
 PDF下载 ( 2016 KB)
PDF下载 ( 2016 KB)

影像学定量参数联合血清肿瘤标志物对胰腺导管腺癌术后预后的评估价值
DOI: 10.12449/JCH260620
Value of quantitative imaging parameters combined with serum tumor markers in prognostic evaluation after pancreatic ductal adenocarcinoma surgery
-
摘要:
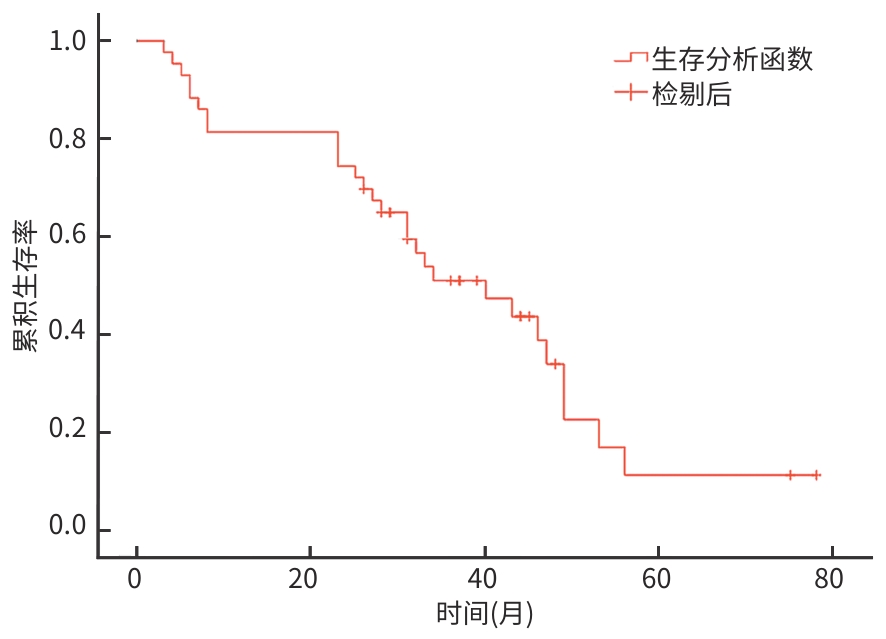
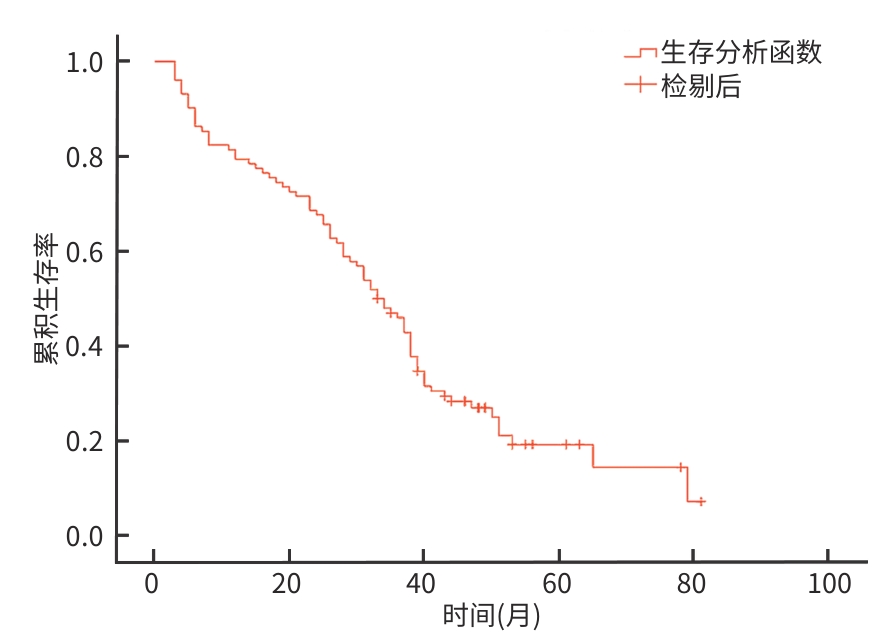
目的 探讨影像学定量参数联合血清肿瘤标志物构建的预测模型在胰腺导管腺癌(PDAC)患者术后预后评估中的应用价值。 方法 回顾性选取2020年4月—2023年3月于河北医科大学第四医院接受根治性切除术治疗的146例PDAC患者为研究对象,采用完全随机法将患者按照7∶3的比例分为训练集(n=102)和验证集(n=44)。所有患者进行增强计算机体层成像(CT)以及多参数磁共振成像扫描,记录动脉期、静脉期和延迟期CT值以及b值为800 s/mm2的表观扩散系数(ADC)、T2加权成像的信号强度(SI);检测患者血清糖类抗原19-9(CA19-9)及癌胚抗原(CEA)水平。计量资料两组间比较采用成组t检验;计数资料两组间比较采用χ2检验。Kaplan-Meier法绘制生存曲线,生存情况的比较采用Log-rank检验;采用单因素及多因素Logistic分析评估各临床及影像学指标与预后的关系,并采用最小绝对值收敛和选择算子(LASSO)-Cox回归模型筛选影响患者预后的重要因素,构建预后预测模型。采用受试者操作特征曲线分析该模型在训练集和验证集中的预后预测价值。 结果 Kaplan-Meier生存曲线分析显示,训练集患者的中位生存时间为33.00个月,验证集患者的中位生存时间为32.00个月,差异无统计学意义(P>0.05)。单因素分析结果显示,患者年龄、分化程度、淋巴结转移、肿瘤分期、血管侵犯、CA19-9、CEA、ADC及SI与患者生存预后有关(χ2值分别为5.906、13.116、12.807、17.277、14.611、7.275、14.339、9.506、13.137,P值均<0.05)。LASSO-Cox多因素回归分析显示,6个因素进入回归模型:肿瘤分期[风险比(HR)=8.934,95%CI:3.215~21.562,P<0.001]、淋巴结转移(HR=2.971,95%CI:1.298~5.647,P=0.002)、CA19-9(HR=3.948,95%CI:1.758~8.994,P<0.001)、CEA(HR=1.965,95%CI:1.083~3.664,P=0.039)、ADC(HR=2.873,95%CI:1.307~6.037,P=0.003)及SI(HR=3.107,95%CI:1.264~7.339,P=0.001)。基于上述指标构建的列线图模型在训练集中的预测曲线下面积为0.845[95%置信区间(CI):0.774~0.915],在验证集中的曲线下面积为0.919(95%CI:0.870~0.967)。 结论 基于LASSO-Cox回归构建的影像学定量参数-血清标志物联合模型可有效预测PDAC患者术后预后,有助于识别高风险患者,从而指导辅助治疗决策。 -
关键词:
- 胰腺肿瘤 /
- 体层摄影术, X线计算机 /
- 多参数磁共振成像 /
- 生物标记, 肿瘤 /
- 预后
