
 PDF下载 ( 1561 KB)
PDF下载 ( 1561 KB)

血清高尔基体蛋白73、缺氧诱导因子-1α及基质金属蛋白酶-9对乙型肝炎病毒相关肝细胞癌经导管肝动脉化疗栓塞治疗效果的预测价值
DOI: 10.12449/JCH260616
Value of serum Golgi protein 73, hypoxia-inducible factor-1α, and matrix metalloproteinase-9 in predicting the efficacy of transcatheter arterial chemoembolization in treatment of hepatitis B virus-related hepatocellular carcinoma
-
摘要:
目的 探讨乙型肝炎病毒(HBV)相关肝细胞癌(HCC)患者经导管动脉化疗栓塞术(TACE)治疗前后血清高尔基体蛋白73(GP73)、缺氧诱导因子-1α(HIF-1α)及基质金属蛋白酶-9(MMP-9)水平与疗效的关系。 方法 选取2023年1月—2025年10月在新疆医科大学第一附属医院首次接受TACE治疗的135例HBV相关HCC患者为研究对象,分别于TACE术前及术后1个月检测患者血清GP73、HIF-1α及MMP-9水平,术后根据疗效将患者分为缓解组与未缓解组。比较两组患者一般资料、治疗前后血清GP73、HIF-1α及MMP-9水平,采用Logistic回归分析TACE疗效的影响因素,采用受试者操作特征(ROC)曲线评估治疗前GP73、HIF-1α、MMP-9及其联合对TACE疗效的预测价值。计量资料两组间比较采用成组t检验,计数资料两组间比较采用χ2检验。 结果 治疗后,135例患者中缓解组78例(57.78%),未缓解组57例(42.22%)。治疗前,缓解组患者血清GP73、HIF-1α和MMP-9水平均显著低于未缓解组(P值均<0.05);治疗后,两组血清GP73、HIF-1α、MMP-9水平均较治疗前有所降低,且缓解组显著低于未缓解组(P值均<0.05)。二元Logistic回归分析显示,治疗前血清GP73、HIF-1α和MMP-9水平升高是影响TACE疗效的独立危险因素(P值均<0.05)。ROC曲线分析结果显示,治疗前血清GP73、HIF-1α和MMP-9水平单独预测TACE疗效的曲线下面积(AUC)分别为0.799、0.835和0.777,其中HIF-1α的预测价值最高;三者联合检测的AUC为0.950,约登指数为0.787,最佳临界值为0.39,敏感度为87.72%,特异度为91.03%。 结论 TACE治疗可降低HBV相关HCC患者血清GP73、HIF-1α及MMP-9水平,且疗效良好的患者下降更为显著。治疗前高水平的血清GP73、HIF-1α及MMP-9是TACE近期疗效不佳的独立危险因素,三者联合检测对TACE疗效具有较高的预测价值。 -
关键词:
- 乙型肝炎病毒 /
- 癌, 肝细胞 /
- 经导管动脉化疗栓塞术 /
- 高尔基体蛋白73 /
- 缺氧诱导因子1, α亚基 /
- 基质金属蛋白酶9
Abstract:Objective To investigate the association of the serum levels of Golgi protein 73 (GP73), hypoxia-inducible factor-1α (HIF-1α), and matrix metalloproteinase-9 (MMP-9) before and after transcatheter arterial chemoembolization (TACE) with the treatment outcome of patients with hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC). Methods A total of 135 patients with HBV-related HCC who received TACE for the first time in The First Affiliated Hospital of Xinjiang Medical University from January 2023 to October 2025 were enrolled as subjects, and the serum levels of GP73, HIF-1α, and MMP-9 were measured before TACE and at 1 month after TACE. According to the treatment outcome after TACE, the patients were divided into remission group and non-remission group. The two groups were compared in terms of general information and the serum levels of GP73, HIF-1α, and MMP-9 before and after treatment. The Logistic regression analysis was used to investigate the influencing factors for the efficacy of TACE, and the receiver operating