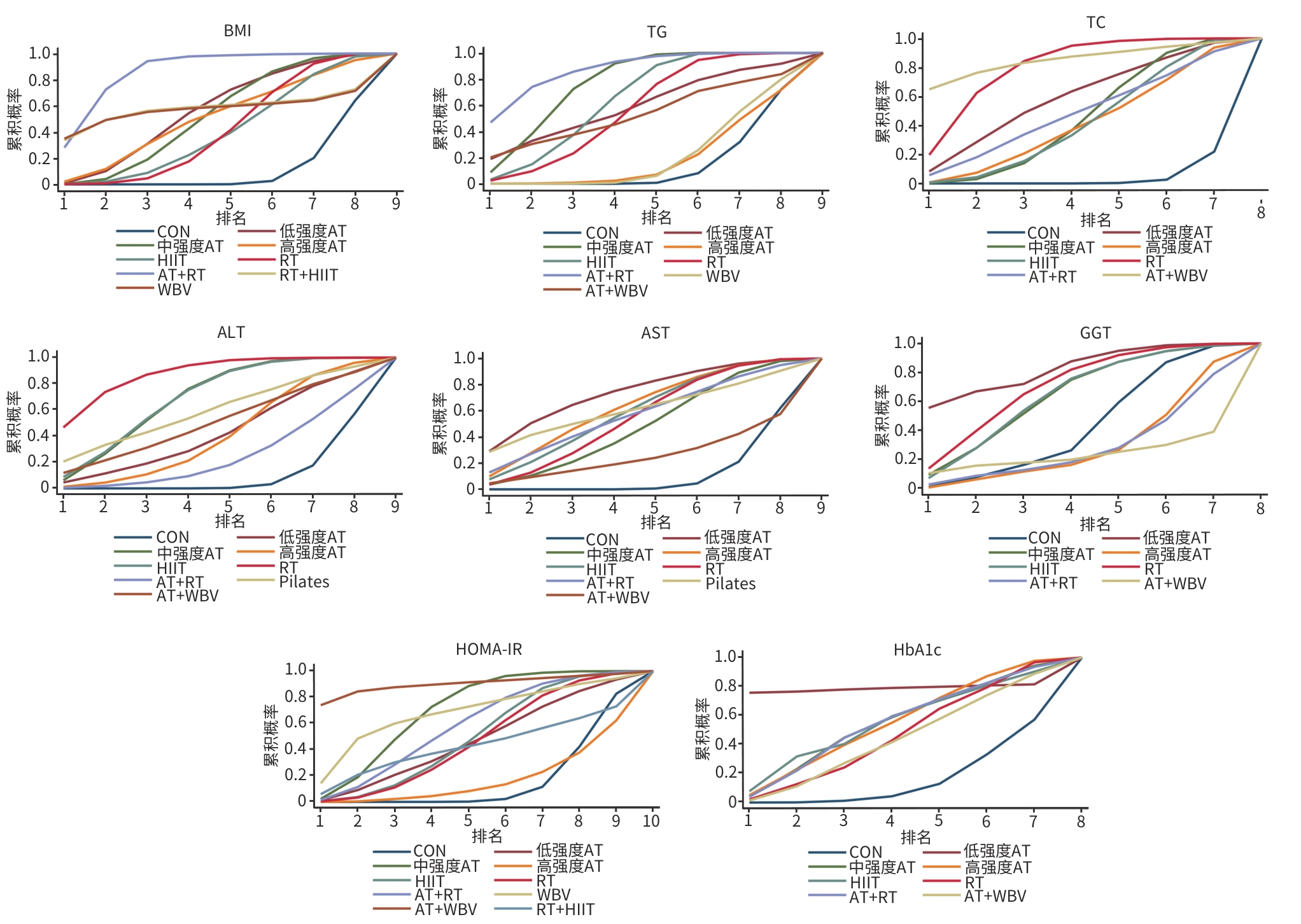
注: AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;Pilates,普拉提训练;CON,对照组;BMI,体重指数;TG,甘油三酯;TC,总胆固醇;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;GGT,γ-谷氨酰转移酶;HOMA-IR,稳态模型评估胰岛素抵抗指数;HbA1c,糖化血红蛋白。
图 3 各指标证据网络图
Figure 3. Evidence network diagram for each indicator
注: AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;Pilates,普拉提训练;CON,对照组;BMI,体重指数;TG,甘油三酯;TC,总胆固醇;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;GGT,γ-谷氨酰转移酶;HOMA-IR,稳态模型的胰岛素抵抗指数;HbA1c,糖化血红蛋白。
图 5 各指标改善效果优劣排序
Figure 5. Ranking of the improvement effects of each indicator
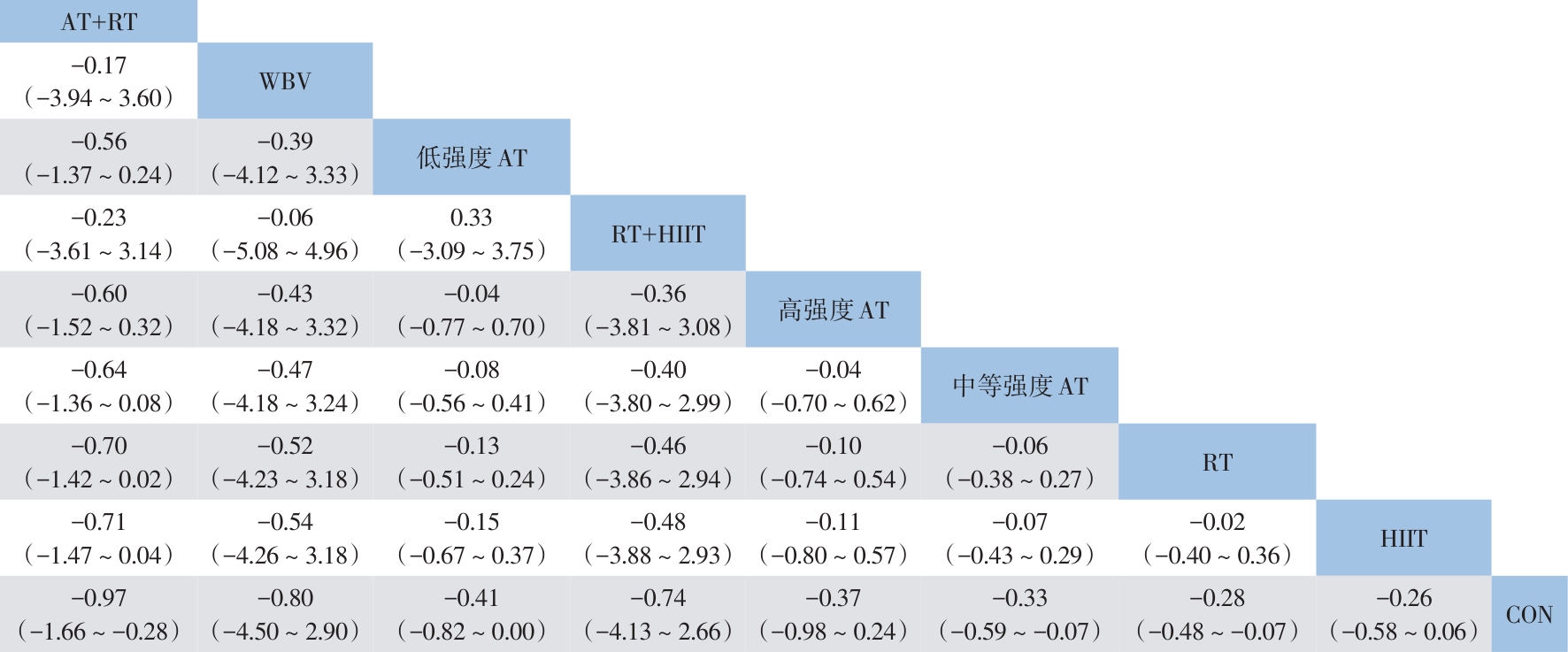
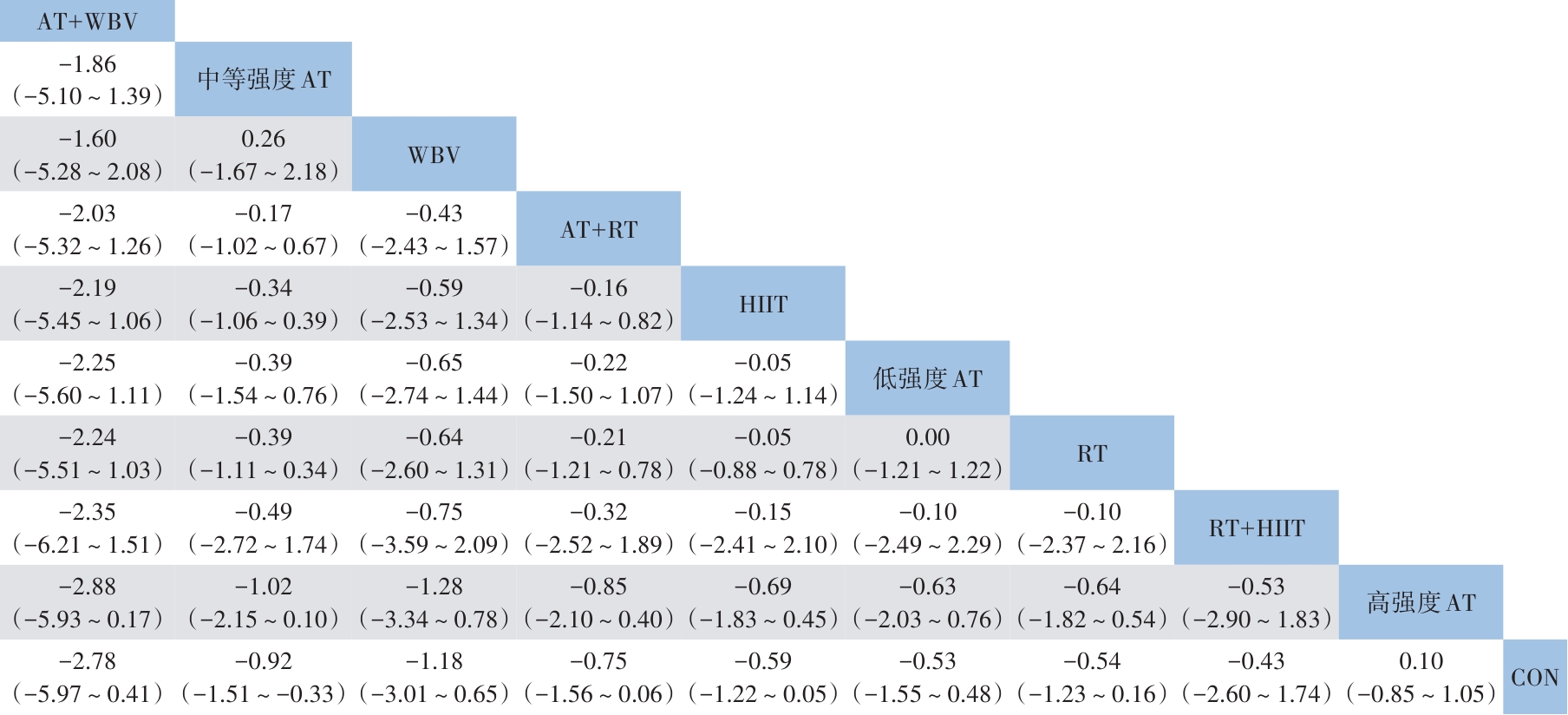
注: MAFLD,代谢相关脂肪性肝病;BMI,体重指数;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;CON,对照组。
图 4 不同运动干预MAFLD患者BMI效果的联赛表
Figure 4. League table of the effect of different exercise interventions on BMI in patients with MAFLD
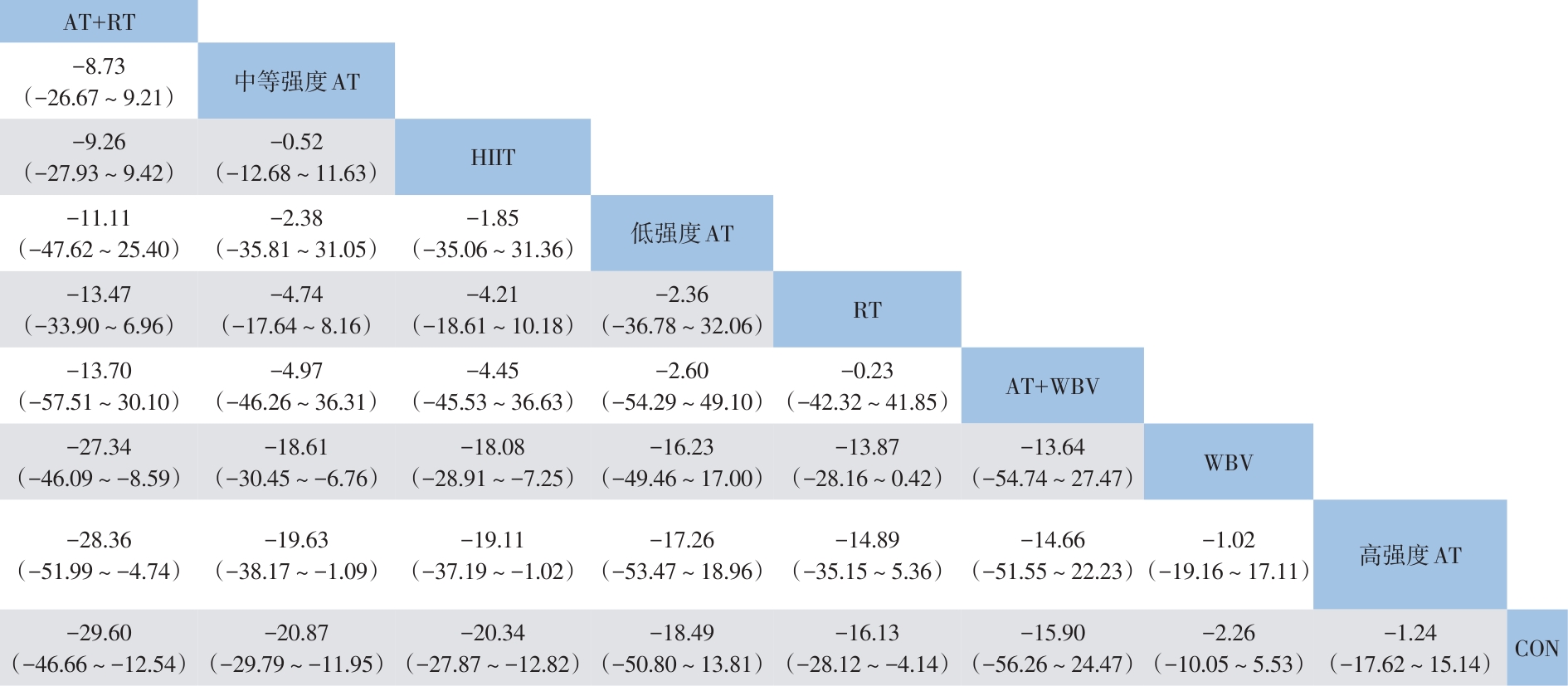
注: MAFLD,代谢相关脂肪性肝病;TG,甘油三酯;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;CON,对照组。
图 6 不同运动干预MAFLD患者TG效果的联赛表
Figure 6. League table of the effect of different exercise interventions on TG in patients with MAFLD
注: MAFLD,代谢相关脂肪性肝病;TC,总胆固醇;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;Pilates,普拉提训练;CON,对照组。
图 7 不同运动干预MAFLD患者TC效果的联赛表
Figure 7. League table of the effect of different exercise interventions on TC in patients with MAFLD
注: MAFLD,代谢相关脂肪性肝病;ALT,丙氨酸氨基转移酶;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;Pilates,普拉提训练;CON,对照组。
图 8 不同运动干预MAFLD患者ALT效果的联赛表
Figure 8. League table of the effect of different exercise interventions on ALT in patients with MAFLD
注: MAFLD,代谢相关脂肪性肝病;AST,天冬氨酸氨基转移酶;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;Pilates,普拉提训练;CON,对照组。
图 9 不同运动干预MAFLD患者AST效果的联赛表
Figure 9. League table of the effect of different exercise interventions on AST in patients with MAFLD
注: MAFLD,代谢相关脂肪性肝病;GGT,γ-谷氨酸氨基转移酶;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;CON,对照组。
图 10 不同运动干预MAFLD患者GGT效果的联赛表
Figure 10. League table of the effect of different exercise interventions on GGT in patients with MAFLD
注: MAFLD,代谢相关脂肪性肝病;HOMA-IR,稳态模型评估胰岛素抵抗指数;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;CON,对照组。
图 11 不同运动干预MAFLD患者HOMA-IR效果的联赛表
Figure 11. League table of the effect of different exercise interventions on HOMA-IR in patients with MAFLD
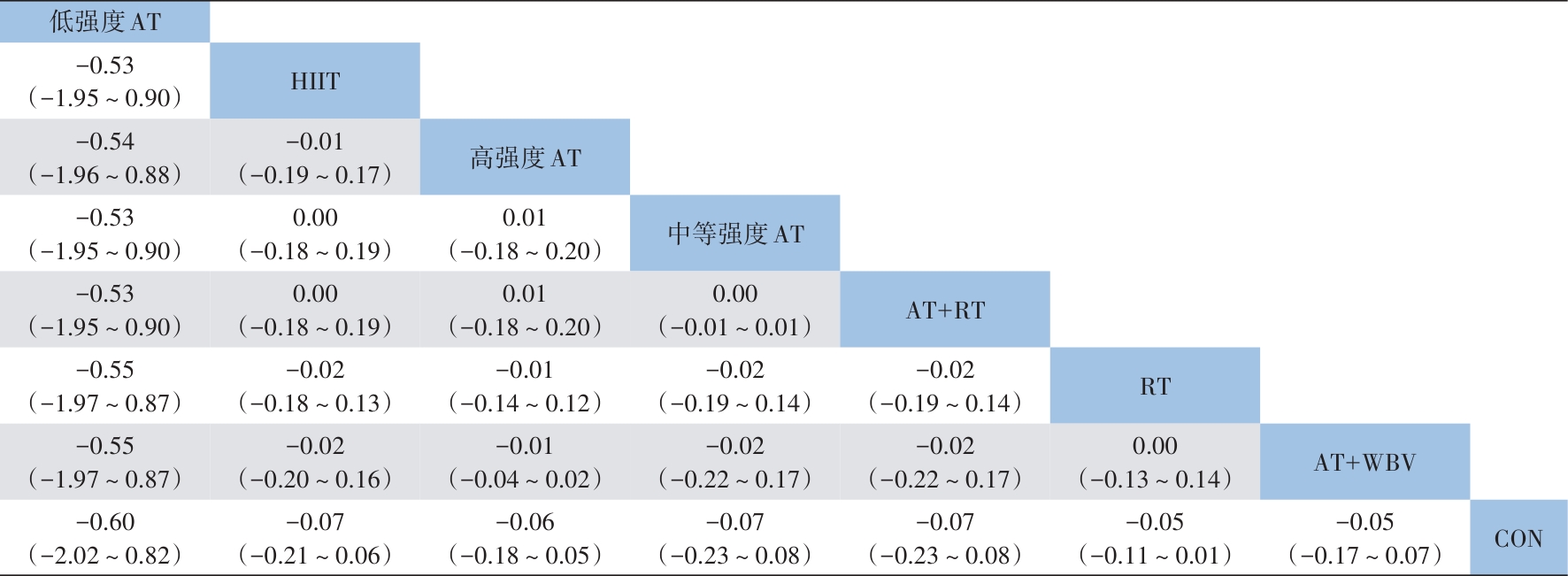
注: MAFLD,代谢相关脂肪性肝病;HbA1c,糖化血红蛋白;AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;CON,对照组。
图 12 不同运动干预MAFLD患者HbA1c效果的联赛表
Figure 12. League table of the effect of different exercise interventions on HbA1c in patients with MAFLD
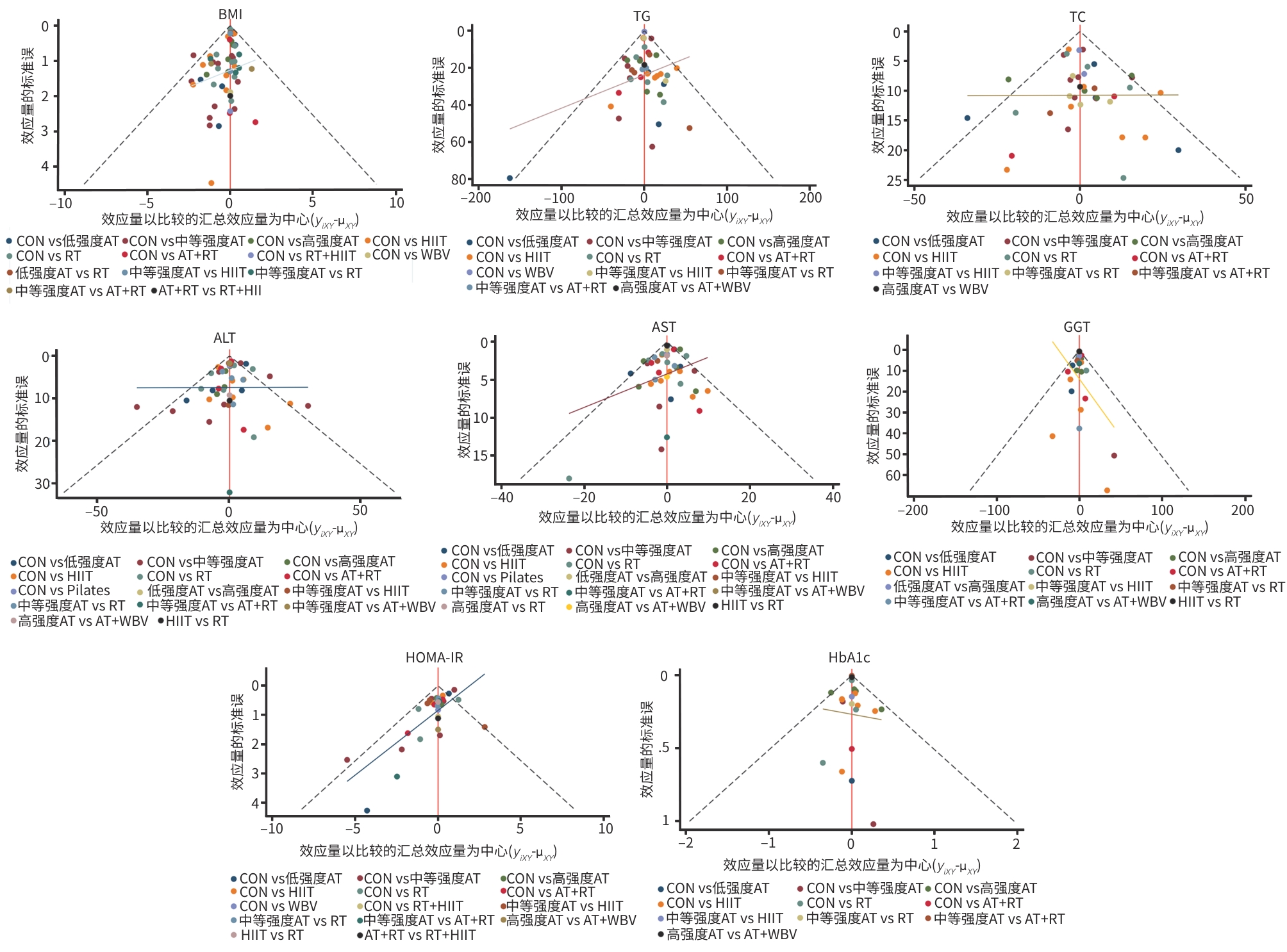
注: AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇运动;WBV,全身振动训练;Pilates,普拉提训练;CON,对照组;BMI,体重指数;TG,甘油三酯;TC,总胆固醇;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;GGT,γ-谷氨酰转移酶;HOMA-IR,稳态模型评估胰岛素抵抗指数;HbA1c,糖化血红蛋白。
图 13 各指标发表偏倚检验图
Figure 13. Plot of publication bias test for each indicator
表 1 PubMed检索策略示例
Table 1. Search strategy using PubMed as an example
检索步骤 检索式 #1 ("fatty liver"[Title/Abstract]) OR ("Non-alcoholic fatty liver disease"[Title/Abstract]) OR ("steatohpatitis"[Title/
Abstract]) OR ("nonalcoholic steatohepatitis"[Title/Abstract]) OR ("steatosis of liver"[Title/Abstract])) OR ("liver
steatosis"[Title/Abstract]) OR ("NAFLD"[Title/Abstract]) OR ("MAFLD"[Title/Abstract]) OR ("MASLD"[Title/
Abstract])#2 ("exercise"[Title/Abstract]) OR ("training"[Title/Abstract]) OR ("aerobic exercise"[Title/Abstract]) OR ("aerobic
training"[Title/Abstract]) OR ("moderate intensity continuous training"[Title/Abstract]) OR ("resistance training"
[Title/Abstract]) OR ("resistance exercise"[Title/Abstract]) OR ("strength training"[Title/Abstract]) OR
("concurrent training"[Title/Abstract]) OR ("high intensity interval training"[Title/Abstract]) OR ("blood flow
restriction"[Title/Abstract]) OR ("moderate intensity continuous training"[Title/Abstract]) OR ("physical activity"
[Title/Abstract])#3 #1 AND #2  下载: 导出CSV
下载: 导出CSV
表 2 纳入文献基本特征
Table 2. Basic characteristics of the included literature
第一作者(发表年) 干预措施 样本量
(例)年龄(岁) 运动强度 干预周期(周)/
