
 PDF下载 ( 737 KB)
PDF下载 ( 737 KB)

肝纤维化4因子指数及肝脏瞬时弹性成像在社区代谢相关脂肪性肝病肝纤维化危险分层中的应用价值
DOI: 10.12449/JCH260610
Application value of fibrosis-4 index and liver transient elastography in liver fibrosis risk stratification for metabolic associated fatty liver disease in community health institutions
-
摘要:
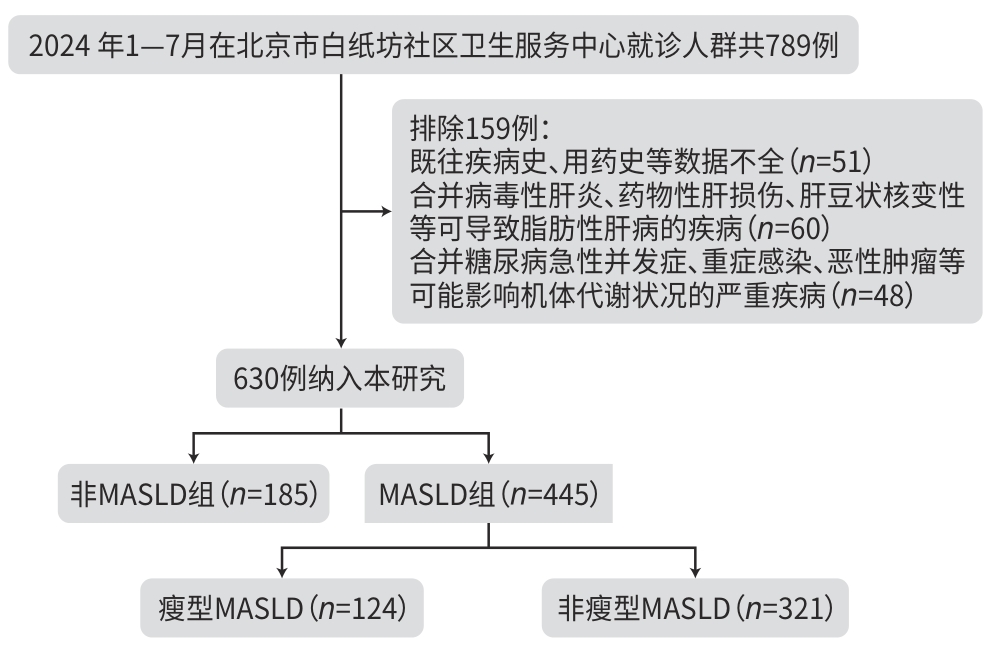
目的 旨在对社区卫生机构就诊人群进行代谢相关脂肪性肝病(MAFLD)筛查,通过肝纤维化4因子指数(FIB-4)及肝脏瞬时弹性成像检测肝脏硬度值(LSM),以识别进展期肝纤维化低、中、高危患者,并实施分层管理。 方法 选取2024年1—7月北京市白纸坊社区卫生机构630例就诊人群进行横断面研究,将患者分为MAFLD组和非MAFLD组,按照体重指数(BMI)进一步将MAFLD组分为瘦型MAFLD组(BMI<23 kg/m2)和非瘦型MAFLD组(BMI≥23 kg/m2),比较各组人口学特征、实验室指标、肝脂肪变性及LSM等。通过FIB-4和LSM对MAFLD患者进行肝纤维化危险分层,并对患者实施上级医院转诊与社区卫生机构随访的闭环管理。非正态分布的计量资料两组间比较采用Mann-Whitney U检验,计数资料组间比较采用χ2检验或Fisher精确检验。 结果 本研究中MAFLD组为445例(70.6%),非MAFLD组为185例(29.4%)。与非MAFLD组相比,MAFLD组男性占比(χ2=4.299)及高密度脂蛋白胆固醇水平(Z=3.484)显著降低,而体重(Z=-7.366)、BMI(Z=-9.740)、腰围(Z=-6.397)、臀围(Z=-6.935)、丙氨酸氨基转移酶(Z=-2.765)、空腹血糖(Z=-3.646)、甘油三酯(Z=-6.569)、总胆固醇(Z=-2.033)、低密度脂蛋白胆固醇(Z=-2.935)、受控衰减参数(Z=-19.784)、LSM(Z=-5.703)显著升高,差异均有统计学意义(P值均<0.05)。在MAFLD组中,瘦型MAFLD组124例(27.9%),非瘦型MAFLD组321例(72.1%)。瘦型MAFLD组体重(Z=-12.414)、BMI(Z=-16.363)、腰围(Z=-7.733)、臀围(Z=-8.595)、丙氨酸氨基转移酶(Z=-2.835)、天冬氨酸氨基转移酶(Z=-1.972)、甘油三酯(Z=-2.407)、受控衰减参数(Z=-4.429)、脂肪变程度(χ2=16.588)和LSM(Z=-3.908)显著低于非瘦型MAFLD组,差异均有统计学意义(P值均<0.05)。基于FIB-4及LSM的检测结果,76例肝纤维化中、高危患者应转诊至上级医院继续治疗。 结论 在社区卫生机构就诊人群中,MAFLD检出率达70.6%,其中76例患者(17.1%)应转诊至上级医院。基于FIB-4和LSM建立的社区MAFLD肝纤维化危险分层及管理体系,为社区卫生机构慢病管理及转诊体系建设提供了可推广的实践路径。 Abstract:Objective To perform metabolic associated fatty liver disease (MAFLD) screening among individuals attending community health institutions, to identify the patients at a low, moderate or high risk of advanced liver fibrosis based on fibrosis-4 index (FIB-4) and liver stiffness measurement (LSM) measured by liver transient elastography, and to implement stratified management. Methods A cross-sectional study was conducted among 630 individuals attending Beijing Baizhifang Community Health Service Center from January to July 2024, and they were divided into MAFLD group and non-MAFLD group. According to body mass index (BMI), the MAFLD group was further divided into lean MAFLD group (BMI<23 kg/m2) and non-lean MAFLD group (BMI≥23 kg/m2). The