characteristic (ROC) curve was used to assess the value of the serum levels of GP73, HIF-1α, and MMP-9 before treatment used alone or in combination in predicting the efficacy of TACE. The independent-samples t test was used for comparison of continuous data between two groups, and the chi-square test was used for comparison of categorical data between two groups. Results Among the 135 patients after treatment, 78 (57.78%) were enrolled in the remission group and 57 (42.22%) were enrolled in the non-remission group. Before treatment, the remission group had significantly lower serum levels of GP73, HIF-1α, and MMP-9 than the non-remission group (all P<0.05); after treatment, both groups had reductions in the serum levels of GP73, HIF-1α, and MMP-9, and the remission group had significantly lower levels than the non-remission group (all P<0.05). The binary Logistic regression analysis showed that increases in the serum levels of GP73, HIF-1α, and MMP-9 before treatment were independent influencing factors for the efficacy of TACE (all P<0.05). The ROC curve analysis showed that the serum levels of GP73, HIF-1α, and MMP-9 before treatment used alone had an area under the ROC curve (AUC) of 0.799, 0.835, and 0.777, respectively, in predicting the efficacy of TACE, among which HIF-1α showed the highest predictive value, and the combination of these three indicators had an AUC of 0.950, a Youden index of 0.787, an optimal cut-off value of 0.39, a sensitivity of 87.72%, and a specificity of 91.03%. Conclusion TACE can reduce the serum levels of GP73, HIF-1α, and MMP-9 in patients with HBV-related HCC, and patients with a good outcome tend to have greater reductions. The high serum levels of GP73, HIF-1α, and MMP-9 before treatment are independent risk factors for poor short-term efficacy of TACE, and the combination of these three indicators has a relatively high value in predicting the efficacy of TACE. -
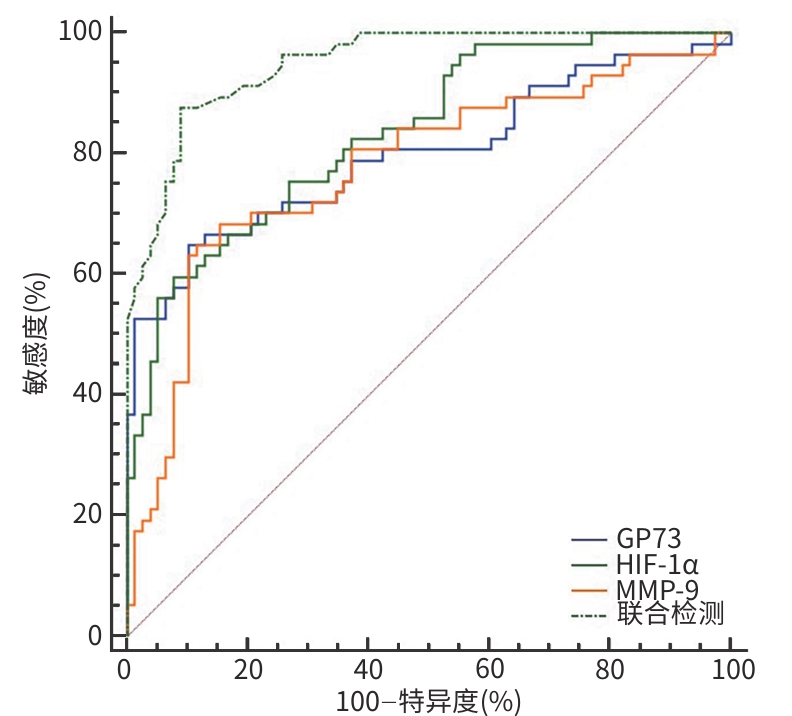
注: GP73,高尔基体蛋白73;HIF-1α,缺氧诱导因子-1α;MMP-9,基质金属蛋白酶-9;TACE,经导管动脉化疗栓塞术。
图 1 血清GP73、HIF-1α、MMP-9水平对TACE疗效预测价值的受试者操作特征曲线
Figure 1. ROC curves for predicting TACE efficacy based on serum GP73, HIF-1α, and MMP-9 levels
表 1 两组患者一般资料比较
Table 1. Comparison of general data between the two groups