Abstract:Objective To investigate the application value of a predictive model constructed based on quantitative imaging parameters and serum tumor markers in predicting the postoperative prognosis of patients with pancreatic ductal adenocarcinoma (PDAC). Methods A retrospective study was conducted among 146 patients with PDAC who underwent radical resection in Hebei Medical University Fourth Hospital from April 2020 to March 2023, and the patients were divided into a training set with 102 patients and a validation set of 44 patients at a ratio of 7∶3 using the completely randomized method. All patients underwent enhanced computed tomography (CT) and multi-parametric magnetic resonance imaging scans, and CT values in the arterial phase, the venous phase, and the delayed phase were recorded, as well as apparent diffusion coefficient (ADC) at b = 800 s/mm2 and signal intensity (SI) of T2 weighted imaging. The serum levels of carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen (CEA) were also measured. The independent-samples t test was used for comparison of continuous data between groups, and the chi-square test was used for comparison of categorical data between groups. Kaplan-Meier survival curves were plotted for survival analysis; the univariate and multivariate Logistic regression analysis was used to investigate the association of clinical and imaging indicators with prognosis; the least absolute shrinkage and selection operator (LASSO)-Cox regression model was used to identify the important influencing factors for prognosis, and a prognostic prediction model was constructed. The receiver operating characteristic (ROC) curve was used to analyze the predictive value of the model in predicting prognosis in