
 PDF下载 ( 920 KB)
PDF下载 ( 920 KB)

仑伐替尼联合信迪利单抗与阿替利珠单抗联合贝伐珠单抗治疗不可切除肝细胞癌的效果及安全性分析
DOI: 10.12449/JCH260615
Efficacy and safety of lenvatinib combined with sintilimab versus atezolizumab combined with bevacizumab in treatment of unresectable hepatocellular carcinoma
-
摘要:
目的 比较仑伐替尼联合信迪利单抗与阿替利珠单抗联合贝伐珠单抗在不可切除肝细胞癌(uHCC)患者中的疗效及安全性差异,为临床个体化治疗提供真实世界证据。 方法 回顾性纳入2023年1月1日—2025年5月31日首都医科大学附属北京地坛医院收治的78例uHCC患者为研究对象,根据治疗方式将其分为两组:接受仑伐替尼联合信迪利单抗治疗者(L+S组,n=49)、接受阿替利珠单抗联合贝伐珠单抗治疗者(A+T组,n=29)。主要终点为无进展生存期(PFS)、总生存期(OS),次要终点包括客观缓解率(ORR)、疾病控制率(DCR)和不良反应发生率。符合正态分布的计量资料两组间比较采用成组t检验;非正态分布计量资料的两组间比较采用Mann-Whitney U检验;计数资料两组间比较采用χ2检验。应用Kaplan-Meier法进行生存分析,组间比较采用Log-rank检验。 结果 78例患者的中位PFS、OS分别为9个月、15个月,其中L+S组、A+T组的中位PFS分别为11个月、7个月,差异无统计学意义(χ2=0.247,P=0.619);L+S组、A+T组的中位OS分别为19个月、12个月,差异有统计学意义(χ2=6.565,P=0.010)。两组患者的完全缓解、部分缓解、疾病稳定、疾病进展、DCR和ORR比较,差异均无统计学意义(P值均>0.05)。L+S组患者的不良反应发生率为95.9%,显著高于A+T组的75.9%,差异有统计学意义(P=0.007);其中,L+S组和A+T组3级以上不良反应发生率分别为65.3%和34.5%,差异有统计学意义(P=0.008)。 结论 与阿替利珠单抗联合贝伐珠单抗相比,仑伐替尼联合信迪利单抗可提高uHCC患者的OS,但阿替利珠单抗联合贝伐珠单抗的安全性更好。 Abstract:Objective To investigate the efficacy and safety of lenvatinib combined with sintilimab versus atezolizumab combined with bevacizumab in patients with unresectable hepatocellular carcinoma (uHCC), aims to provide real-world evidence for clinical personalized treatment. Methods A retrospective analysis was performed for 78 patients with uHCC who were admitted to Beijing Ditan Hospital, Capital Medical University, from January 1, 2023, to May 31, 2025, and according to the treatment modality, they were divided into lenvatinib+sintilimab group (L+S group with 49 patients) and atezolizumab+bevacizumab group (A+T group with 29 patients). The primary endpoints were progression-free survival (PFS) and overall survival (OS), and the secondary endpoints included objective response rate (ORR), disease control rate (DCR), and the incidence rate of adverse events. The independent-samples t test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the chi-square test was used for comparison of categorical data between groups. The Kaplan-Meier method was used for survival analysis, and the log-rank test was used for comparison between