指标 缓解组(n=78) 未缓解组(n=57) 统计值 P值 年龄(岁) 56.32±9.36 57.14±8.41 t=0.524 0.601 性别[例(%)] χ2=0.187 0.665 男 60(76.92) 42(73.68) 女 18(23.08) 15(26.32) 病程(年) 2.89±0.52 2.92±0.48 t=0.342 0.733 肿瘤大小(cm) 6.53±2.14 6.82±2.26 t=0.759 0.449 Child-Pugh分级[例(%)] χ2=0.863 0.353 A级 59(75.64) 39(68.42) B级 19(24.36) 18(31.58) BCLC分期[例(%)] χ2=0.318 0.573 B期 50(64.10) 32(56.14) C期 28(35.90) 25(43.86) 注:Child-Pugh分级,蔡尔德-皮尤分级;BCLC分期,巴塞罗那肝癌临床分期。
 下载: 导出CSV
下载: 导出CSV
表 2 两组患者治疗前后血清GP73、HIF-1α和MMP-9水平比较
Table 2. Comparison of serum GP73, HIF-1α and MMP-9 levels between the two groups before and after treatment
组别 例数 GP73(ng/mL) HIF-1α(ng/L) MMP-9(ng/mL) 治疗前 治疗后 治疗前 治疗后 治疗前 治疗后 缓解组 78 86.46±13.26 51.23±10.14 75.85±8.39 60.25±7.56 215.25±45.14 146.85±38.56 未缓解组 57 108.54±22.14 96.25±13.52 88.54±9.25 79.52±8.55 265.14±52.36 235.24±47.85 t值 7.218 22.114 8.311 13.837 5.926 11.874 P值 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 注:GP73,高尔基体蛋白73;HIF-1α,缺氧诱导因子-1α;MMP-9,基质金属蛋白酶-9。
下载: 导出CSV
表 3 影响TACE疗效的多因素分析
Table 3. Multiplicity analysis of factors influencing the efficacy of TACE
指标 β值 SE Wald P值 OR 95%CI GP73(ng/mL) 0.067 0.018 13.814 <0.001 1.069 1.032~1.107 HIF-1α(ng/L) 0.220 0.047 22.117 <0.001 1.246 1.137~1.365 MMP-9(ng/mL) 0.028 0.007 15.556 <0.001 1.028 1.014~1.042 注:GP73,高尔基体蛋白73;HIF-1α,缺氧诱导因子-1α;MMP-9,基质金属蛋白酶-9;TACE,经导管动脉化疗栓塞术;SE,标准误;OR,比值比;CI,置信区间。
下载: 导出CSV
表 4 治疗前血清GP73、HIF-1α和MMP-9水平对TACE疗效的预测价值分析
Table 4. Predictive value of serum GP73, HIF-1α, and MMP-9 levels before treatment for TACE efficacy
指标 AUC(95%CI) Z值 P值 约登指数 最佳临界值 敏感度(%) 特异度(%) GP73 0.799(0.722~0.863) 7.206 <0.001 0.547 100.93 ng/mL 64.91 89.74 HIF-1α 0.835(0.761~0.893) 9.778 <0.001 0.520 86.03 ng/L 59.65 95.31 MMP-9 0.777(0.697~0.844) 6.489 <0.001 0.534 261.29 ng/mL 64.91 88.46 联合检测 0.950(0.898~0.980) 27.775 <0.001 0.787 0.39 87.72 91.03 注:GP73,高尔基体蛋白73;HIF-1α,缺氧诱导因子-1α;MMP-9,基质金属蛋白酶-9;TACE,经导管动脉化疗栓塞术;AUC,曲线下面积;CI,置信区间。
下载: 导出CSV
-
[1] WANG CHM, ZHU JH, LIU XH, et al. Diagnostic value of combined detection of ascites and serum extracellular vesicle contents for HBV-related primary hepatocellular carcinoma[J]. Chin J Nosocomiology, 2025, 35( 19): 2921- 2926. DOI: 10.11816/cn.ni.2025-250428.王辰洪妹, 朱嘉恒, 刘晓会, 等. 腹水和血清细胞外囊泡内容物联合检测HBV相关原发性肝细胞癌的诊断价值[J]. 中华医院感染学杂志, 2025, 35( 19): 2921- 2926. DOI: 10.11816/cn.ni.2025-250428. [2] ZHANG YB. Observation on the changes and clinical significance study of serum T lymphocyte immunoglobulin mucin-3 and Golgi protein 73 in patients with hepatitis B virus infection related liver diseases[J]. Infection, Inflammation, Repair, 2024, 25( 2): 109- 113. DOI: 10.3969/j.issn.1672-8521.2024.02.006.