both the training set and the validation set. Results The Kaplan-Meier survival curve analysis showed a median survival time of 33.00 months in the training set and 32.00 months in the validation set, with no significant difference between the training set and the validation set (P>0.05). The univariate analysis showed that patient age, degree of tumor differentiation, lymph node metastasis, tumor stage, vascular invasion, CA19-9, CEA, ADC value, and SI value were significantly associated with the survival prognosis of patients (χ²=5.906, 13.116, 12.807, 17.277, 14.611, 7.275, 14.339, 9.506, and 13.137, all P<0.05). The LASSO-Cox multivariate regression analysis showed that six factors were incorporated into the regression model, i.e., tumor stage (HR=8.934, 95%CI: 3.215 — 21.562, P<0.001), lymph node metastasis (HR=2.971, 95%CI: 1.298 — 5.647, P=0.002), CA19-9 (HR=3.948, 95%CI: 1.758 — 8.994, P<0.001), CEA (HR=1.965, 95%CI: 1.083 — 3.664, P=0.039), ADC value (HR=2.873, 95%CI: 1.307 — 6.037, P=0.003), and SI value (HR=3.107, 95%CI: 1.264 — 7.339, P=0.001). The nomogram model constructed based on these factors had an area under the ROC curve of 0.845 (95%CI: 0.774 — 0.915) in the training set and 0.919 (95%CI: 0.870 — 0.967) in the validation set. Conclusion The combined model of quantitative imaging parameters and serum tumor markers constructed based on LASSO-Cox regression can effectively predict the postoperative prognosis of PDAC patients, thereby helping to identify high-risk patients and guide decision-making for adjuvant therapy. -
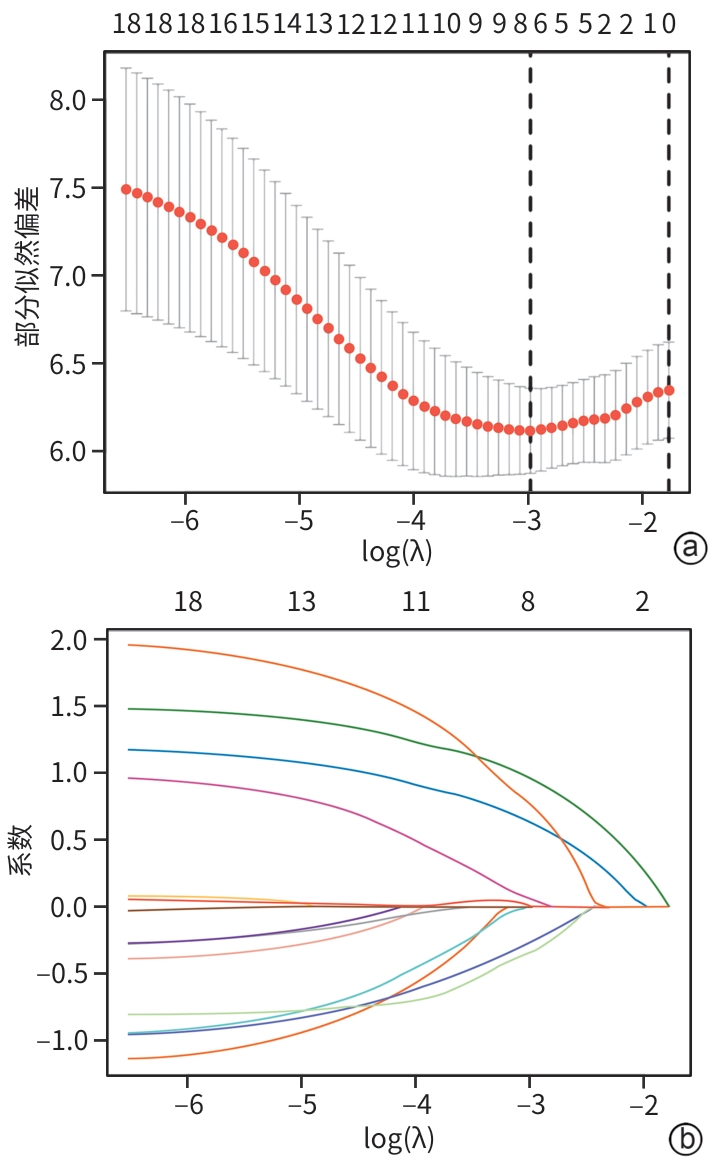
注: a,交叉验证曲线;b,系数路径图。
图 3 胰腺导管腺癌术后预后最小绝对值收敛和选择算子回归变量筛选