groups. Results The 78 patients had a median PFS of 9 months and a median OS of 15 months. The median PFS was 11 months in the L+S group and 7 months in the A+T group, with no significant difference between the two groups (χ2=0.247, P=0.619); the median OS was 19 months in the L+S group and 12 months in the A+T group, with a significant difference between the two groups (χ2=6.565, P=0.010). There were no significant differences between the two groups in complete remission, partial remission, stable disease, disease progression, DCR, and ORR (all P>0.05). The L+S group had a significantly higher incidence rate of adverse events than the A+T group (95.9% vs 75.9%, P=0.007), and there was a significant difference in the incidence rate of grade ≥3 adverse events between the L+S group and the A+T group (65.3% vs 34.5%, P=0.008). Conclusion Compared with atezolizumab combined with bevacizumab, lenvatinib combined with sintilimab can improve the OS of patients with uHCC, while atezolizumab combined with bevacizumab has a better safety profile. -
Key words:
- Carcinoma, Hepatocellular /
- Lenvatinib /
- Sintilimab /
- Atezolizumab /
- Bevacizumab
-
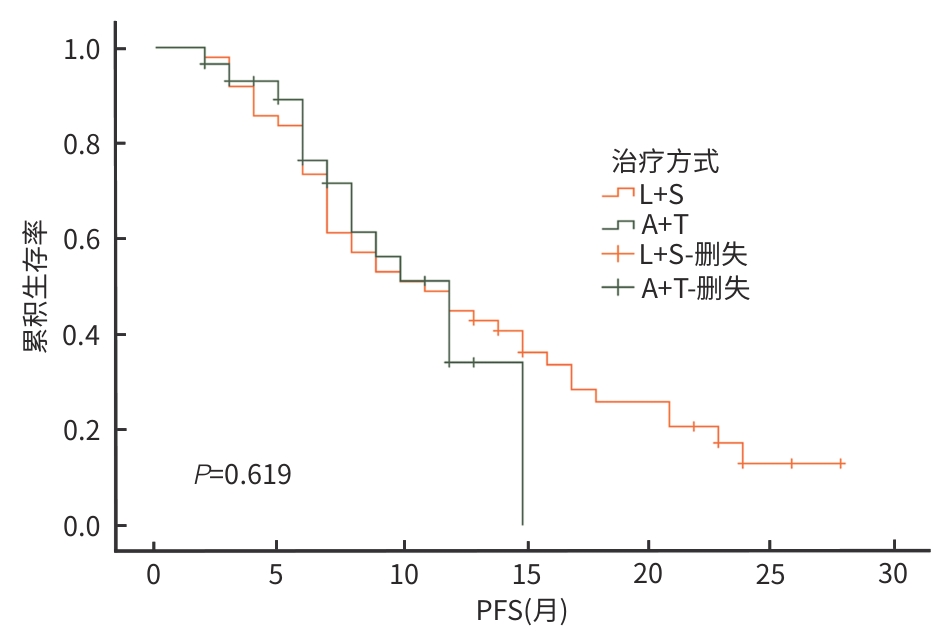
注: PFS,无进展生存期。
图 1 L+S组和A+T组患者的PFS比较
Figure 1. Comparison of PFS between the L+S group and the A+T group of patients
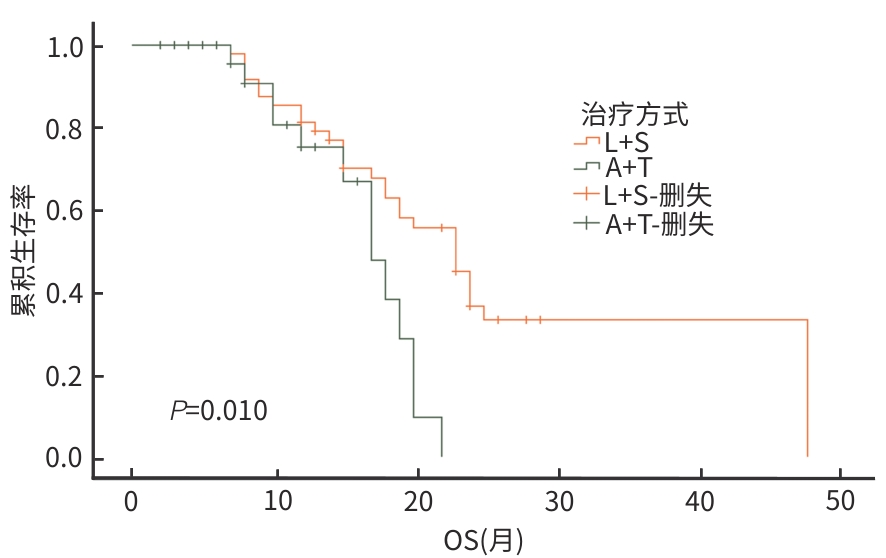
注: OS,总生存期。
图 2 L+S组和A+T组患者的OS比较
Figure 2. Comparison of OS between the L+S group and the A+T group of patients
表 1 两组患者的基线资料
Table 1. Baseline data of the two patient groups
指标 L+S组(n=49) A+T组(n=29) 统计值 P值 性别[例(%)] χ2=0.538 0.463 男 42(85.7) 23(79.3) 女 7(14.3) 6(20.7) 年龄(岁) 56.33±11.65 60.72±12.15 t=-1.586 0.117 ECOG评分[例(%)] χ2=0.148 0.700 0分 12(24.5) 6(20.7) 1分 37(75.5) 23(79.3) 既往治疗方式[例(%)] 外科手术史 2(4.1) 1(3.4) χ2=0.020 0.888 TACE史 45(91.8) 24(82.8) χ2=1.471 0.225 消融史 10(20.4) 3(10.3) χ2=1.328 0.249 嗜肝病毒感染[例(%)] χ2=0.459 0.759 HBV 41(83.7) 24(82.8) HCV 3(6.1) 1(3.4) 非HBV或HCV 5(10.2) 4(13.8) 肝硬化[例(%)] χ2=0.529 0.467 有 39(79.6) 21(72.4) 无 10(20.4) 8(27.6) Child-Pugh分级[例(%)] χ2=2.717 0.099 A级 44(89.8) 22(75.9) B级 5(10.2) 7(24.1) 肝外转移[例(%)] χ2=3.134 0.770 有 7(14.3) 9(31.0) 无 42(85.7) 20(69.0) 