张亚宾. 乙型肝炎病毒感染相关肝病患者血清T淋巴细胞免疫球蛋白黏蛋白分子-3、高尔基体蛋白73变化及其临床意义的研究[J]. 感染、炎症、修复, 2024, 25( 2): 109- 113. DOI: 10.3969/j.issn.1672-8521.2024.02.006. [3] Nursing Group of Interventional Medicine Branch of Hubei Medical Association, Interventional Perioperative Nursing Group of Interventional Physicians Branch of Chinese Medical Doctor Association. Expert consensus on perioperative nursing strategy of hepatocellular carcinoma treated by arterial chemoembolization[J]. J Clin Radiol, 2022, 41( 2): 212- 216.湖北省医学会介入医学分会护理学组, 中国医师协会介入医师分会介入围手术学组. 肝细胞癌经动脉化疗栓塞治疗围术期护理策略专家共识[J]. 临床放射学杂志, 2022, 41( 2): 212- 216. [4] YANG Y, LU P, LIN KY, et al. Analysis of factors influencing early recurrence for patients with initially unresectable hepatocellular carcinoma who underwent liver resection following downstaging treatment and construction of a predictive model: A multicenter study[J]. Chin J Dig Surg, 2025, 24( 2): 223- 235. DOI: 10.3760/cma.j.cn115610-20250106-00011.杨云, 卢鹏, 林孔英, 等. 初始不可切除肝细胞癌降期后行肝切除术患者早期复发影响因素分析及预测模型构建的多中心研究[J]. 中华消化外科杂志, 2025, 24( 2): 223- 235. DOI: 10.3760/cma.j.cn115610-20250106-00011. [5] WANG KQ, MAO JS, ZHAO Y, et al. Application progress of artificial intelligence in prognosis and therapeutic effect prediction of hepatocellular carcinoma by transcatheter arterial chemoembolization[J]. J Xiamen Univ Nat Sci, 2024, 63( 1): 13- 23. DOI: 10.6043/j.issn.0438-0479.202207014.王侃琦, 毛景松, 赵扬, 等. 人工智能在经导管动脉化疗栓塞术治疗肝细胞癌的预后和疗效预测中的应用进展[J]. 厦门大学学报(自然科学版), 2024, 63( 1): 13- 23. DOI: 10.6043/j.issn.0438-0479.202207014. [6] ZHU YJ, WANG MM, ZHAO SJ, et al. Determination of the earliest time point for efficacy evaluation of transarterial chemoembolization combined with lenvatinib in patients with unresectable hepatocellular carcinoma based on imaging evaluation methods[J]. Clin J Med Offic, 2024, 52( 11): 1123- 1128. DOI: 10.16680/j.1671-3826.2024.11.05.祝叶静, 汪檬檬, 赵首捷, 等. 基于影像学评价手段确定经肝动脉化疗栓塞术联合仑伐替尼治疗不可切除肝细胞癌患者疗效评估最早时间节点[J]. 临床军医杂志, 2024, 52( 11): 1123- 1128. DOI: 10.16680/j.1671-3826.2024.11.05. [7] TANG H, LIU W, CHEN GS. Value of HC-gp39 and GP73 in the diagnosis of primary liver cancer and prognosis of TACE[J]. China J Mod Med, 2020, 30( 10): 54- 58. DOI: 10.3969/j.issn.1005-8982.2020.10.011.唐辉, 刘伟, 陈根生. HC-gp39和GP73检测对原发性肝癌的诊断及TACE预后的评估价值[J]. 