above groups were compared in terms of demographic features, laboratory markers, hepatic steatosis, and LSM. Fibrosis risk stratification was performed for MAFLD patients based on FIB-4 and LSM, and a closed-loop management system involving referral to tertiary hospitals and follow-up at community health institutions was implemented. The Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups, and the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. Results There were 445 individuals (70.6%) in the MAFLD group and 185 individuals (29.4%) in the non-MAFLD group. Compared with the non-MAFLD group, the MAFLD group had a significantly lower proportion of male individuals (χ2=4.299, P<0.05), a significant reduction in the level of high-density lipoprotein cholesterol (Z=3.484, P<0.05), and significant increases in body weight (Z=-7.366, P<0.05), BMI (Z=-9.740, P<0.05), waist circumference (Z=-6.397, P<0.05), hip circumference (Z=-6.935, P<0.05), alanine aminotransferase (ALT) (Z=-2.765, P<0.05), fasting blood glucose (Z=-3.646, P<0.05), triglyceride (TG) (Z=-6.569, P<0.05), total cholesterol (Z=-2.033, P<0.05), low-density lipoprotein cholesterol (Z=-2.935, P<0.05), controlled attenuation parameter (CAP) (Z=-19.784, P<0.05), and LSM (Z=-5.703, P<0.05). Within the MAFLD group, there were 124 individuals (27.9%) in the lean MAFLD group and 321 individuals (72.1%) in the non-lean MAFLD group. Compared with the non-lean MAFLD group, the lean MAFLD group had significantly lower body weight (Z=-12.414, P<0.05), BMI (Z=-16.363, P<0.05), waist circumference (Z=-7.733, P<0.05), hip circumference (Z=-8.595, P<0.05), ALT (Z=-2.835, P<0.05), aspartate aminotransferase (Z=-1.972, P<0.05), TG (Z=-2.407, P<0.05), CAP (Z=-4.429, P<0.05), degree of steatosis (χ2=16.588, P<0.05), and LSM (Z=-3.908, P<0.05). Based on the results of FIB-4 and LSM, 76 patients at a moderate or high risk of liver fibrosis should be referred to a higher-level hospital for further management. Conclusion The detection rate of MAFLD reaches 70.6% among the individuals attending community health institutions, among whom 76 (17.1%) should be referred to a higher-level hospital. Establishing a liver fibrosis risk stratification and management system based on FIB-4 and LSM among MAFLD individuals in communities provides a practical pathway for chronic disease management and referral system construction in community health institutions. -