Figure 3. The minimum absolute contraction and selection operator regression variable screening for prognosis after pancreatic ductal carcinoma surgery
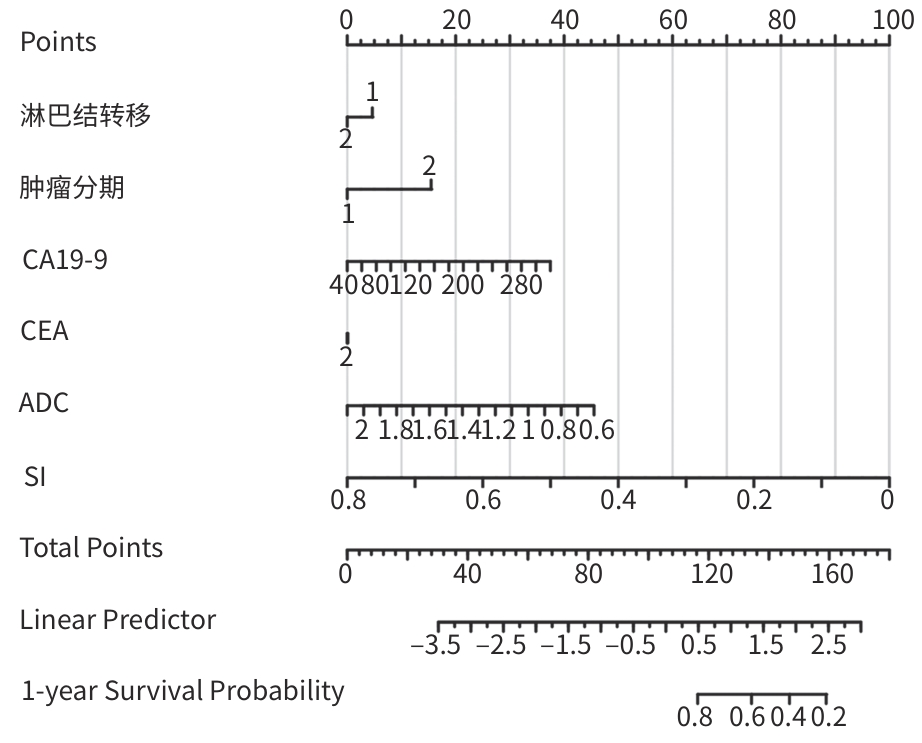
注: CA19-9,糖类抗原19-9;CEA,癌胚抗原;ADC,表观扩散系数;SI,信号强度。
图 4 胰腺导管腺癌术后预后预测列线图模型
Figure 4. Nomogram model for predicting prognosis after pancreatic ductal adenocarcinoma surgery
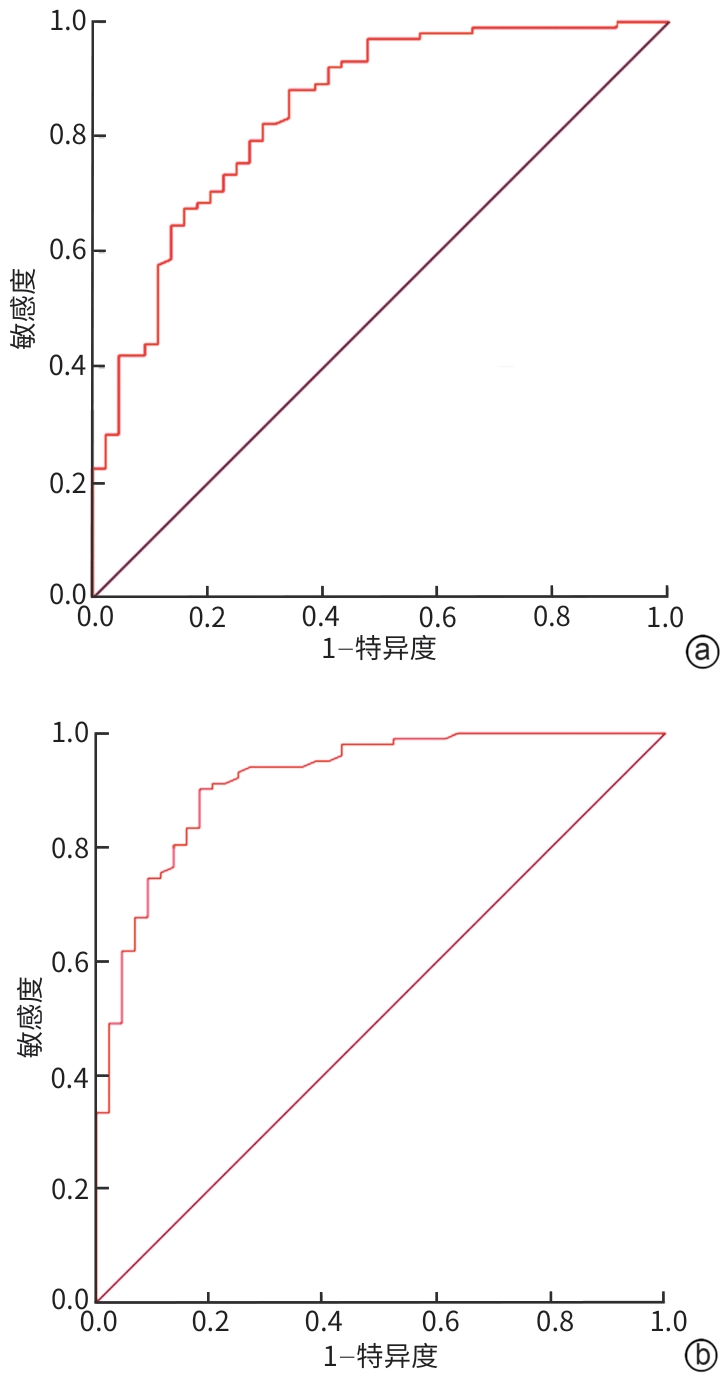
注: a,训练集;b,验证集。
图 5 模型对训练集和验证集患者预后预测价值的受试者操作特征曲线分析
Figure 5. ROC curve analysis of the model to evaluate its predictive value for the prognosis of patients in the training set and patients in the validation set
表 1 训练集及验证集患者临床资料比较
Table 1. Comparison of clinical data of patients in the training set and the validation set
临床资料 训练集(n=102) 验证集(n=44) 统计值 P值 性别[例(%)] χ2=0.186 0.666 男 48(47.06) 19(43.18) 女 54(52.94) 25(56.82) 年龄(岁) 55.23±8.64 54.58±6.59 t=0.446 0.656 高血压[例(%)] 25(24.51) 13(29.55) χ2=0.405 0.525 糖尿病[例(%)] 17(16.67) 6(13.64) χ2=0.213 0.645 分化程度[例(%)] χ2=0.251 0.617 中高分化 67(65.69) 27(61.36) 低分化 35(34.31) 17(38.64) 肿瘤最大径(cm) 3.57±1.21 3.74±1.30 t=0.762 0.448 肿瘤位置[例(%)] χ2=0.059 0.812 胰头颈部 67(65.69) 28(63.64) 胰体尾部 35(34.31) 16(36.36) 淋巴结转移[例(%)] 39(38.24) 15(34.09) χ2=0.227 0.634 肿瘤分期[例(%)] χ2=0.133 0.715 Ⅰ期 38(37.25) 15(34.09) Ⅱ~Ⅲ期 64(62.75) 29(65.91) 血管侵犯[例(%)] 41(40.20) 17(38.64) χ2=0.031 0.860 CA19-9(U/mL) 185.43±53.02 189.28±31.64 t=0.448 0.655 CEA(U/mL) 12.56±4.21 13.04±3.15 t=0.678 0.499 CT值(HU) 平扫期 34.83±3.19 36.04±3.95 t=1.953 0.053 动脉期 43.87±5.52 41.96±6.03 t=1.865 0.064 门静脉期 54.58±7.93 54.02±8.49 t=0.383 0.702 延迟期 60.21±5.68 59.38±6.10 t=0.792 0.430 ADC(×10-3 mm2/s) 1.21±0.31 1.27±0.28 t=1.104 0.272 SI(×10-3) 0.45±0.09 0.46±0.12 t=0.555 0.580 注:CA19-9,糖类抗原19-9;CEA,癌胚抗原;CT,计算机断层扫描;ADC,表观扩散系数;SI,信号强度。