中国现代医学杂志, 2020, 30( 10): 54- 58. DOI: 10.3969/j.issn.1005-8982.2020.10.011. [8] MÉNDEZ-BLANCO C, FERNÁNDEZ-PALANCA P, FONDEVILA F, et al. Prognostic and clinicopathological significance of hypoxia-inducible factors 1α and 2α in hepatocellular carcinoma: A systematic review with meta-analysis[J]. Ther Adv Med Oncol, 2021, 13: 1758835920987071. DOI: 10.1177/1758835920987071. [9] PU J, QIN ZB, FANG Q, et al. Hypoxia-induced HIF1A activates DUSP18-mediated MAPK14 dephosphorylation to promote hepatocellular carcinoma cell migration and invasion[J]. Pathol Res Pract, 2022, 237: 153955. DOI: 10.1016/j.prp.2022.153955. [10] LIAO JS, SONG L, WANG JC, et al. Effects of osthole on proliferation, migration and invasion of human hepatocellular carcinoma cells and the expression of MMP-2 and MMP-9[J]. J Chin Med Mater, 2020, 43( 6): 1469- 1472. DOI: 10.13863/j.issn1001-4454.2020.06.035.廖健思, 宋雷, 王建超, 等. 蛇床子素对人肝癌细胞增殖、迁移和侵袭能力及MMP-2、MMP-9表达的影响[J]. 中药材, 2020, 43( 6): 1469- 1472. DOI: 10.13863/j.issn1001-4454.2020.06.035. [11] Expert Panel of Antiviral Therapy for Hepatocellular Carcinoma. Expert consensus on antiviral therapy to hepatitis B/C virus-related hepatocellular carcinoma[J]. Chin Clin Oncol, 2014, 19( 5): 452- 459.肝细胞癌抗病毒治疗专家组. HBV/HCV相关性肝细胞癌抗病毒治疗专家共识[J]. 临床肿瘤学杂志, 2014, 19( 5): 452- 459. [12] Clinical Guidelines Committee of Chinese Interventionalists College. Chinese clinical practice guidelines for transarterial chemoembolization of hepatocellular carcinoma[J]. Chin J Intern Med, 2021, 60( 7): 599- 614. DOI: 10.3760/cma.j.cn112137-20210425-00991.中国医师协会介入医师分会临床诊疗指南专委会. 中国肝细胞癌经动脉化疗栓塞(TACE)治疗临床实践指南(2021年版)[J]. 中华内科杂志, 2021, 60( 7): 599- 614. DOI: 10.3760/cma.j.cn112137-20210425-00991. [13] YANG XN, WU YL. RECIST-New guidelines to evaluate the response to treatment in solid tumors[J]. J Evid Based Med, 2004, 4( 2): 85- 90. DOI: 10.3969/j.issn.1671-5144.2004.02.012.杨学宁, 吴一龙. 实体瘤治疗疗效评价标准——RECIST[J]. 循证医学, 2004, 4( 2): 85- 90. DOI: 10.3969/j.issn.1671-5144.2004.02.012. [14] LAI QY, GAO Y, WANG JL, et al. Effect of ulinastatin on the treatment of hepatocellular carcinoma after hepatectomy and its impact on Th9 and IL-9 in peripheral blood[J]. Transl Med J, 2025, 14( 1): 219- 222. DOI: 10.3639/i.issn.2095-3097.2025.01.043.赖全友, 高远, 汪建林, 等. 乌司他丁辅助肝叶切除术治疗肝细胞癌的效果及对外周血Th9、IL-9的影响[J]. 