门静脉癌栓[例(%)] χ2=0.055 0.815 有 25(51.0) 14(48.3) 无 24(49.0) 15(51.7) CNLC分期[例(%)] χ2=4.707 0.095 1+2期 17(34.7) 10(34.5) 3a期 26(53.1) 10(34.5) 3b期 6(12.2) 9(31.0) BCLC分期[例(%)] χ2=0.011 0.916 A+B期 18(36.7) 11(37.9) C期 31(63.3) 18(62.1) AFP[例(%)] χ2=0.299 0.585 <400 ng/mL 35(71.4) 19(65.5) ≥400 ng/mL 14(28.6) 10(34.5) TBil(μmol/L) 12.50(10.05~17.55) 12.10(8.30~17.55) Z=-0.595 0.552 Alb(g/L) 37.50(36.00~41.35) 38.30(34.10~40.35) Z=-0.057 0.955 PT(s) 12.20(11.80~13.30) 12.20(11.15~12.90) Z=-1.499 0.134 WBC(×109/L) 38.11±4.42 37.22±5.30 t=0.798 0.307 注:ECOG,东部肿瘤协作组体能状态;TACE,经导管动脉栓塞化疗;HBV,乙型肝炎病毒;HCV,丙型肝炎病毒;Child-Pugh分级,蔡尔德-皮尤分级;CNLC分期,中国肝癌临床分期;BCLC分期,巴塞罗那临床肝癌分期;AFP,甲胎蛋白;TBil,总胆红素;Alb,白蛋白;PT,凝血酶原时间;WBC,白细胞。
 下载: 导出CSV
下载: 导出CSV
表 2 根据mRECIST标准评估的肿瘤反应率
Table 2. Tumor response rate assessed according to the mRECIST criteria
疗效 L+S组(n=49) A+T组(n=29) χ2值 P值 CR[例(%)] 9(18.4) 1(3.4) 3.628 0.057 PR[例(%)] 14(28.6) 9(31.0) 0.053 0.818 SD[例(%)] 19(38.8) 16(55.2) 1.980 0.159 PD[例(%)] 7(14.3) 3(10.3) 0.253 0.615 DCR(%) 85.7 89.7 0.253 0.615 ORR(%) 46.9 34.5 1.158 0.282 注:CR,完全缓解;PR,部分缓解;SD,疾病稳定;PD,疾病进展;DCR,疾病控制率;ORR,客观缓解率。
下载: 导出CSV
表 3 不良反应发生情况
Table 3. Occurrence of adverse reactions
不良事件 合计 1/2级 ≥3级 L+S组
(n=49)A+T组
(n=29)χ2值 P值 L+S组
(n=49)A+T组
(n=29)χ2值 P值 L+S组
(n=49)A+T组
(n=29)χ2值 P值 总发生率[例(%)] 47(95.9) 22(75.9) 7.180 0.007 15(30.6) 12(41.4) 0.933 0.334 32(65.3) 10(34.5) 6.965 0.008 乏力[例(%)] 12(24.5) 3(10.3) 2.347 0.126 7(14.3) 3(10.3) 0.253 0.615 5(10.2) 0(0.0) 3.162 0.075 食欲下降[例(%)] 18(36.7) 5(17.2) 3.329 0.068 12(24.5) 4(13.8) 1.278 0.258 6(12.2) 1(3.4) 1.726 0.189 高血压[例(%)] 16(32.7) 7(24.1) 0.635 0.425 9(18.4) 5(17.2) 0.016 0.900 7(14.3) 2(6.9) 0.975 0.324 蛋白尿[例(%)] 13(26.5) 9(31.0) 0.182 0.669 10(20.4) 8(27.6) 0.529 0.467 3(6.1) 1(3.4) 0.268 0.605 腹泻[例(%)] 11(22.4) 1(3.4) 5.052 0.025 9(18.4) 1(3.4) 3.628 0.057 2(4.1) 0(0.0) 1.241 0.270 皮疹[例(%)] 3(6.1) 0(0.0) 1.847 0.174 2(4.1) 0(0.0) 1.215 0.27 1(2.0) 0(0.0) 0.600 0.439 肝功能异常[例(%)] 15(30.6) 3(10.3) 4.216 0.040 11(22.4) 1(3.4) 5.052 0.025 4(8.2) 2(6.9) 0.041 0.839 甲状腺功能减退[例(%)] 10(20.4) 0(0.0) 6.789 0.009 9(18.4) 0(0.0) 6.021 0.014 1(2.0) 0(0.0) 0.600 0.439 手足综合征[例(%)] 7(14.3) 0(0.0) 4.551 0.033 4(8.2) 0(0.0) 2.495 0.114 3(6.1) 0(0.0) 1.847 0.174 消化道出血[例(%)] 1(2.0) 3(10.3) 2.582 0.108 0(0.0) 0(0.0) — — 1(2.0) 3(10.3) 2.582 0.108 肾上腺功能减退[例(%)] 1(2.0) 0(0.0) 0.600 0.439 0(0.0) 0(0.0) — — 1(2.0) 0(0.0) 0.600 0.439 其他[例(%)] 10(20.4) 5(17.2) 0.118 0.732 8(16.3) 4(13.8) 0.09 0.764 2(4.1) 1(3.4) 0.020 0.888