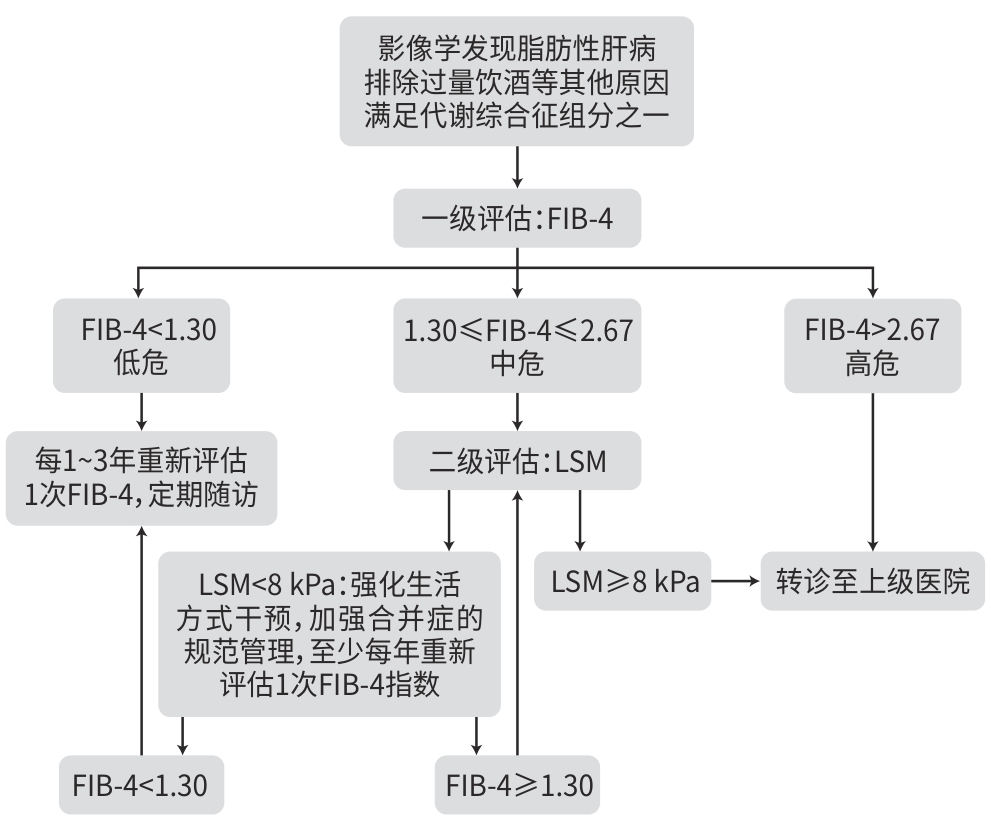
注: FIB-4,肝纤维化4因子指数;LSM,肝脏硬度值。
图 1 白纸坊社区与佑安医院联合转诊及管理流程图
Figure 1. Flow chart of joint referral and management between Baizhifang Community and You’an Hospital
表 1 按MAFLD分层的患者特征、临床指标及合并症情况比较
Table 1. Patient characteristics, clinical indicators, and comorbidities stratified by MAFLD
指标 MAFLD组(n=445) 非MAFLD组(n=185) 统计值 P值 年龄(岁) 69.0(66.0~73.0) 70.0(67.0~74.0) Z=1.893 0.058 男性[例(%)] 186(41.8) 94(50.8) χ2=4.299 0.038 体重(kg) 69.2(60.6~76.8) 61.1(55.9~67.1) Z=-7.366 <0.001 BMI(kg/m2) 25.7(23.8~28.0) 22.9(21.4~24.6) Z=-9.740 <0.001 腰围(cm) 88.5(84.0~95.0) 84.0(80.0~88.5) Z=-6.397 <0.001 臀围(cm) 100.0(95.0~105.0) 95.0(90.0~98.0) Z=-6.935 <0.001 腰臀比 0.90(0.87~0.93) 0.90(0.86~0.93) Z=-1.351 0.177 PLT(×109/L) 242.0(204.0~281.0) 241.0(198.0~289.0) Z=0.374 0.709 ALT(U/L) 15.0(12.0~24.0) 15.0(11.0~19.0) Z=-2.765 0.006 AST(U/L) 19.0(16.0~23.0) 18.0(16.0~21.0) Z=-1.337 0.181 空腹血糖(mmol/L) 6.8(5.9~8.1) 6.2(5.3~7.8) Z=-3.646 <0.001 糖化血红蛋白(%) 6.7(6.2~7.5) 6.6(6.2~7.4) Z=-0.755 0.450 TG(mmol/L) 1.4(1.0~1.9) 1.0(0.7~1.5) Z=-6.569 <0.001 TC(mmol/L) 4.4(3.8~5.3) 4.3(3.8~4.9) Z=-2.033 0.042 HDL-C(mmol/L) 1.5(1.3~1.8) 1.6(1.4~1.9) Z=3.484 0.001 LDL-C(mmol/L) 2.7(2.1~3.4) 2.4(2.0~3.0) Z=-2.935 0.003 CAP(dB/m) 300.0(277.0~328.0) 216.0(190.0~234.0) Z=-19.784 <0.001 LSM(kPa) 5.2(4.3~6.7) 4.4(3.6~5.4) Z=-5.703 <0.001 高血压[例(%)] 375(84.3) 146(78.9) χ2=2.615 0.106 2型糖尿病[例(%)] 396(89.0) 159(85.9) χ2=1.154 0.283 注:MAFLD,代谢相关脂肪性肝病;BMI,体重指数;PLT,血小板;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;TG,甘油三酯;TC,总胆固醇;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;CAP,受控衰减参数;LSM,肝脏硬度值。
 下载: 导出CSV
下载: 导出CSV
表 2 按BMI分层的患者特征、临床指标及合并症
Table 2. Patient characteristics, clinical indicators, and comorbidities stratified by BMI
