
 PDF下载 ( 1076 KB)
PDF下载 ( 1076 KB)

内镜下曲张静脉套扎术/组织胶注射术治疗肝硬化食管胃静脉曲张的安全性及术后出血的影响因素分析
DOI: 10.12449/JCH260215
Safety of endoscopic variceal ligation and endoscopic cyanoacrylate injection in treatment of esophagogastric varices in patients with liver cirrhosis and influencing factors for postoperative bleeding
-
摘要:
目的 分析内镜下曲张静脉套扎术(EVL)和内镜下组织胶注射术(ECI)治疗肝硬化食管胃静脉曲张术后5 d和2周内出血的影响因素,探讨血小板计数减少患者接受EVL/ECI的安全性。 方法 选取2018年1月—2023年12月于广州医科大学附属市八医院接受EVL/ECI治疗的489例肝硬化食管胃静脉曲张患者为研究对象,根据术后是否出血分为术后出血组和术后未出血组,分析术后5 d和2周出血的危险因素。计量资料两组间比较采用成组t检验或Mann-Whitney U检验,计数资料两组间比较采用χ2检验或连续校正χ2检验;通过受试者操作特征曲线(ROC曲线)确定终末期肝病模型(MELD)评分的截断值。采用Logistic多因素回归分析术后出血的独立危险因素。 结果 血小板计数≥50×109/L患者(n=386)与血小板计数在25×109/L~49×109/L的患者(n=103)EVL/ECI术后5 d出血率(1.94% vs 2.85%,P=0.870)和术后2周出血率(2.91% vs 4.92%,P=0.544)比较,差异均无统计学意义。EVL/ECI术后5 d和2周的总体出血率分别是2.66%(13/489)和4.50%(22/489)。Logistic多因素回归分析显示,MELD评分是EVL/ECI术后5 d出血[比值比(OR)=3.726,95%置信区间(CI):1.214~11.429,P=0.021]和术后2周出血的独立危险因素(OR=5.760,95%CI:1.779~18.651,P=0.003),血红蛋白是术后5 d(OR=0.972, 95%CI: 0.948~0.996,P=0.025)和术后2周(OR=0.976, 95%CI: 0.957~0.995,P=0.016)出血的保护因素,门静脉癌栓是术后2周出血的独立危险因素(OR=2.667,95%CI:1.000~7.117,P=0.050),血小板计数(25×109/L~49×109/L)不是术后出血的危险因素(P>0.05)。 结论 对于伴有三级血小板减少的肝病患者,EVL和ECI治疗安全性较好;MELD评分是术后5 d和2周出血的独立危险因素,血红蛋白为保护因素;门静脉癌栓是术后2周出血的独立危险因素。 Abstract:Objective To investigate the risk factors for bleeding within 5 days and 2 weeks after endoscopic variceal ligation (EVL) or endoscopic cyanoacrylate injection (ECI) for the treatment of esophagogastric varices in patients with liver cirrhosis, as well as the safety of EVL/ECI in patients with thrombocytopenia. Methods A total of 489 patients with liver cirrhosis and esophagogastric varices who underwent EVL/ECI in Guangzhou Eighth People’s Hospital, Guangzhou Medical University, from January 2018 to December 2023 were enrolled as subjects, and according to the presence or absence of bleeding after surgery, they were divided into bleeding group and non-bleeding group. The risk factors for bleeding within 5 days and 2 weeks after surgery were analyzed. The independent-samples t test or the Mann-Whitney U test was used for comparison of continuous data between groups, and the chi-square test or the continuity-corrected chi-square test was used for comparison of categorical data between groups; the receiver operating characteristic (ROC) curve was plotted to determine the cut-off value of MELD score; a multivariate logistic regression analysis