下载: 导出CSV
-
[1] SUNG H, FERLAY J, SIEGEL RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71( 3): 209- 249. DOI: 10.3322/caac.21660. [2] YOUNOSSI ZM, WONG G, ANSTEE QM, et al. The global burden of liver disease[J]. Clin Gastroenterol Hepatol, 2023, 21( 8): 1978- 1991. DOI: 10.1016/j.cgh.2023.04.015. [3] FAN R, CHEN L, ZHAO SR, et al. Novel, high accuracy models for hepatocellular carcinoma prediction based on longitudinal data and cell-free DNA signatures[J]. J Hepatol, 2023, 79( 4): 933- 944. DOI: 10.1016/j.jhep.2023.05.039. [4] ZENG HM, CAO MM, XIA CF, et al. Performance and effectiveness of hepatocellular carcinoma screening in individuals with HBsAg seropositivity in China: A multicenter prospective study[J]. Nat Cancer, 2023, 4( 9): 1382- 1394. DOI: 10.1038/s43018-023-00618-8. [5] KUDO M, FINN RS, QIN SK, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial[J]. Lancet, 2018, 391( 10126): 1163- 1173. DOI: 10.1016/S0140-6736(18)30207-1. [6] FINN RS, IKEDA M, ZHU AX, et al. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma[J]. J Clin Oncol, 2020, 38( 26): 2960- 2970. DOI: 10.1200/JCO.20.00808. [7] LLOVET JM, KUDO M, MERLE P, et al. Lenvatinib plus pembrolizumab versus lenvatinib plus placebo for advanced hepatocellular carcinoma(LEAP-002): A randomised, double-blind, phase 3 trial[J]. Lancet Oncol, 2023, 24( 12): 1399- 1410. DOI: 10.1016/S1470-2045(23)00469-2. [8] KUDO M, IKEDA M, MOTOMURA K, et al. A phase Ib study of lenvatinib(LEN) plus nivolumab(NIV) in patients(pts) with unresectable hepatocellular carcinoma(uHCC): Study 117[J]. J Clin Oncol, 2020, 38( 4_suppl): 513. DOI: 10.1200/jco.2020.38.4_suppl.513. [9] SUN W, DING XY, CHEN JL. Efficacy and safety of anti-PD-1 monoclonal antibody combined with sorafenib or lenvatinib in treatment of patients with Child-Pugh class B unresectable hepatocellular carcinoma[J]. J Clin Hepatol, 2024, 40( 5): 975- 981. DOI: 10.12449/JCH240517.