转化医学杂志, 2025, 14( 1): 219- 222. DOI: 10.3639/i.issn.2095-3097.2025.01.043. [15] LI SM, LIU B, PENG SL, et al. Correlation between HBV DNA load,serum IL-2R, GP73, miR-21 and HBVM expression pattern, liver histopathological changes in patients with chronic hepatitis B[J]. J Clin Exp Med, 2024, 23( 10): 1017- 1021. DOI: 10.3969/j.issn.1671-4695.2024.10.003.李述美, 刘冰, 彭思璐, 等. 慢性乙型肝炎患者HBV DNA载量及血清IL-2R、GP73、miR-21与HBVM表达模式、肝组织病理学改变的相关性[J]. 临床和实验医学杂志, 2024, 23( 10): 1017- 1021. DOI: 10.3969/j.issn.1671-4695.2024.10.003. [16] LIU YN, YAO MJ, LU FM. Clinical application of serum Golgi protein 73 in patients with chronic liver disease[J]. Chin Hepatol, 2021, 26( 2): 103- 106. DOI: 10.3969/j.issn.1008-1704.2021.02.002.刘燕娜, 姚明解, 鲁凤民. 慢性肝病患者中血清高尔基体蛋白73的临床应用[J]. 肝脏, 2021, 26( 2): 103- 106. DOI: 10.3969/j.issn.1008-1704.2021.02.002. [17] HUYNH KN, RAO S, ROTH B, et al. Targeting hypoxia-inducible factor-1α for the management of hepatocellular carcinoma[J]. Cancers, 2023, 15( 10): 2738. DOI: 10.3390/cancers15102738. [18] LUO YW, FANG Y, ZENG HX, et al. HIF1α counteracts TGFβ1-driven TSP1 expression in endothelial cells to stimulate angiogenesis in the hypoxic tumor microenvironment[J]. Cancer Res, 2025, 85( 1): 69- 83. DOI: 10.1158/0008-5472.CAN-24-2324. [19] DING ZN, DONG ZR, CHEN ZQ, et al. Effects of hypoxia-inducible factor-1α and hypoxia-inducible factor-2α overexpression on hepatocellular carcinoma survival: A systematic review with meta-analysis[J]. J Gastroenterol Hepatol, 2021, 36( 6): 1487- 1496. DOI: 10.1111/jgh.15395. [20] WANG FF, ZHANG GF, WANG Q, et al. GP73, AFU and 25(OH)D3 in patients with HBV infection and primary liver cancer and their association with recurrence and metastasis after TACE[J]. Chin J Nosocomiology, 2023, 33( 11): 1660- 1664. DOI: 10.11816/cn.ni.2023-221946.王芳芳, 张国范, 王琪, 等. HBV感染原发性肝癌患者GP73和AFU与25(OH)D3及其与TACE术后复发转移的关系[J]. 中华医院感染学杂志, 2023, 33( 11): 1660- 1664. DOI: 10.11816/cn.ni.2023-221946. [21] CHEN H, CHEN J, YUAN HX, et al. Hypoxia-inducible factor-1α: A critical target for inhibiting the metastasis of hepatocellular carcinoma[J]. Oncol Lett, 2022, 24( 2): 284. DOI: 10.3892/ol.2022.13404. [22] LIN ZH, JIANG JR, MA XK, et al. Prognostic value of serum HIF-1α change following transarterial chemoembolization in hepatocellular carcinoma[J]. Clin Exp Med, 2021, 21( 1): 109- 120. DOI: 10.1007/s10238-020-00667-8. [23] SUN JY, CHEN XY, WANG L, et al. Hypoxia-inducible factor-1α mediates and regulates angiogenesis-related factors expression in hepatocellular carcinoma[J]. Chin J Hepatol, 2020, 28( 11): 942- 948. DOI: 10.3760/cma.j.cn501113-20200228-00074.