指标 瘦型MAFLD组(n=124) 非瘦型MAFLD组(n=321) 统计值 P值 年龄(岁) 69.0(66.0~73.0) 69.0(66.0~73.0) Z=0.874 0.382 男性[例(%)] 44(35.5) 142(44.2) χ2=2.817 0.093 体重(kg) 58.6(55.0~63.2) 72.5(66.0~79.7) Z=-12.414 <0.001 BMI(kg/m2) 22.6(21.5~23.3) 27.0(25.3~29.0) Z=-16.363 <0.001 腰围(cm) 85.0(82.0~88.5) 90.0(86.0~97.0) Z=-7.733 <0.001 臀围(cm) 95.0(90.0~98.0) 100.0(96.0~108.0) Z=-8.595 <0.001 腰臀比 0.90(0.86~0.93) 0.90(0.88~0.94) Z=-1.425 0.154 PLT(×109/L) 249.0(205.0~284.0) 238.0(203.0~280.0) Z=1.567 0.117 ALT(U/L) 14.0(11.0~20.0) 16.0(13.0~25.0) Z=-2.835 0.005 AST(U/L) 18.0(16.0~21.0) 19.0(16.0~24.0) Z=-1.972 0.049 空腹血糖(mmol/L) 6.5(5.7~8.2) 6.9(6.0~8.1) Z=-1.461 0.144 糖化血红蛋白(%) 6.5(6.2~7.2) 6.8(6.2~7.5) Z=-1.553 0.121 TG(mmol/L) 1.3(1.0~1.7) 1.4(1.0~1.9) Z=-2.407 0.016 TC(mmol/L) 4.4(3.9~5.3) 4.4(3.8~5.3) Z=0.251 0.802 HDL-C(mmol/L) 1.6(1.3~1.8) 1.5(1.3~1.8) Z=1.436 0.151 LDL-C(mmol/L) 2.7(2.2~3.3) 2.7(2.1~3.4) Z=-0.081 0.935 CAP(dB/m) 289.0(268.0~308.0) 306.0(283.0~333.0) Z=-4.429 <0.001 CAP分组[例(%)] χ2=16.588 <0.001 248 dB/m≤CAP<268 dB/m 31(25.0) 47(14.6) 268 dB/m≤CAP<294 dB/m 40(32.3) 69(21.5) ≥294 dB/m 53(42.7) 205(63.9) LSM(kPa) 4.8(4.1~5.7) 5.4(4.3~6.9) Z=-3.908 <0.001 高血压[例(%)] 102(82.2) 273(85.0) χ2=0.525 0.469 2型糖尿病[例(%)] 108(87.1) 288(89.7) χ2=0.628 0.428 注:MAFLD,代谢相关脂肪性肝病;BMI,体重指数;PLT,血小板;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;TG,甘油三酯;TC,总胆固醇;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;CAP,受控衰减参数;LSM,肝脏硬度值。
下载: 导出CSV
表 3 FIB-4及LSM评估MAFLD患者进展期肝纤维化风险
Table 3. Assessment of the risk of advanced fibrosis using FIB-4 and LSM in MAFLD patients
指标 MAFLD组 瘦型MAFLD组 非瘦型MAFLD组 P值 年龄≤65岁 0.782 FIB-4<1.30 62/92(67.4%) 17/23(73.9%) 45/69(65.2%) 1.30≤FIB-4≤2.67 28/92(30.4%) 6/23(26.1%) 22/69(31.9%) 2.67<FIB-4<3.48 2/92(2.2%) 0/23(0.0) 2/69(2.9%) ≥3.48 0/92(0.0) 0/23(0.0) 0/69(0.0) 年龄>65岁 0.430 FIB-4<2.0 293/353(83.0%) 88/101(87.1%) 205/252(81.3%) 2.0≤FIB-4≤2.67 43/353(12.2%) 9/101(8.9%) 34/252(13.5%) 2.67<FIB-4<3.48 13/353(3.7%) 4/101(4.0%) 9/252(3.6%) ≥3.48 4/353(1.1%) 0/101(0.0) 4/252(1.6%) LSM(kPa) <0.001 <8 384/445(86.3%) 120/124(96.8%) 264/321(82.2%) 8~≤12 46/445(10.3%) 2/124(1.6%) 44/321(13.7%) 12~<20 9/445(2.0%) 2/124(1.6%) 7/321(2.2%) ≥20 6/445(1.4%) 0/124(0.0) 6/321(1.9%) 注:FIB-4,肝纤维化4因子指数;LSM,肝脏硬度值;MAFLD,代谢相关脂肪性肝病。
下载: 导出CSV
-