频率(次)结局指标 Astinchap[10](2021年) 51±8 8/3 ①②③⑦ AT 15 30~45 min,60%~75%HRmax RT 15 35~50 min,50~70%1RM CON 15 — de Piano[16](2012年) 16.48±1.42 52/3 ①②③④⑤⑥⑦ AT 14 60 min,50%~70%VO2max AT+RT 14 30 minAT;30 min RT Babu[17](2022年) 12/2 ①②③④⑤⑥⑧ HIIT 20 59.9±9.8 40%~50 min,85%HRmax,间歇
2~4 minCON 22 56.7±10.7 — Shamsoddini[18](2015年) 8/3 ①④⑤ AT 10 39.7±6.3 45 min,60%~75%HRmax RT 10 45.9±7.3 45 min,50%~70%1RM CON 10 45.8±7.3 — Takahashi[19](2015年) 12/3 ①②④⑤⑥⑦⑧ RT 31 55.5±13.2 3组,1组各10次俯卧撑,深蹲 CON 22 51.4±14.8 — Kelardeh[20](2020年) 12/3 ① RT 12 65.91±3.31 60~70 min,40%~95%1RM CON 11 64.36±2.97 — Eckard[21](2013年) 26/4~7 ④⑤ AT 9 52±10 20~60 min,中等强度 CON 11 51±11 — Pugh[22](2013年) 16/3~5 ①②③④⑤⑥ AT 6 50±11.05 30~45 min,30%~60%HRmax CON 5 48±12.85 标准护理 Baba[23](2006年) 12/5 ①④⑤ AT 16 36.5±8.6 45 min,60%~70%HRmax CON 15 45.2±9.4 — Houghton[24](2017年) 12/3 ①②③④⑤⑥⑦⑧ AT+RT 12 54±12 45~60 min,固定自行车(16~
18RPE),RT(14~16RPE)CON 12 51±16 标准护理 Cuthbertson[25](2016年) 16/3~5 ①②③④⑤⑥⑦ AT 30 52±16.74 30~45 min,30%~60%HRmax CON 20 52.5±14.86 — Reljic[26](2021年) 12/2 ①②③④⑤⑥⑧ HIIT 29 52.1±9.6 14 min,80%~95%HRmax,间歇
1~3 minCON 17 56.7±9.8 标准护理 Bacchi[11](2013年) 16/3 ①②③④⑤⑥⑧ AT 13 55.6±2 60 min,60%~65%HRmax RT 17 56±1.9 70%~80%1RM Mohammadi[27](2019年) 12/3 ①④⑤ RT 10 37.3±2.87 40%~80%1RM CON 10 31.7±3.07 — Moradie[28](2016年) 16/4~5 ①②③④⑤⑥ AT+RT 15 52.4±2.2 20~60 min,40%~60%HRmax CON 12 52.8±3 —
下载: 导出CSV
表 2 (续)
Table 2. (continued)
第一作者(发表年) 干预措施 样本量
(例)年龄(岁) 运动强度 干预周期(周)
/频率(次)结局指标 Bhat[29](2012年) 26/5 ①④⑦ AT 12 40.1±9 45 min,70%HRmax CON 15 39.6±8.9 — Elsisia[30](2015年) 12/3 ①②③④⑤ AT 16 44.64±11.4 20~30 min,60%~75% HRmax RT 16 43.32±10.32 30 min,60%~80%1RM Iraji[31](2021年) 8/3 ① HIIT 11 12.81±1.02 36~40 min,100%~110%MAS,
间歇4 minCON 12 13.14±1.49 — Zhang[32](2016年) 26/5 ④⑤⑥ AT 68 53.2±7.1 30 min,65%~80% HRmax AT 69 54.4±7.4 30 min,45%~55% HRmax CON 74 54±6.8 — Franco[33](2020年) 12/3 ①②③⑦⑧ AT 25 50.45±9.45 50~60 min,60%~75% HRmax AT+RT 23 46.23±9.39 45 minAT;3组12项RT Stine[34](2023年) 20/5 ①②③④⑤⑦⑧ AT 12 54.65±15.81 30 min,45%~55% VO2max CON 8 45.9±13.14 标准护理 Achten[35](2003年) 12/3~5 ①②③ AT 4 42±5 30~60 min,55%~65% HRmax CON 5 43±4 — Hallsworth[36](2011年) 8/3 ①②③④⑦⑧ RT 11 52±13.3 45~60 min,50%~70% HRmax CON 8 62±7.4 标准护理 Hallsworth[37](2015年) 12/3 ①②③④⑤⑥⑦⑧ HIIT 11 54±10 30~40 min,16~17RPE,间歇
3 minCON 12 52±12 标准护理 Fahmy[38](2024年) 12/3 ④⑤ AT 30 40.8±3.4 65 min,60%~75% HRmax AT+WBV 30 41.07±3.3 45 minAT;30~40 minWBV Chehreh[39](2020年) 8/3 ① RT 15 未说明 60 min,50%~70%1RM CON 12 未说明 — Ezpeleta[40](2023年) 12/5 ①②③④⑤⑧ AT 15 44±13 60 min,65%~80% HRmax CON 20 44±12 — Norouzpour[41](2021年) 10/3 ②④⑤⑦ AT+RT 10 56.1±3.21 15~30 min,50%~75% HRmax
(AT);45 min,50%~75%1RM
(RT)CON 12 56.25±5.62 — Winn[42](2018年) 4/4 ①②③④⑤⑦ AT 8 46±9 60 min,55% VO2max HIIT 8 41±14 80% VO2max,间歇3 min CON 5 51±13 — O’Gorman[43](2020年) 12/3~5 ①②③④⑤⑥⑧ AT 16 61±15 21~42 min,40%~75% HRmax CON 8 58±23 标准护理
下载: 导出CSV
表 2 (续)
Table 2. (continued)
第一作者(发表年) 干预措施 样本量
(例)年龄(岁) 运动强度 干预周期(周)/
频率(次)结局指标 Rezende[44](2016年) 24/2 ①②③④⑤⑥⑦⑧ AT 19 56.2±7.8 30~50 min,高强度有氧 CON 21 54.5±8.9 — Jafarikhah[45](2023年) 8/3 ①②③④⑤ RT 8 48.6±2.51 60 min,12~14RPE CON 8 46.2±5.4 — Willis[46](2024年) 6/4 ①③④⑤⑥⑦⑧ AT 11 61±17 35~50 min,70%~75% HRmax CON 13 63±18 — Balducci[12](2015年) 52/2 ④⑤⑥ AT+RT 288 未说明 55%~70% VO2max;60%1RM CON 275 未说明 — Cheng[47](2017年) 38/2~3 ②④⑤⑥⑧ AT 22 59±4.4 30~60 min,60%~75% VO2max CON 18 60±3.4 — Csader[48](2023年) 12/2 ①②③④⑤⑥⑧ HIIT 7 56.9±12.2 5组2~4 min,85% VO2max,间歇
3 minCON 7 61.3±7.1 — Keating[49](2023年) 12/3 ①②③④⑤⑥ HIIT 7 53±12 4组4 min,85%~95% HRmax,间
歇3 minCON 5 61±5 拉伸 Hoseini[50](2019年) 8/3 ①④⑤ HIIT 17 39.82±5.21 基于RAST测试的HIIT训练 CON 13 38.69±6.7 — EL-Kader[51](2014年) 12/3 ④⑤ AT 25 50.87±5.93 40 min,60%~80% HRmax RT 25 51.12±5.58 40 min,8~12组,60%~
80%1RMChen[52](2008年) 10/2 ①②③④⑤⑥⑦ AT 23 36±6.9 60 min,高强度自行车 CON 15 37.7±6.6 — Naimimohasses[53](2022年) 12/3~5 ① AT 16 61±15 30~60 min,40%~75% HRmax CON 14 55±20 — Oh[54](2017年) 12/3 ④⑤⑥⑦ AT 13 48.2±2.3 40 min,60%~65% VO2max HIIT 20 48.6±1.8 3组,80%~85% VO2max,间歇
2 minRT 19 51.2±1.9 3~5组,40%~60%1RM Oh[55](2019年) 26/2 ①②⑦ WBV 25 54.2 20 min,30~50 Hz CON 17 48.4 — Rajabi[56](2021年) 12/3 ①⑦ AT+RT 11 44.45±6.47 16~30 min,70%~75% HRmax;
20~30 min,60%~75%1RMRT+HIIT 11 42.09±9.04 8~13 min,85%~95 %HRmax;