孙建英, 陈禧钰, 王理, 等. 缺氧诱导因子-1α介导和调控肝癌相关血管生成因子的表达[J]. 中华肝脏病杂志, 2020, 28( 11): 942- 948. DOI: 10.3760/cma.j.cn501113-20200228-00074. [24] LI YF. Mechanism of HIF-1α regulating GP73 and promoting EMT to lead to poor prognosis of TACE in hepatocellular carcinoma[D]. Urumqi: Xinjiang Medical University, 2022.李一帆. HIF-1α调控GP73促进EMT导致肝细胞肝癌TACE预后不良的机制研究[D]. 乌鲁木齐: 新疆医科大学, 2022. [25] XU Y, NING GL, HU ZJ, et al. Relationship between the levels of serum GP73 and IL-18 and HBV infection in patients with hepatocellular carcinoma and influence on disease progression after TACE[J]. J Med Postgrad, 2021, 34( 11): 1188- 1193. DOI: 10.16571/j.cnki.1008-8199.2021.11.013.徐永, 宁国龙, 胡宗举, 等. HBV感染的肝细胞癌患者血清高尔基体蛋白73与IL-18水平及其对肝动脉化疗栓塞术的影响[J]. 医学研究生学报, 2021, 34( 11): 1188- 1193. DOI: 10.16571/j.cnki.1008-8199.2021.11.013. [26] MENG YB, CHENG BB, DU J, et al. Research progress of mechanism for hypoxia promoting the occurrence and development of hepatocellular carcinoma[J]. Chin J Gen Surg, 2020, 29( 1): 97- 103. DOI: 10.7659/j.issn.1005-6947.2020.01.012.孟永斌, 程彬彬, 杜娟, 等. 缺氧促进肝细胞癌发生发展机制的研究进展[J]. 中国普通外科杂志, 2020, 29( 1): 97- 103. DOI: 10.7659/j.issn.1005-6947.2020.01.012. [27] GAO WL, WEI C, GUO XY. Prediction of preoperative serum MMP- 9 level for survival after hepatectomy in patients with HBV- associated hepatocellular carcinoma[J]. J Southeast Univ Med Sci Ed, 2022, 41( 5): 652- 659. DOI: 10.3969/j.issn.1671-6264.2022.05.008.高武林, 韦超, 郭晓烨. 术前血清MMP-9水平对HBV相关肝细胞癌患者肝切除术后生存的预测作用[J]. 东南大学学报(医学版), 2022, 41( 5): 652- 659. DOI: 10.3969/j.issn.1671-6264.2022.05.008. [28] WANG L, PENG JL. Association of hypoxia-inducible factor 1α expression with susceptibility to hepatitis B virus-related hepatocellular carcinoma: A meta-analysis[J]. Int J Biol Markers, 2023, 38( 3-4): 149- 158. DOI: 10.1177/03936155231204391. [29] SONG SL, WANG SJ, LI HM, et al. Changes and significance of serum HIF-1α and VEGF levels in patients with hepatocellular carcinoma before and after transcatheter arterial chemoembolization[J]. Shandong Med J, 2024, 64( 1): 60- 63. DOI: 10.3969/j.issn.1002-266X.2024.01.014.宋淑莉, 王淑娇, 李红梅, 等. 肝细胞癌患者经导管动脉化疗栓塞术前后血清HIF-1α、VEGF水平变化及其意义[J]. 山东医药, 2024, 64( 1): 60- 63. DOI: 10.3969/j.issn.1002-266X.2024.01.014. -

 本文二维码
本文二维码
计量
- 文章访问数: 10
- HTML全文浏览量: 1
- PDF下载量: 1
- 被引次数: 0