[1] Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of metabolic dysfunction-associated(non-alcoholic) fatty liver disease(version 2024)[J]. J Pract Hepatol, 2024, 27( 4): 494- 510. DOI: 10.3760/cma.j.cn501113-20240327-00163.中华医学会肝病学分会. 代谢相关(非酒精性)脂肪性肝病防治指南(2024年版)[J]. 实用肝脏病杂志, 2024, 27( 4): 494- 510. DOI: 10.3760/cma.j.cn501113-20240327-00163. [2] LOU TW, YANG RX, FAN JG. The global burden of fatty liver disease: The major impact of China[J]. Hepatobiliary Surg Nutr, 2024, 13( 1): 119- 123. DOI: 10.21037/hbsn-23-556. [3] YIP TC, LEE HW, LIN HP, et al. Prognostic performance of the two-step clinical care pathway in metabolic dysfunction-associated steatotic liver disease[J]. J Hepatol, 2025, 83( 2): 304- 314. DOI: 10.1016/j.jhep.2025.01.014. [4] BOURSIER J, HAGSTRÖM H, EKSTEDT M, et al. Non-invasive tests accurately stratify patients with NAFLD based on their risk of liver-related events[J]. J Hepatol, 2022, 76( 5): 1013- 1020. DOI: 10.1016/j.jhep.2021.12.031. [5] Beijing Municipal Health Commission. Notice on further deepening the development of specialized disease clinics in community health service institutions[EB/OL].( 2022-07-07)[ 2025-04-17]. https://wjw.beijing.gov.cn/zwgk_20040/ylws/202207/t20220707_2766088.html. https://wjw.beijing.gov.cn/zwgk_20040/ylws/202207/t20220707_2766088.html北京市卫生健康委员会. 关于进一步深化社区卫生服务机构专病特色科室建设工作的通知[EB/OL].( 2022-07-07)[ 2025-04-17]. https://wjw.beijing.gov.cn/zwgk_20040/ylws/202207/t20220707_2766088.html. https://wjw.beijing.gov.cn/zwgk_20040/ylws/202207/t20220707_2766088.html [6] European Association for the Study of the Liver(EASL), European Association for the Study of Diabetes(EASD), European Association for the Study of Obesity(EASO). EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease(MASLD)[J]. J Hepatol, 2024, 81( 3): 492- 542. DOI: 10.1016/j.jhep.2024.04.031. [7] European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis-2021 update[J]. J Hepatol, 2021, 75( 3): 659- 689. DOI: 10.1016/j.jhep.2021.05.025. [8] WATTACHERIL JJ, ABDELMALEK MF, LIM JK, et al. AGA clinical practice update on the role of noninvasive biomarkers in the evaluation and management of nonalcoholic fatty liver disease: Expert review[J]. Gastroenterology, 2023, 165( 4): 1080- 1088. DOI: 