20~30 min,60%~75%1RMCON 11 43.82±7.53 —
下载: 导出CSV
表 2 (续)
Table 2. (continued)
第一作者(发表年) 干预措施 样本量
(例)年龄(岁) 运动强度 干预周期(周)/
频率(次)结局指标 Sullivan[57](2012年) 16/5 ①②③④ AT 12 48.6±2.2 30~60 min,45%~55% VO2max CON 6 47.5±3.1 — Zelber-Sagi[58](2014年) 12/3 ①②③④⑤⑥⑦⑧ RT 33 46.32±10.32 40 min,10~12RPE CON 31 46.64±11.4 拉伸 Çevik Saldiran[59](2020年) 8/3 ②③④⑤⑥⑦⑧ AT 16 43.75±8.62 40 min,60%~80%HRmax AT+WBV 15 45.07±9.11 40 min,60%~80%HRmax;
15 min,30 HzAbdelbasset[60](2019年) 8/3 ①②③④⑦⑧ HIIT 16 54.4±5.8 40 min,80%~85%VO2max,
间歇2 minCON 16 55.2±4.3 — Abdelbasset[61](2020年) 8/3 ①②③④⑦⑧ AT 15 54.9±4.7 40~50 min,60%~70%HRmax HIIT 16 54.4±4.8 3组4 min,80%~85% VO2max,
间歇2 minCON 16 55.2±4.3 — Hoseini[62](2020年) 8/3 ①②③⑦ AT 10 62.6±1.89 45~60 min,60%~75% HRmax CON 10 62±1.88 — Keymasi[63](2020年) 8/3 ④⑤ Pilates 10 41.67±5.62 60 min,50%~80% HRmax CON 10 39.3±4.64 — Qi[64](2024年) 34/2~3 ①⑧ AT 29 59±4.4 30~60 min,60%~75% VO2max CON 29 60±3.4 — 付洋洋[65](2018年) 16/3 ①②③ AT 28 61.18±7.53 60 min,60%~70% HRmax RT 27 55.9±12.3 60 min,60%~80%1RM CON 30 58.16±9.8 — 吴明方[66](2015年) 16/4~5 ①②⑦ AT 13 54.2±3.1 40~60 min,60%~75% HRmax CON 13 55.8±3.2 — 毛治和[67](2008年) 12/3 ②③ AT 30 42.1±4.6 30~60 min,60%~80% HRmax CON 30 43.4±5.9 — 罗超[68](2020年) 12/3 ②③④⑤ HIIT 26 29.69±7.77 60 min,85%~95% HRmax CON 25 30.96±7.15 — 许寿生[69](2006年) 12/4~5 ②③ AT 42 51.93±7.68 20~60 min,50%~70% HRmax CON 29 49.17±8.71 — 注:AT,有氧运动;RT,抗阻运动;HIIT,高强度间歇训练;WBV,全身振动训练;Pilates,普拉提运动;CON,对照组;%HRmax,最大心率百分比;VO2max,最大摄氧量;1RM,一次重复最大重量;RPE,主观用力感知等级;MAS,最大有氧速度;—,无干预。结局指标:①体重指数;②甘油三酯;③总胆固醇;④丙氨酸氨基转移酶;⑤天冬氨酸氨基转移酶;⑥γ-谷氨酰转移酶;⑦稳态模型评估胰岛素抵抗指数;⑧糖化血红蛋白。
下载: 导出CSV
-
[1] ZHOU XD, TIAN N, ZHENG MH. Excerpt of an international multidisciplinary consensus statement on MAFLD and the risk of CVD(2023)[J]. J Clin Hepatol, 2023, 39( 10): 2336- 2339. DOI: 10.3969/j.issn.1001-5256.2023.10.010.周晓东, 田娜, 郑明华.《2023年国际多学科专家共识: 代谢相关脂肪性肝病和心血管疾病风险》摘译[J]. 临床肝胆病杂志, 2023, 39( 10): 2336- 2339. DOI: 10.3969/j.issn.1001-5256.2023.10.010. [2] KONG JN, ZHANG BB, SHI JP. An excerpt of clinical practice guideline of prevention and treatment of metabolic dysfunction-associated(non-alcoholic) fatty liver disease(2024 edition)[J]. J Clin Hepatol, 2024, 40( 9): 1767- 1770. DOI: 10.12449/JCH240908.孔嘉宁, 张彬彬, 施军平.《代谢相关(非酒精性)脂肪性肝病防治指南(2024年版)》解读[J]. 临床肝胆病杂志, 2024, 40( 9): 1767- 1770. DOI: 10.12449/JCH240908. [3] YOUNOSSI ZM, GOLABI P, PAIK JM, et al. The global epidemiology of nonalcoholic fatty liver disease(NAFLD) and nonalcoholic steatohepatitis(NASH): A systematic review[J]. Hepatology, 2023, 77( 4): 1335- 1347. DOI: 10.1097/HEP.0000000000000004. [4] QIN L, WU JR, LIU YQ, et al. Nonalcoholic fatty liver disease is a risk factor for cardiovascular disease[J]. Sci Sin Vitae, 2024, 54( 11): 2154- 2166. DOI: 10.1360/SSV-2024-0098.秦莉, 伍俊儒, 刘雨晴, 等. 非酒精性脂肪肝病是心血管疾病危险因素[J]. 中国科学: 生命科学, 2024, 54( 11): 2154- 2166. DOI: 10.1360/SSV-2024-0098. [5] ZHANG Y, WEN L, DING SZ. Mechanisms in exercise intervening NAFLD: Mitohormesis of ROS-induced UPRmt[J]. China Sport Sci, 2022, 42( 7): 74- 84. DOI: 10.16469/j.css.202207007.张媛, 文立, 丁树哲. 运动干预NAFLD的分子机制研究述评: 基于ROS调节UPRmt的线粒体毒性兴奋效应[J]. 体育科学, 2022, 42( 7): 74- 84. DOI: 10.16469/j.css.202207007. [6] PAIK JM, KABBARA K, EBERLY KE, et al. Global burden of NAFLD and chronic liver disease among adolescents and young adults[J]. Hepatology, 2022, 75( 5): 1204- 1217. DOI: 10.1002/hep.32228. [7] KERR CJ, WATERWORTH SP, BRODIE D, et al. The associations between physical activity intensity, cardiorespiratory fitness, and non-alcoholic fatty liver disease[J]. J Gastroenterol Hepatol, 2021, 36( 12): 3508- 3514. DOI: 10.1111/jgh.15672. [8] ZHOU BJ, HUANG G, WANG W, et al. Intervention effects of four exercise modalities on nonalcoholic fatty liver disease: A systematic review and Bayesian network meta-analysis[J]. Eur Rev Med Pharmacol Sci, 2021, 25( 24): 7687- 7697. DOI: 10.26355/eurrev_202112_27615. [9] HEJAZI K, HACKETT D. Effect of exercise on liver function and insulin resistance markers in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis of randomized controlled trials[J]. J Clin Med, 2023, 12( 8): 3011. DOI: 10.3390/jcm12083011. [10] ASTINCHAP A, MONAZZAMI A, FEREIDOONFARA K, et al. Modulation of fibroblast growth factor-21 and βklotho proteins expression in type 2 diabetic women with non-alcoholic fatty liver disease following endurance and strength training[J]. Hepat Mon, 2021, 21( 7): e116513. DOI: 10.5812/hepatmon.116513. [11] BACCHI E, NEGRI C, TARGHER G, et al. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease(the RAED2 Randomized Trial)[J]. Hepatology, 2013, 58( 4): 1287- 1295. DOI: 10.1002/hep.26393. [12] BALDUCCI S, CARDELLI P, PUGLIESE L, et al. Volume-dependent effect of supervised exercise training on fatty liver and visceral adiposity index in subjects with type 2 diabetes The Italian Diabetes Exercise Study(IDES)[J]. Diabetes Res Clin Pract, 2015, 109( 2): 355- 363. DOI: 10.1016/j.diabres.2015.05.033. [13] LEI SY, LIAN LY, ZHENG MH. Excerpt and interpretation of the Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic dysfunction-associated fatty liver disease in 2025[J]. J Clin Hepatol, 2025, 41( 6): 1043- 1052. DOI: 10.12449/JCH250607.雷偲艺, 连莉优, 郑明华.《2025年亚太肝病学会临床实践指南: 代谢相关脂肪性肝病的诊断和管理》摘译与解读[J]. 临床肝胆病杂志, 2025, 41( 6): 1043- 1052. DOI: 10.12449/JCH250607. [14] GU ZQ, XU F, WEI J, et al. Talk test: A convenient option for prescribing exercise intensity[J]. China Sport Sci, 2019, 39( 12): 54- 61. DOI: 10.16469/j.css.201912006.顾正秋, 徐飞, 魏佳, 等. 说话测试: 运动处方强度制定指标的便捷选择[J]. 体育科学, 2019, 39( 12): 54- 61. DOI: 10.16469/j.css.201912006. [15] WANG ZZ. Research and application progress of exercise prescriptions[J]. J Phys Res, 2021, 35( 3): 40- 49. DOI: 10.15877/j.cnki.nsic.20210601.001.王正珍. 运动处方的研究与应用进展[J]. 体育学研究, 2021, 35( 3): 40- 49. DOI: 10.15877/j.cnki.nsic.20210601.001. [16] de PIANO A, de MELLO MT, de L SANCHES P, et al. Long-term effects of aerobic plus resistance training on the adipokines and neuropeptides in nonalcoholic fatty liver disease obese adolescents[J]. Eur J Gastroenterol Hepatol, 2012, 24( 11): 1313- 1324. DOI: 10.1097/MEG.0b013e32835793ac. [17] BABU AF, CSADER S, MÄNNISTÖ V, et al. Effects of exercise on NAFLD using non-targeted metabolomics in adipose tissue, plasma, urine, and stool[J]. Sci Rep, 2022, 12( 1): 6485. DOI: 10.1038/s41598-022-10481-9. [18] SHAMSODDINI A, SOBHANI V, GHAMAR CHEHREH ME, et al. Effect of aerobic and resistance exercise training on liver enzymes and hepatic fat in Iranian men with nonalcoholic fatty liver disease[J]. Hepat Mon, 2015, 15( 10): e31434. DOI: 10.5812/hepatmon.31434. [19] TAKAHASHI A, ABE K, USAMI K, et al. Simple resistance exercise helps patients with non-alcoholic fatty liver disease[J]. Int J Sports Med, 2015, 36( 10): 848- 852. DOI: 10.1055/s-0035-1549853. [20] MORADI KELARDEH B, RAHMATI-AHMADABAD S, FARZANEGI P, et al. Effects of non-linear resistance training and curcumin supplementation on the liver biochemical markers levels and structure in older women with non-alcoholic fatty liver disease[J]. J Bodyw Mov Ther, 2020, 24( 3): 154- 160. DOI: 10.1016/j.jbmt.2020.02.021. [21] ECKARD C, COLE R, LOCKWOOD J, et al. Prospective histopathologic evaluation of lifestyle modification in nonalcoholic fatty liver disease: A randomized trial[J]. Therap Adv Gastroenterol, 2013, 6( 4): 249- 259. DOI: 10.1177/1756283X13484078. [22] PUGH CJA, CUTHBERTSON DJ, SPRUNG VS, et al. Exercise training improves cutaneous microvascular function in nonalcoholic fatty liver disease[J]. Am J Physiol Endocrinol Metab, 2013, 305( 1): E50- E58. DOI: 10.1152/ajpendo.00055.2013. [23] SREENIVASA BABA C, ALEXANDER G, KALYANI B, et al. Effect of exercise and dietary modification on serum aminotransferase levels in patients with nonalcoholic steatohepatitis[J]. J Gastroenterol Hepatol, 2006, 21( 1 Pt 1): 191- 198. DOI: 10.1111/j.1440-1746.2005.04233.x. [24] HOUGHTON D, THOMA C, HALLSWORTH K, et al. Exercise reduces liver lipids and visceral adiposity in patients with nonalcoholic steatohepatitis in a randomized controlled trial[J]. Clin Gastroenterol Hepatol, 2017, 15( 1): 96- 102. e 3. DOI: 10.1016/j.cgh.2016.07.031. [25] CUTHBERTSON DJ, SHOJAEE-MORADIE F, SPRUNG VS, et al. Dissociation between exercise-induced reduction in liver fat and changes in hepatic and peripheral glucose homoeostasis in