孙巍, 丁晓燕, 陈京龙. 程序性死亡受体1(PD-1)单抗联合索拉非尼或仑伐替尼治疗肝功能Child-Pugh B级不可切除肝癌患者的效果分析[J]. 临床肝胆病杂志, 2024, 40( 5): 975- 981. DOI: 10.12449/JCH240517. [10] CAI MY, HUANG WS, LIANG W, et al. Lenvatinib, sintilimab plus transarterial chemoembolization for advanced stage hepatocellular carcinoma: A phase II study[J]. Liver Int, 2024, 44( 4): 920- 930. DOI: 10.1111/liv.15831. [11] FINN RS, QIN SK, IKEDA M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma[J]. N Engl J Med, 2020, 382( 20): 1894- 1905. DOI: 10.1056/NEJMoa1915745. [12] National Health Commission of the People’s Republic of China. Standard for diagnosis and treatment of primary liver cancer(2024 edition)[J]. J Clin Hepatol, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508.中华人民共和国国家卫生健康委员会. 原发性肝癌诊疗指南(2024年版)[J]. 临床肝胆病杂志, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508. [13] LENCIONI R, LLOVET JM. Modified RECIST(mRECIST) assessment for hepatocellular carcinoma[J]. Semin Liver Dis, 2010, 30( 1): 52- 60. DOI: 10.1055/s-0030-1247132. [14] U.S. Department of Health& Human Services. CTCAE5.0[EB/OL]. https://ctep.cancer.gov/protocoldevelopment/electronicapplications/ctc.htm. https://ctep.cancer.gov/protocoldevelopment/electronicapplications/ctc.htm [15] de CASTRIA TB, KHALIL DN, HARDING JJ, et al. Tremelimumab and durvalumab in the treatment of unresectable, advanced hepatocellular carcinoma[J]. Future Oncol, 2022, 18( 33): 3769- 3782. DOI: 10.2217/fon-2022-0652. [16] ZHU MY, LIU ZL, CHEN SL, et al. Sintilimab plus bevacizumab combined with radiotherapy as first-line treatment for hepatocellular carcinoma with portal vein tumor thrombus: A multicenter, single-arm, phase 2 study[J]. Hepatology, 2024, 80( 4): 807- 815. DOI: 10.1097/HEP.0000000000000776. [17] CASADEI-GARDINI A, RIMINI M, TADA T, et al. Atezolizumab plus bevacizumab versus lenvatinib for unresectable hepatocellular carcinoma: A large real-life worldwide population[J]. Eur J Cancer, 2023, 180: 9- 20. DOI: 10.1016/j.ejca.2022.11.017. [18] VITIELLO F, TADA T, SUDA G, et al. Atezolizumab plus bevacizumab versus Lenvatinib for patients with Barcelona clinic