10.1053/j.gastro.2023.06.013. [9] GRAUPERA I, THIELE M, SERRA-BURRIEL M, et al. Low accuracy of FIB-4 and NAFLD fibrosis scores for screening for liver fibrosis in the population[J]. Clin Gastroenterol Hepatol, 2022, 20( 11): 2567- 2576.e6. DOI: 10.1016/j.cgh.2021.12.034. [10] Chronic Disease Management Branch of China Medical Biotechnology Association, Chinese Research Hospital Society(Integrated Chinese and Western Medicine), Chinese Society of General Practice, et al. Guideline for diagnosis and management of metabolic dysfunction-associated fatty liver disease in primary care(2025)[J]. Chin J Gen Pract, 2025, 24( 5): 513- 525. DOI: 10.3760/cma.j.cn114798-20241021-00829.中国医药生物技术协会慢病管理分会, 中国研究型医院学会肝病(中西医结合)专业委员会, 中华医学会全科医学分会, 等. 代谢相关脂肪性肝病基层诊疗与管理指南(2025年)[J]. 中华全科医师杂志, 2025, 24( 5): 513- 525. DOI: 10.3760/cma.j.cn114798-20241021-00829. [11] MAN S, DENG YH, MA Y, et al. Prevalence of liver steatosis and fibrosis in the general population and various high-risk populations: A nationwide study with 5.7 million adults in China[J]. Gastroenterology, 2023, 165( 4): 1025- 1040. DOI: 10.1053/j.gastro.2023.05.053. [12] GUO HQ, LI ML, LIU F, et al. Prevalence, influencing factors, and fibrosis risk stratification of metabolic dysfunction-associated fatty liver disease in the health check-up population in Beijing, China[J]. J Clin Hepatol, 2025, 41( 4): 643- 649. DOI: 10.12449/JCH250408.郭海清, 李明亮, 刘峰, 等. 北京市体检人群代谢相关脂肪性肝病的患病率、影响因素和纤维化风险分层分析[J]. 临床肝胆病杂志, 2025, 41( 4): 643- 649. DOI: 10.12449/JCH250408. [13] QIU YS, XIE WN, LI CY, et al. Diagnostic value of ultrasound elastography combined with APRI in liver fibrosis of patients with metabolic dysfunction-associated fatty liver disease[J]. Clin Misdiagnosis Mistherapy, 2025, 38( 24): 62- 68. DOI: 10.3969/j.issn.1002-3429.2025.24.010.邱燕生, 谢维宁, 李彩妍, 等. 超声弹性成像联合APRI对代谢相关脂肪性肝病肝纤维化的诊断价值[J]. 临床误诊误治, 2025, 38( 24): 62- 68. DOI: 10.3969/j.issn.1002-3429.2025.24.010. [14] CHEN XN, GOH GB, HUANG JF, et al. Validation of non-invasive fibrosis scores for predicting advanced fibrosis in metabolic-associated fatty liver disease[J]. J Clin Transl Hepatol, 2022, 10( 4): 589- 594. DOI: 10.14218/JCTH.2021.00311. [15] WU YL, KUMAR