obese patients with non-alcoholic fatty liver disease[J]. Clin Sci, 2016, 130( 2): 93- 104. DOI: 10.1042/CS20150447. [26] RELJIC D, KONTUREK PC, HERRMANN HJ, et al. Very low-volume interval training improves nonalcoholic fatty liver disease fibrosis score and cardiometabolic health in adults with obesity and metabolic syndrome[J]. J Physiol Pharmacol, 2021, 72( 6). DOI: 10.26402/jpp.2021.6.10. [27] MOHAMMADI F, GHALAVAND A, DELARAMNASAB M. Effect of circuit resistance training and L-carnitine supplementation on body composition and liver function in men with non-alcoholic fatty liver disease[J]. Jundishapur J Chronic Dis Care, 2019, 8( 4): e90213. DOI: 10.5812/jjcdc.90213. [28] SHOJAEE-MORADIE F, CUTHBERTSON DJ, BARRETT M, et al. Exercise training reduces liver fat and increases rates of VLDL clearance but not VLDL production in NAFLD[J]. J Clin Endocrinol Metab, 2016, 101( 11): 4219- 4228. DOI: 10.1210/jc.2016-2353. [29] BHAT G, BABA CS, PANDEY A, et al. Life style modification improves insulin resistance and liver histology in patients with non-alcoholic fatty liver disease[J]. World J Hepatol, 2012, 4( 7): 209- 217. DOI: 10.4254/wjh.v4.i7.209. [30] ELSISIA HF, ANEISB YM. High-intensity circuit weight training versus aerobic training in patients with nonalcoholic fatty liver disease[J]. Bull Fac Phys Ther, 2015, 20( 2): 181- 192. DOI: 10.4103/1110-6611.174717. [31] IRAJI H, MINASIAN V, KELISHADI R. Changes in liver enzymes and metabolic profile in adolescents with fatty liver following exercise interventions[J]. Pediatr Gastroenterol Hepatol Nutr, 2021, 24( 1): 54- 64. DOI: 10.5223/pghn.2021.24.1.54. [32] ZHANG HJ, HE J, PAN LL, et al. Effects of moderate and vigorous exercise on nonalcoholic fatty liver disease: A randomized clinical trial[J]. JAMA Intern Med, 2016, 176( 8): 1074- 1082. DOI: 10.1001/jamainternmed.2016.3202. [33] FRANCO I, BIANCO A, MIRIZZI A, et al. Physical activity and low glycemic index Mediterranean diet: Main and modification effects on NAFLD score. results from a randomized clinical trial[J]. Nutrients, 2020, 13( 1): 66. DOI: 10.3390/nu13010066. [34] STINE JG, WELLES JE, KEATING S, et al. Serum fibroblast growth factor 21 is markedly decreased following exercise training in patients with biopsy-proven nonalcoholic steatohepatitis[J]. Nutrients, 2023, 15( 6): 1481. DOI: 10.3390/nu15061481. [35] ACHTEN J, SUTEDJA D, JOHNSON J, et al. Treatment of nonalcoholic steatohepatitis: The effects of regular exercise[J]. Eur J Sport Sci, 2003, 3( 4): 1- 13. DOI: 10.1080/17461390300073404. [36] HALLSWORTH K, FATTAKHOVA G, HOLLINGSWORTH KG, et al. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss[J]. Gut, 2011, 60( 9): 1278- 1283. DOI: 10.1136/gut.2011.242073. [37] HALLSWORTH K, THOMA C, HOLLINGSWORTH KG, et al. Modified high-intensity interval training reduces liver fat and improves cardiac function in non-alcoholic fatty liver disease: A randomized controlled trial[J]. Clin Sci, 2015, 129( 12): 1097- 1105. DOI: 10.1042/CS20150308. [38] FAHMY LM, ELHADY AA ABD, ALI AA, et al. Enhancing sleep quality in non-alcoholic fatty liver with combined accelerated aerobic training: A randomized control study[J]. Bull Rehabil Med, 2024, 23( 3): 14- 20. DOI: 10.38025/2078-1962-2024-23-3-14-20. [39] GHAMAR CHEHREH ME, SHAMSODDINI A, RAHIMI M. The effects of resistance training on body and liver fat stores and insulin resistance in peoples with non-alcoholic fatty liver disease[J]. Iranian J Public Health, 2020, 49( 3): 614- 616. DOI: 10.18502/ijph.v49i3.3166. [40] EZPELETA M, GABEL K, CIENFUEGOS S, et al. Effect of alternate day fasting combined with aerobic exercise on non-alcoholic fatty liver disease: A randomized controlled trial[J]. Cell Metab, 2023, 35( 1): 56- 70. e 3. DOI: 10.1016/j.cmet.2022.12.001. [41] NOROUZPOUR M, MARANDI SM, GHANBARZADEH M, et al. Response of inflammatory biomarkers to 10 weeks of aerobic resistance training in inactive postmenopausal women with non-alcoholic fatty liver[J]. Jundishapur J Chronic Dis Care, 2021, 10( 3): e114163. DOI: 10.5812/jjcdc.114163. [42] WINN NC, LIU Y, RECTOR RS, et al. Energy-matched moderate and high intensity exercise training