liver cancer stage B(BCLC-B) hepatocellular carcinoma(HCC): A real-world population[J]. Semin Oncol, 2025, 52( 4): 152348. DOI: 10.1016/j.seminoncol.2025.152348. [19] REMITHA NPSI, DEWI NPRP, KUSUMA IKWA, et al. Efficacy and safety of lenvatinib versus atezolizumab plus bevacizumab in the treatment of unresectable hepatocellular carcinoma: A systematic review and meta-analysis[J]. Asian Pac J Cancer Prev, 2025, 26( 5): 1529- 1542. DOI: 10.31557/APJCP.2025.26.5.1529. [20] KIM HD, PARK YG, HONG H, et al. Atezolizumab plus bevacizumab is associated with favorable overall survival over lenvatinib in patients with unresectable hepatocellular carcinoma[J]. Oncology, 2026, 104( 1): 40- 50. DOI: 10.1159/000545351. [21] LEE MS, RYOO BY, HSU CH, et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma(GO30140): An open-label, multicentre, phase 1b study[J]. Lancet Oncol, 2020, 21( 6): 808- 820. DOI: 10.1016/S1470-2045(20)30156-X. [22] TOHYAMA O, MATSUI J, KODAMA K, et al. Antitumor activity of lenvatinib(E7080): An angiogenesis inhibitor that targets multiple receptor tyrosine kinases in preclinical human thyroid cancer models[J]. J Thyroid Res, 2014, 2014: 638747. DOI: 10.1155/2014/638747. [23] ZHU YJ, WANG MM, ZHAO SJ, et al. Determination of the earliest time point for efficacy evaluation of transarterial chemoembolization combined with lenvatinib in patients with unresectable hepatocellular carcinoma based on imaging evaluation methods[J]. Clin J Med Offic, 2024, 52( 11): 1123- 1128. DOI: 10.16680/j.1671-3826.2024.11.05.祝叶静, 汪檬檬, 赵首捷, 等. 基于影像学评价手段确定经肝动脉化疗栓塞术联合仑伐替尼治疗不可切除肝细胞癌患者疗效评估最早时间节点[J]. 临床军医杂志, 2024, 52( 11): 1123- 1128. DOI: 10.16680/j.1671-3826.2024.11.05. [24] ADACHI Y, KAMIYAMA H, ICHIKAWA K, et al. Inhibition of FGFR reactivates IFNγ signaling in tumor cells to enhance the combined antitumor activity of lenvatinib with anti-PD-1 antibodies[J]. Cancer Res, 2022, 82( 2): 292- 306. DOI: 10.1158/0008-5472.CAN-20-2426. [25] KATO Y. Lenvatinib enhances antitumor immunity of anti-PD-1 antibody[J]. Int J Clin Oncol, 2025, 30( 4): 666- 673. DOI: 10.1007/s10147-025-02721-5. -

 本文二维码
本文二维码
计量
- 文章访问数: 8
- HTML全文浏览量: 1
- PDF下载量: 1
- 被引次数: 0