was used to identify the independent risk factors for postoperative bleeding. Results There were no significant differences in the bleeding rates within 5 days and 2 weeks after EVL/ECI between the 386 patients with a platelet count of ≥50×109/L and the 103 patients with a platelet count of (25 — 49)×109/L (5 days: 1.94% vs 2.85%, P=0.870; 2 weeks: 2.91% vs 4.92%, P=0.544). The overall bleeding rate was 2.66% (13/489) and 4.50% (22/489), respectively, within 5 days and 2 weeks after EVL/ECI. The multivariate logistic regression analysis showed that MELD score was an independent risk factor for bleeding within 5 days (odds ratio [OR]=3.726, 95% confidence interval [CI]: 1.214 — 11.429, P=0.021) and 2 weeks (OR=5.760, 95%CI: 1.779 — 18.651, P=0.003) after EVL/ECI, while hemoglobin (Hb) was a protective factor against bleeding within 5 days (OR=0.972, 95%CI: 0.948 — 0.996, P=0.025) and 2 weeks (OR=0.976, 95%CI: 0.957 — 0.995, P=0.016) after surgery; portal vein tumor thrombus (OR=2.667, 95%CI: 1.000 — 7.117, P=0.050) was an independent risk factor for bleeding within 2 weeks after surgery, while platelet count [(25 — 49)×10⁹/L] was not a risk factor for postoperative bleeding (P>0.05). Conclusion Both EVL and ECI have good safety in patients with liver diseases and grade 3 thrombocytopenia. MELD score is an independent risk factor for bleeding within 5 days and 2 weeks after EVL/ECI, while Hb is a protective factor; portal vein tumor thrombus is an independent risk factor for bleeding within 2 weeks after surgery. -
Key words:
- Thrombocytopenia /
- Esophageal and Gastric Varices /
- Endoscopy
-
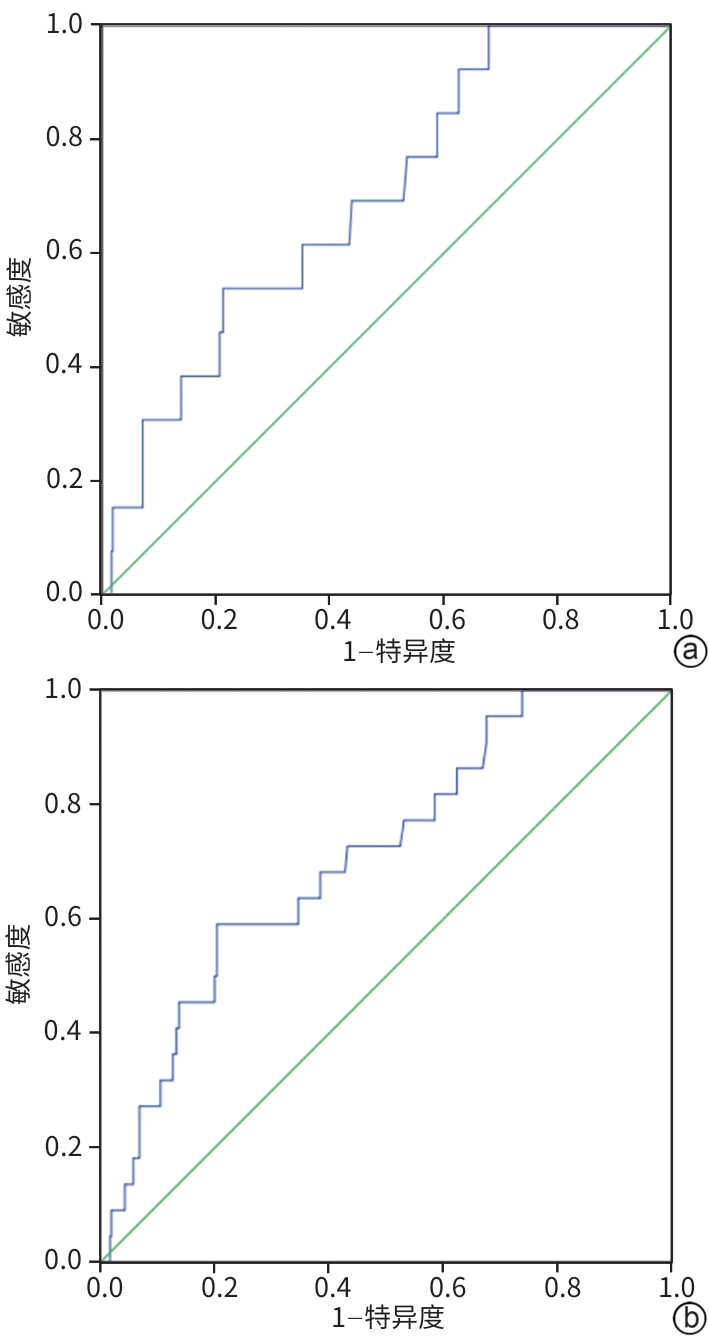
注: a,5 d;b,2周。MELD,终末期肝病模型;EVL,内镜下曲张静脉套扎术;ECI,内镜下组织胶注射术;ROC曲线,受试者操作特征曲线。
图 1 MELD评分预测 EVL/ECI术后出血的ROC曲线
Figure 1. ROC curve of MELD scoring in predicting of bleeding after EVL/ECI
表 1 EVL/ECI术后5 d出血组和未出血组的基线特征比较
Table 1. Comparison of baseline characteristics between bleeding group and non bleeding group after 5-day EVL/ECI
项目 术后5 d出血组
(n=13)术后5 d未出血组
(n=476)统计值 P值 男性[例(%)] 12(92.3) 404(84.9) χ2=0.121 0.728 年龄(岁) 51.54±9.33 53.09±10.66 t=-0.519 0.604 肝硬化病因[例(%)] χ2=0.182 0.670 HBV相关 9(69.2) 372(78.2) 无HBV 4(30.8) 104(21.8) 合并肝癌[例(%)] 6(46.2) 145(30.5) χ2=0.817 0.366 门静脉血栓[例(%)] 1(7.7) 38(8.0) χ2=0.000 >0.05 门静脉宽度(cm) 14(12~16) 13(12~14) Z=-1.730 0.080 门静脉癌栓[例(%)] 5(30.8) 59(12.4) χ2=2.345 0.126 内镜治疗方式[例(%)] χ2=1.318 0.251 EVL 9(68.2) 404(84.9) EVL+ECI 4(30.8) 72(15.1) 