improves nonalcoholic fatty liver disease risk independent of changes in body mass or abdominal adiposity- A randomized trial[J]. Metabolism, 2018, 78: 128- 140. DOI: 10.1016/j.metabol.2017.08.012. [43] O’GORMAN P, NAIMIMOHASSES S, MONAGHAN A, et al. Improvement in histological endpoints of MAFLD following a 12-week aerobic exercise intervention[J]. Aliment Pharmacol Ther, 2020, 52( 8): 1387- 1398. DOI: 10.1111/apt.15989. [44] REZENDE REF, DUARTE SMB, STEFANO JT, et al. Randomized clinical trial: Benefits of aerobic physical activity for 24 weeks in postmenopausal women with nonalcoholic fatty liver disease[J]. Menopause, 2016, 23( 8): 876- 883. DOI: 10.1097/GME.0000000000000647. [45] JAFARIKHAH R, DAMIRCHI A, RAHMANI NIA F, et al. Effect of functional resistance training on the structure and function of the heart and liver in patients with non-alcoholic fatty liver[J]. Sci Rep, 2023, 13: 15475. DOI: 10.1038/s41598-023-42687-w. [46] WILLIS SA, MALAIKAH S, BAWDEN SJ, et al. Greater hepatic lipid saturation is associated with impaired glycaemic regulation in men with metabolic dysfunction-associated steatotic liver disease but is not altered by 6 weeks of exercise training[J]. Diabetes Obes Metab, 2024, 26( 9): 4030- 4042. DOI: 10.1111/dom.15755. [47] CHENG SL, GE J, ZHAO C, et al. Effect of aerobic exercise and diet on liver fat in pre-diabetic patients with non-alcoholic-fatty-liver-disease: A randomized controlled trial[J]. Sci Rep, 2017, 7( 1): 15952. DOI: 10.1038/s41598-017-16159-x. [48] CSADER S, ISMAIAH MJ, KUNINGAS T, et al. Twelve weeks of high-intensity interval training alters adipose tissue gene expression but not oxylipin levels in people with non-alcoholic fatty liver disease[J]. Int J Mol Sci, 2023, 24( 10): 8509. DOI: 10.3390/ijms24108509. [49] KEATING SE, CROCI I, WALLEN MP, et al. High-intensity interval training is safe, feasible and efficacious in nonalcoholic steatohepatitis: A randomized controlled trial[J]. Dig Dis Sci, 2023, 68( 5): 2123- 2139. DOI: 10.1007/s10620-022-07779-z. [50] FAKHREDIN HOSEINI S, RAHMATI M, GOLLOP ND, et al. The effects of high intensity interval training on the levels of liver enzymes associated with non-alcoholic fatty liver and selected anthropometric indices in obese men[J]. Sci Phys, 2019, 34( 1): 59- 60. DOI: 10.1016/j.scispo.2018.10.008. [51] EL-KADER SM ABD, AL-JIFFRI OH, AL-SHREEF FM. Markers of liver function and inflammatory cytokines modulation by aerobic versus resisted exercise training for nonalcoholic steatohepatitis patients[J]. Afr Health Sci, 2014, 14( 3): 551- 557. DOI: 10.4314/ahs.v14i3.8. [52] CHEN SM, LIU CY, LI SR, et al. Effects of therapeutic lifestyle program on ultrasound-diagnosed nonalcoholic fatty liver disease[J]. J Chin Med Assoc, 2008, 71( 11): 551- 558. DOI: 10.1016/S1726-4901(08)70168-0. [53] NAIMIMOHASSES S, O’GORMAN P, WRIGHT C, et al. Differential effects of dietary versus exercise intervention on intrahepatic MAIT cells and histological features of NAFLD[J]. Nutrients, 2022, 14( 11): 2198. DOI: 10.3390/nu14112198. [54] OH S, SO R, SHIDA T, et al. High-intensity aerobic exercise improves both hepatic fat content and stiffness in sedentary obese men with nonalcoholic fatty liver disease[J]. Sci Rep, 2017, 7: 43029. DOI: 10.1038/srep43029. [55] OH S, OSHIDA N, SOMEYA N, et al. Whole-body vibration for patients with nonalcoholic fatty liver disease: A 6-month prospective study[J]. Physiol Rep, 2019, 7( 9): e14062. DOI: 10.14814/phy2.14062. [56] RAJABI S, ASKARI R, HAGHIGHI AH, et al. The effects of two different intensities of combined training on C1q/TNF-related protein 3(CTRP3) and insulin resistance in women with non-alcoholic fatty liver disease[J]. Hepat Mon, 2021, 21( 2): e108106. DOI: 10.5812/hepatmon.108106. [57] SULLIVAN S, KIRK EP, MITTENDORFER B, et al. Randomized trial of exercise effect on intrahepatic triglyceride content and lipid kinetics in nonalcoholic fatty liver disease[J]. Hepatology, 2012, 55( 6): 1738- 1745. DOI: 10.1002/hep.25548. [58] ZELBER-SAGI S, BUCH A, YESHUA H, et al. Effect of resistance training on non-alcoholic fatty-liver disease a randomized-clinical trial[J]. World