 下载: 导出CSV
下载: 导出CSV
表 2 训练集患者生存预后单因素分析
Table 2. Univariate analysis of survival prognosis of patients in the training set
因素 例数 中位生存期(月) 95%CI χ2值 P值 性别 0.159 0.690 男 48 34.00 27.512~40.488 女 54 32.00 22.398~41.602 年龄 5.906 0.015 ≥55岁 53 28.00 22.650~33.350 <55岁 49 38.00 34.193~41.807 高血压 25 32.00 23.840~40.160 0.438 0.508 糖尿病 17 31.00 18.899~43.101 0.823 0.364 分化程度 13.116 <0.001 中高分化 67 38.00 35.669~40.331 低分化 35 23.00 14.443~31.557 肿瘤最大径 0.233 0.629 ≥3.5 cm 55 34.00 28.627~39.373 <3.5 cm 47 28.00 14.806~41.194 肿瘤位置 0.273 0.602 胰头颈部 67 34.00 28.092~39.908 胰体尾部 35 33.00 22.706~43.294 淋巴结转移 39 24.00 16.658~31.342 12.807 <0.001 肿瘤分期 17.277 <0.001 Ⅰ期 38 43.00 34.006~51.994 Ⅱ~Ⅲ期 64 28.00 23.569~32.431 血管侵犯 41 25.00 19.772~30.228 14.611 <0.001 CA19-9 7.275 0.007 ≥185 U/mL 56 26.00 19.714~32.286 <185 U/mL 46 39.00 33.412~44.588 CEA 14.339 0.001 ≥12 U/mL 54 24.00 17.827~30.173 <12 U/mL 48 40.00 37.408~42.592 平扫期CT值 1.170 0.279 ≥34 HU 59 32.00 23.577~40.423 <34 HU 43 35.00 29.493~40.507 动脉期CT值 0.830 0.362 ≥43 HU 61 36.00 30.265~41.735 <43 HU 41 29.00 20.934~37.066 门静脉期CT值 0.072 0.788 ≥54 HU 63 34.00 28.920~39.080 <54 HU 39 32.00 21.115~42.885 延迟期CT值 0.802 0.370 ≥60 HU 57 37.00 26.994~47.006 <60 HU 45 32.00 26.840~37.160 ADC 9.506 0.002 ≥1.2×10-3 mm2/s 60 38.00 35.501~40.499 <1.2×10-3 mm2/s 42 27.00 20.649~33.351 SI 13.137 0.001 ≥0.45×10-3 58 26.00 19.506~32.494 <0.45×10-3 44 39.00 35.856~42.144 注:CA19-9,糖类抗原19-9;CEA,癌胚抗原;CT,计算机体层成像;ADC,表观扩散系数;SI,信号强度;CI,置信区间。
下载: 导出CSV
表 3 胰腺导管腺癌术后预后Cox多因素回归分析