血小板计数(×109/L) 72(54~153) 77(52~116) Z=-0.373 0.709 血小板计数[例(%)] χ2=0.027 0.870 ≥50×109/L 11(84.6) 375(78.8) 25×109/L~49×109/L 2(15.4) 101(21.2) HGB(g/L) 63(52~77) 87(65~111) Z=-2.640 0.008 PTA(%) 55(49~68) 63(52~72) Z=-1.405 0.160 INR 1.49(1.28~1.62) 1.35(1.21~1.58) Z=-1.357 0.175 PT(s) 18.20(16.10~19.55) 16.7(15.4~18.8) Z=-1.388 0.165 APTT(s) 42.10(39.35~58.15) 41.15(37.57~45.39) Z=-1.411 0.158 TBil(μmol/L) 24.68(13.75~96.71) 22.48(14.87~37.90) Z=-0.787 0.431 Alb(g/L) 31.85±5.52 32.95±5.58 t=-0.702 0.483 MELD评分(分) 14.43(10.33~20.02) 10.90(8.93~3.63) Z=-2.410 0.016 Child-Pugh评分(分) 8(7~10) 7(6~9) Z=-1.210 0.226 注:EVL,内镜下曲张静脉套扎术;ECI,内镜下组织胶注射术;HBV,乙型肝炎病毒;HGB,血红蛋白; PTA,凝血酶原活动度;INR,国际标准化比值;PT,凝血酶原时间;APTT,活化部分凝血活酶时间;TBil,总胆红素;Alb,白蛋白;MELD,终末期肝病模型;Child-Pugh评分,蔡尔德-皮尤评分。
 下载: 导出CSV
下载: 导出CSV
表 2 EVL/ECI术后5 d出血的单因素和多因素Logistic回归分析
Table 2. Univariate and multivariate Logistic regression analysis of bleeding 5-days after EVL/ECI
影响因素 单因素分析 多因素分析 OR(95%CI) P值 B值 SE Wald OR(95%CI) P值 HGB(g/L) 0.971(0.949~0.994) 0.015 -0.029 0.013 4.996 0.972(0.948~0.996) 0.025 MELD评分>14.39分 4.278(1.407~13.009) 0.010 1.315 0.572 5.289 3.726(1.214~11.429) 0.021 Child-Pugh评分(分) 1.186(0.931~1.511) 0.168 PT(s) 1.075(0.966~1.195) 0.184 APTT(s) 1.000(0.997~1.003) 0.983 INR 1.689(0.749~3.810) 0.207 血小板计数(25×109/L~49×109/L) 0.675(0.147~3.095) 0.613 内镜治疗方式 2.494(0.748~8.315) 0.137 门静脉癌栓 3.141(0.938~10.523) 0.063 注:EVL,内镜下曲张静脉套扎术;ECI,内镜下组织胶注射术;HGB,血红蛋白;MELD,终末期肝病模型;Child-Pugh评分,蔡尔德-皮尤评分;PT,凝血酶原时间;APTT,活化部分凝血活酶时间;INR,国际标准化比值;OR,比值比;CI,置信区间。
下载: 导出CSV
表 3 EVL/ECI术后2周出血的单因素和多因素Logistic回归分析
Table 3. Univariate and multivariate Logistic regression analysis of bleeding 2-weeks after EVL/ECI
影响因素 单因素分析 多因素分析 OR(95%CI) P值 B值 SE Wald OR(95%CI) P值 HGB(g/L) 0.976(0.959~0.993) 0.006 -0.024 0.010 5.777 0.976(0.957~0.995) 0.016 MELD评分>14.39分 4.919(2.046~11.825) <0.001 1.751 0.599 8.533 5.760(1.779~18.651) 0.003 Child-Pugh评分(分) 1.280(1.062~1.542) 0.010 PT(s) 1.092(1.004~1.187) 0.040 APTT(s) 1.000(0.997~1.003) 0.926 INR 1.909(0.984~3.702) 0.056 血小板计数(25×109/L~49×109/L) 1.726(0.501~5.949) 0.388 内镜治疗方式 1.304(0.428~3.970) 0.640 门静脉癌栓 4.281(1.718~10.66) 0.002 0.981 0.501 3.837 2.667(1.000~7.117) 0.050 注: EVL,内镜下曲张静脉套扎术;ECI,内镜下组织胶注射术;HGB,血红蛋白;MELD,终末期肝病模型;Child-Pugh评分,蔡尔德-皮尤评分;PT,凝血酶原时间;APTT,活化部分凝血活酶时间;INR,国际标准化比值;OR,比值比;CI,置信区间。
下载: 导出CSV
-