J Gastroenterol, 2014, 20( 15): 4382- 4392. DOI: 10.3748/wjg.v20.i15.4382. [59] ÇEVIK SALDIRAN T, MUTLUAY FK, YAĞCI İ, et al. Impact of aerobic training with and without whole-body vibration training on metabolic features and quality of life in non-alcoholic fatty liver disease patients[J]. Ann Endocrinol, 2020, 81( 5): 493- 499. DOI: 10.1016/j.ando.2020.05.003. [60] ABDELBASSET WK, TANTAWY SA, KAMEL DM, et al. A randomized controlled trial on the effectiveness of 8-week high-intensity interval exercise on intrahepatic triglycerides, visceral lipids, and health-related quality of life in diabetic obese patients with nonalcoholic fatty liver disease[J]. Medicine, 2019, 98( 12): e14918. DOI: 10.1097/MD.0000000000014918. [61] ABDELBASSET WK, TANTAWY SA, KAMEL DM, et al. Effects of high-intensity interval and moderate-intensity continuous aerobic exercise on diabetic obese patients with nonalcoholic fatty liver disease: A comparative randomized controlled trial[J]. Medicine, 2020, 99( 10): e19471. DOI: 10.1097/MD.0000000000019471. [62] HOSEINI Z, BEHPOUR N, HOSEINI R. Co-treatment with vitamin D supplementation and aerobic training in elderly women with vit D deficiency and NAFLD: A single-blind controlled trial[J]. Hepat Mon, 2020, 20( 2): e96437. DOI: 10.5812/hepatmon.96437. [63] KEYMASI Z, SADEGHI A, POURRAZI H. Effect of Pilates training on hepatic fat content and liver enzymes in middle-aged men with non-alcoholic fatty liver disease[J]. Balt J Health Phys Act, 2020, 12( 1): 32- 40. DOI: 10.29359/bjhpa.12.1.04. [64] QI Z, LE SL, CHENG RT, et al. Responses of the serum lipid profile to exercise and diet interventions in nonalcoholic fatty liver disease[J]. Med Sci Sports Exerc, 2024, 56( 6): 1036- 1045. DOI: 10.1249/MSS.0000000000003388. [65] FU YY, MENG MM, RONG N, et al. Effect of aerobic exercise and resistance exercise on patients with nonalcoholic fatty liver disease[J]. Acta Univ Med Nanjing Nat Sci, 2018, 38( 4): 528- 531. DOI: 10.7655/NYDXBNS20180422.付洋洋, 孟美美, 荣宁, 等. 有氧运动与抗阻运动对非酒精性脂肪肝患者影响效果研究[J]. 南京医科大学学报(自然科学版), 2018, 38( 4): 528- 531. DOI: 10.7655/NYDXBNS20180422. [66] WU MF, LU AM. Effects of aerobic exercise combined with controlled diet on the serum level of SREBP-1c and RBP4 in patients with non-alcoholic fatty liver disease[J]. Chin J Rehabil Med, 2015, 30( 2): 132- 137. DOI: 10.3969/j.issn.1001-1242.2015.02.006.吴明方, 陆阿明. 有氧运动及其联合饮食干预影响非酒精性脂肪肝患者血浆SREBP-1c、RBP4水平的研究[J]. 中国康复医学杂志, 2015, 30( 2): 132- 137. DOI: 10.3969/j.issn.1001-1242.2015.02.006. [67] MAO ZH. Effect of Oenothera erythrosepala borb with aerobic exercise on serum lipid metabolism and liver histolomorph of non-alcoholic fatty liver patients[J]. J Beijing Sport Univ, 2008, 31( 8): 1087- 1089. DOI: 10.19582/j.cnki.11-3785/g8.2008.08.021.毛治和. 月见草联合有氧运动治疗对非酒精性脂肪肝患者血脂代谢和肝脏形态的影响[J]. 北京体育大学学报, 2008, 31( 8): 1087- 1089. DOI: 10.19582/j.cnki.11-3785/g8.2008.08.021. [68] LUO C, LI HR, TIAN DH, et al. High intensity interval exercise on NAFLD under exercise and medical integration: Exercise method and evaluation[J]. J Beijing Norm Univ Nat Sci, 2020, 56( 1): 132- 140. DOI: 10.16360/j.cnki.jbnuns.2020.01.018.罗超, 李晗冉, 田东华, 等. 体医融合模式下HIIT干预NAFLD的运动方法与效果评价[J]. 北京师范大学学报(自然科学版), 2020, 56( 1): 132- 140. DOI: 10.16360/j.cnki.jbnuns.2020.01.018. [69] XU SS. Influences of walking on some blood biochemical index of NAFLD patients[J]. J Xi’an Phys Educ Univ, 2006, 23( 5): 79- 81, 101. DOI: 10.3969/j.issn.1001-747X.2006.05.024.许寿生. 健步走对非酒精性脂肪性肝病患者血液生化指标的影响[J]. 西安体育学院学报, 2006, 23( 5): 79- 81, 101. DOI: 10.3969/j.issn.1001-747X.2006.05.024. [70] ZHAO C, WANG RW, GAO BH. Method, dose and pathway of different exercise types to intrahepatic lipid in patients with nonalcoholic fatty liver disease[J]. J Shanghai Univ Sport, 2021, 45( 6): 80- 92. DOI: 10.16099/j.sus.2021.06.006.赵璨, 王人卫, 高炳宏. 不同类型运动干预非酒精性脂肪性肝病患者肝内脂质的方式、剂量与途径[J]. 