R, WANG MF, et al. Validation of conventional non-invasive fibrosis scoring systems in patients with metabolic associated fatty liver disease[J]. World J Gastroenterol, 2021, 27( 34): 5753- 5763. DOI: 10.3748/wjg.v27.i34.5753. [16] SHEN F, MI YQ, XU L, et al. Moderate to severe hepatic steatosis leads to overestimation of liver stiffness measurement in chronic hepatitis B patients without significant fibrosis[J]. Aliment Pharmacol Ther, 2019, 50( 1): 93- 102. DOI: 10.1111/apt.15298. [17] CHAN WK, TREEPRASERTSUK S, GOH GB, et al. Optimizing use of nonalcoholic fatty liver disease fibrosis score, fibrosis-4 score, and liver stiffness measurement to identify patients with advanced fibrosis[J]. Clin Gastroenterol Hepatol, 2019, 17( 12): 2570- 2580.e37. DOI: 10.1016/j.cgh.2019.03.006. [18] PUIGVEHÍ M, BROQUETAS T, COLL S, et al. Impact of anthropometric features on the applicability and accuracy of FibroScan®(M and XL) in overweight/obese patients[J]. J Gastroenterol Hepatol, 2017, 32( 10): 1746- 1753. DOI: 10.1111/jgh.13762. [19] BLANCO-GRAU A, GABRIEL-MEDINA P, RODRIGUEZ-ALGARRA F, et al. Assessing liver fibrosis using the FIB4 index in the community setting[J]. Diagnostics, 2021, 11( 12): 2236. DOI: 10.3390/diagnostics11122236. [20] ZHANG XR, YIP TC, WONG GL, et al. Clinical care pathway to detect advanced liver disease in patients with type 2 diabetes through automated fibrosis score calculation and electronic reminder messages: A randomised controlled trial[J]. Gut, 2023, 72( 12): 2364- 2371. DOI: 10.1136/gutjnl-2023-330269. [21] PAPADAKIS S, ANASTASAKI M, GERGIANAKI I, et al. Development and implementation of a continuing medical education program on non-alcoholic fatty liver disease for primary care practitioners in Europe[J]. Front Med, 2023, 10: 1034626. DOI: 10.3389/fmed.2023.1034626. [22] DECHARATANACHART P, CHAITEERAKIJ R, TIYARATTANACHAI T, et al. Application of artificial intelligence in non-alcoholic fatty liver disease and liver fibrosis: A systematic review and meta-analysis[J]. Ther Adv Gastroenterol, 2021, 14: 17562848211062807. DOI: 10.1177/17562848211062807. -

 本文二维码
本文二维码
计量
- 文章访问数: 5
- HTML全文浏览量: 0
- PDF下载量: 1
- 被引次数: 0