[1] Endoscopic Diagnosis and Treatment Group of Esophageal and Gastric Varices, Digestive Endoscopy Branch, Chinese Medical Association. Expert consensus on endoscopic tissue glue injection for the treatment of gastrointestinal varicose veins with cirrhosis, portal hypertension(Changsha, 2022)[J]. Chin J Dig Endosc, 2023, 40( 1): 12- 23. DOI: 10.3760/cma.j.cn321463-20221016-00530.中华医学会消化内镜学分会食管胃静脉曲张内镜诊断与治疗学组. 肝硬化门静脉高压消化道静脉曲张内镜下组织胶注射治疗专家共识(2022,长沙)[J]. 中华消化内镜杂志, 2023, 40( 1): 12- 23. DOI: 10.3760/cma.j.cn321463-20221016-00530. [2] Chinese Medical Association Liver Disease Branch, Chinese Medical Association Digestive Disease Branch, Chinese Medical Association Endoscopy Branch. Guidelines for prevention and treatment of esophageal and gastric variceal bleeding due to portal hypertension in liver cirrhosis[J]. J Clin Hepatol, 2016, 32( 2): 203- 219. DOI: 10.3969/j.issn.1001-5256.2016.02.002.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2016, 32( 2): 203- 219. DOI: 10.3969/j.issn.1001-5256.2016.02.002. [3] BIOLATO M, VITALE F, GALASSO T, et al. Minimum platelet count threshold before invasive procedures in cirrhosis: Evolution of the guidelines[J]. World J Gastrointest Surg, 2023, 15( 2): 127- 141. DOI: 10.4240/wjgs.v15.i2.127. [4] National Clinical Research Center for Infectious Diseases; Society of Hepatology, Beijing Medical Association; Translational Medicine Branch, Chinese Association of Gerontology and Geriatrics. Chinese expert consensus on clinical management of hepatopathy-related thrombocytopenia[J]. J Clin Hepatol, 2023, 39( 10): 2307- 2320. DOI: 10.3969/j.issn.1001-5256.2023.10.007.国家感染性疾病临床医学研究中心, 北京医学会肝病学分会, 中国老年学和老年医学学会转化医学分会. 肝病相关血小板减少症临床管理中国专家共识[J]. 临床肝胆病杂志, 2023, 39( 10): 2307- 2320. DOI: 10.3969/j.issn.1001-5256.2023.10.007. [5] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno VII-Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76( 4): 959- 974. DOI: 10.1016/j.jhep.2021.12.022. [6] JIA LY, NIE YQ, XIE B, et al. Safe platelet threshold in patients undergoing endoscopic variceal ligation and cyanoacrylate injection due to esophagogastric variceal bleeding: Consensus and challenges[J]. J Clin Hepatol, 2025, 41( 9): 1908- 1912. DOI: 10.12449/JCH250929.贾璐瑶, 聂玉强, 谢飚, 等. 食管胃静脉曲张破裂出血行内镜下曲张静脉套扎术和内镜下组织胶注射术的血小板安全阈值: 共识与挑战[J]. 