上海体育学院学报, 2021, 45( 6): 80- 92. DOI: 10.16099/j.sus.2021.06.006. [71] HUANG MM, YANG JF, WANG YH, et al. Comparative efficacy of different exercise modalities on metabolic profiles and liver functions in non-alcoholic fatty liver disease: A network meta-analysis[J]. Front Physiol, 2024, 15: 1428723. DOI: 10.3389/fphys.2024.1428723. [72] JAMIALAHMADI O, de VINCENTIS A, TAVAGLIONE F, et al. Partitioned polygenic risk scores identify distinct types of metabolic dysfunction-associated steatotic liver disease[J]. Nat Med, 2024, 30( 12): 3614- 3623. DOI: 10.1038/s41591-024-03284-0. [73] WANG YJ, CHENG HR, ZHOU WH. Correlation of body fat composition and metabolic indicators with metabolic-associated fatty liver disease in a non-obese population[J]. Chin Gen Pract, 2023, 26( 6): 672- 680. DOI: 10.12114/j.issn.1007-9572.2022.0573.王颖捷, 程昊然, 周卫红. 体脂成分及代谢指标与非肥胖人群代谢相关脂肪性肝病的相关性研究[J]. 中国全科医学, 2023, 26( 6): 672- 680. DOI: 10.12114/j.issn.1007-9572.2022.0573. [74] ZHAO SP. Meta-analysis of effects of moderate-intensity aerobic exercise on blood lipid levels of patients with hyperlipidemia based on evidence from randomized controlled trials[J]. J Wuhan Inst Phys Educ, 2022, 56( 3): 79- 85. DOI: 10.15930/j.cnki.wtxb.2022.03.010.赵少平. 中等强度有氧运动对高血脂患者血脂水平影响的元分析: 基于随机对照试验的证据[J]. 武汉体育学院学报, 2022, 56( 3): 79- 85. DOI: 10.15930/j.cnki.wtxb.2022.03.010. [75] XUE YQ, PENG Y, ZHANG LT, et al. Effect of different exercise modalities on nonalcoholic fatty liver disease: A systematic review and network meta-analysis[J]. Sci Rep, 2024, 14( 1): 6212. DOI: 10.1038/s41598-024-51470-4. [76] QIN L, FU ZT, ZHANG Y, et al. The effect of exercise on lipid metabolism in metabolic diseases analyzed based on lipidomics[J]. Chin Bull Life Sci, 2024, 36( 11): 1375- 1385. DOI: 10.13376/j.cbls/20240167.秦朗, 傅泽铤, 张燕, 等. 基于脂质组学分析运动对代谢性疾病中脂质代谢的影响[J]. 生命科学, 2024, 36( 11): 1375- 1385. DOI: 10.13376/j.cbls/20240167. [77] KELLEY GA, KELLEY KS, ROBERTS S, et al. Comparison of aerobic exercise, diet or both on lipids and lipoproteins in adults: A meta-analysis of randomized controlled trials[J]. Clin Nutr, 2012, 31( 2): 156- 167. DOI: 10.1016/j.clnu.2011.11.011. [78] GRONEK P, WIELINSKI D, CYGANSKI P, et al. A review of exercise as medicine in cardiovascular disease: Pathology and mechanism[J]. Aging Dis, 2020, 11( 2): 327- 340. DOI: 10.14336/AD.2019.0516. [79] KRÜGER K, TIREKOGLOU P, WEYH C. Immunological mechanisms of exercise therapy in dyslipidemia[J]. Front Physiol, 2022, 13: 903713. DOI: 10.3389/fphys.2022.903713. [80] SMART NA, DOWNES D, van der TOUW T, et al. The effect of exercise training on blood lipids: A systematic review and meta-analysis[J]. Sports Med, 2025, 55( 1): 67- 78. DOI: 10.1007/s40279-024-02115-z. [81] LI BB, MENG ZL. Effect of exercise intervention on glucose and lipid metabolism in the pre-diabetic population: A network meta-analysis[J]. China Sport Sci Technol, 2023, 59( 1): 92- 103. DOI: 10.16470/j.csst.2021044.李贝贝, 孟昭莉. 运动干预对糖尿病前期人群糖脂代谢影响的网状Meta分析[J]. 中国体育科技, 2023, 59( 1): 92- 103. DOI: 10.16470/j.csst.2021044. [82] SANYAL AJ, FOUCQUIER J, YOUNOSSI ZM, et al. Enhanced diagnosis of advanced fibrosis and cirrhosis in individuals with NAFLD using FibroScan-based Agile scores[J]. J Hepatol, 2023, 78( 2): 247- 259. DOI: 10.1016/j.jhep.2022.10.034. [83] QU JC, DOU JT, WANG AP, et al. Association between glutamyl transpeptidase and risk of new onset diabetes in middle aged and elderly population[J]. Chin J Diabetes, 2025, 33( 1): 23- 27. DOI: 10.3969/j.issn.1006-6187.2025.01.005.曲建昌, 窦京涛, 王安平, 等. 谷氨酰转肽酶与中老年人群新发糖尿病风险相关性的研究[J]. 中国糖尿病杂志, 2025, 33( 1): 23- 27. DOI: 10.3969/j.issn.1006-6187.2025.01.005. [84] HASHIDA R, KAWAGUCHI T, BEKKI M, et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: A systematic review[J]. J Hepatol, 2017, 66( 1): 142- 152. DOI: 10.1016/j.jhep.2016.08.023. [85] CHARATCHAROENWITTHAYA P, KULJIRATITIKAL K, AKSORNC-HANYA O, et al. Moderate-intensity aerobic vs resistance exercise and dietary modification in patients with nonalcoholic fatty liver disease: A randomized clinical trial[J]. Clin Transl Gastroenterol, 2021, 12( 3): e00316. DOI: 10.14309/ctg.0000000000000316. [86] KEATING SE, SABAG A, HALLSWORTH K, et al. Exercise in the management of metabolic-associated fatty liver disease(MAFLD) in adults: A position statement from exercise and sport science Australia[J]. Sports Med, 2023, 53( 12): 2347- 2371. DOI: 10.1007/s40279-023-01918-w. -

 本文二维码
本文二维码
计量
- 文章访问数: 785
- HTML全文浏览量: 171
- PDF下载量: 125
- 被引次数: 0