临床肝胆病杂志, 2025, 41( 9): 1908- 1912. DOI: 10.12449/JCH250929. [7] VIEIRA DA ROCHA EC, D’AMICO EA, CALDWELL SH, et al. A prospective study of conventional and expanded coagulation indices in predicting ulcer bleeding after variceal band ligation[J]. Clin Gastroenterol Hepatol, 2009, 7( 9): 988- 993. DOI: 10.1016/j.cgh.2009.04.019. [8] de OLIVEIRA SOUZA E, D’AMICO ÉA, FLORES DA ROCHA TR, et al. Preservation of platelet function in patients with cirrhosis and thrombocytopenia undergoing esophageal variceal ligation[J]. Hepatobiliary Pancreat Dis Int, 2020, 19( 6): 555- 560. DOI: 10.1016/j.hbpd.2019.12.009. [9] PFISTERER N, SCHWARZ M, JACHS M, et al. Endoscopic band ligation is safe despite low platelet count and high INR[J]. Hepatol Int, 2023, 17( 5): 1205- 1214. DOI: 10.1007/s12072-023-10515-y. [10] DI MARTINO V, SIMONE F, GRASSO M, et al. Child-Pugh class and not thrombocytopenia impacts the risk of complications of endoscopic band ligation in patients with cirrhosis and high risk varices[J]. J Pers Med, 2023, 13( 5): 764. DOI: 10.3390/jpm13050764. [11] VILLA E, BIANCHINI M, BLASI A, et al. EASL clinical practice guidelines on prevention and management of bleeding and thrombosis in patients with cirrhosis[J]. J Hepatol, 2022, 76( 5): 1151- 1184. DOI: 10.1016/j.jhep.2021.09.003. [12] O’SHEA RS, DAVITKOV P, KO CW, et al. AGA clinical practice guideline on the management of coagulation disorders in patients with cirrhosis[J]. Gastroenterology, 2021, 161( 5): 1615- 1627.e1. DOI: 10.1053/j.gastro.2021.08.015. [13] LIU LM, ZHANG CQ. Research progress on high risk factors of rebleeding after endoscopic treatment of esophageal-gastric varices bleeding[J/OL]. Chin J Dig Med Image(Electron Ed), 2022, 12( 4): 236- 240. DOI: 10.3877/cma.j.issn.2095-2015.2022.04.010.刘黎明, 张春清. 食管-胃底静脉曲张破裂出血内镜治疗后再出血高危因素研究进展[J/OL]. 中华消化病与影像杂志(电子版), 2022, 12( 4): 236- 240. DOI: 10.3877/cma.j.issn.2095-2015.2022.04.010. [14] DING PP, ZHANG WH, LU Z, et al. Analysis of risk factors for failure of emergency endoscopic hemostasis for esophageal and gastric varices bleeding due to liver cirrhosis[J]. Chin J Dig, 2020, 40( 6): 410- 413. DOI: 10.3760/cma.j.cn311367-20190725-00332.丁鹏鹏, 张文辉, 路筝, 等. 肝硬化食管胃静脉曲张破裂出血急诊胃镜下止血治疗失败的危险因素分析[J]. 中华消化杂志, 2020, 40( 6): 410- 413. DOI: 10.3760/cma.j.cn311367-20190725-00332. [15] LI XY, CUI YJ, GAO S, et al. Development and validation of a score model for predicting the risk of first esophagogastric variceal hemorrhage and mortality in patients with hepatocellular carcinoma[J]. Ann Med, 2025, 57( 1): 2490210. DOI: 10.1080/07853890.2025.2490210. [16] LIU XY, WANG YL, ZHENG L, et al. Risk factors analysis of endoscopy and TIPS in the treatment of secondary esophagogastric varicose bleeding with cirrhosis[J]. Afr Health Sci, 2023, 23( 3): 655- 663. DOI: 10.4314/ahs.v23i3.76. [17] Liver Fibrosis, Cirrhosis and Portal Hypertension Group, Hepatology Branch, Chinese Medical Association. Practical Guidelines for Clinical Management of Thrombocytopenia in Cirrhosis[J]. Chin J Hepatol, 2024, 32( 10): 865- 871. DOI: 10.3760/cma.j.cn501113-20240806-00361.中华医学会肝病学分会肝纤维化、肝硬化及门静脉高压学组. 肝硬化血小板减少症临床管理实用指南[J]. 中华肝脏病杂志, 2024, 32( 10): 865- 871. DOI: 10.3760/cma.j.cn501113-20240806-00361. [18] O’LEARY JG, GREENBERG CS, PATTON HM, et al. AGA clinical practice update: Coagulation in cirrhosis[J]. Gastroenterology, 2019, 157( 1): 34- 43. e 1. DOI: 10.1053/j.gastro.2019.03.070. [19] NORTHUP PG, GARCIA-PAGAN JC, GARCIA-TSAO G, et al. Vascular liver disorders, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the American association for the study of liver diseases[J]. Hepatology, 2021, 73( 1): 366- 413. DOI: 10.1002/hep.31646. [20] SIMONETTO DA, SINGAL AK, GARCIA-TSAO G, et al. ACG clinical guideline: Disorders of the hepatic and mesenteric circulation[J]. Am J Gastroenterol, 2020, 115( 1): 18- 40. DOI: 10.14309/ajg.0000000000000486. [21] National Clinical Guideline Centre(UK). Blood Transfusion[M]. London: National Institute for Health and Care Excellence(NICE), 2015. [22] ANDRIULLI A, TRIPODI A, ANGELI P, et al. Hemostatic balance in patients with liver cirrhosis: Report of a consensus conference[J]. Dig Liver Dis, 2016, 48( 5): 455- 467. DOI: 10.1016/j.dld.2016.02.008. [23] REIBERGER T, PÜSPÖK A, SCHODER M, et al. Austrian consensus guidelines on the management and treatment of portal hypertension(Billroth III)[J]. Wien Klin Wochenschr, 2017, 129( Suppl 3): 135- 158. DOI: 10.1007/s00508-017-1262-3. [24] TRIPODI A, MANNUCCI PM. The coagulopathy of chronic liver disease[J]. N Engl J Med, 2011, 365( 2): 147- 156. DOI: 10.1056/NEJMra1011170. [25] LISMAN T, BONGERS TN, ADELMEIJER J, et al. Elevated levels of von Willebrand Factor in cirrhosis support platelet adhesion despite reduced functional capacity[J]. Hepatology, 2006, 44( 1): 53- 61. DOI: 10.1002/ hep.21231. [26] NAPOLITANO G, IACOBELLIS A, MERLA A, et al. Bleeding after invasive procedures is rare and unpredicted by platelet counts in cirrhotic patients with thrombocytopenia[J]. Eur J Intern Med, 2017, 38: 79- 82. DOI: 10.1016/j.ejim.2016.11.007. -

 本文二维码
本文二维码
计量
- 文章访问数: 403
- HTML全文浏览量: 258
- PDF下载量: 120
- 被引次数: 0