Table 3. Cox multivariate regression analysis of prognosis after pancreatic ductal adenocarcinoma surgery
因素 HR 95%CI P值 肿瘤分期 8.934 3.215~21.562 <0.001 淋巴结转移 2.971 1.298~5.647 0.002 CA19-9 3.948 1.758~8.994 <0.001 CEA 1.965 1.083~3.664 0.039 ADC 2.873 1.307~6.037 0.003 SI 3.107 1.264~7.339 0.001 注:CA19-9,糖类抗原19-9;CEA,癌胚抗原;ADC,表观扩散系数;SI,信号强度;HR,风险比;CI,置信区间。
下载: 导出CSV
-
[1] WANG T, YE L, LUO JG, et al. Expression and significance of miR-510 in pancreatic ductal adenocarcinoma[J]. China J Gen Surg, 2025, 34( 2): 390- 396. DOI: 10.7659/j.issn.1005-6947.240592.王涛, 叶林, 罗纪光, 等. miR-510在胰腺导管腺癌中的表达及意义[J]. 中国普通外科杂志, 2025, 34( 2): 390- 396. DOI: 10.7659/j.issn.1005-6947.240592. [2] GROSSBERG AJ, CHU LC, DEIG CR, et al. Multidisciplinary standards of care and recent progress in pancreatic ductal adenocarcinoma[J]. CA Cancer J Clin, 2020, 70( 5): 375- 403. DOI: 10.3322/caac.21626. [3] SCHIMA W, BÖHM G, RÖSCH CS, et al. Mass-forming pancreatitis versus pancreatic ductal adenocarcinoma: CT and MR imaging for differentiation[J]. Cancer Imaging, 2020, 20( 1): 52. DOI: 10.1186/s40644-020-00324-z. [4] LIU ZH, LONG D, WANG Q, et al. MicroRNA-324-5p targeting transmembrane and coiled-coil domain family 1 regulates the proliferation of pancreatic ductal adenocarcinoma cells[J]. Chin J Exp Surg, 2025, 42( 1): 29- 32. DOI: 10.3760/cma.j.cn421213-20240808-00023.刘宗昊, 龙迪, 王琦, 等. 微小RNA-324-5p靶向卷曲结构域家族1调控胰腺导管腺癌细胞增殖的实验研究[J]. 中华实验外科杂志, 2025, 42( 1): 29- 32. DOI: 10.3760/cma.j.cn421213-20240808-00023. [5] LU PY, ZHAI J, LI YC, et al. Prognostic value of preoperative quantitative CT analysis of body components in patients with radical resection of pancreatic ductal adenocarcinoma[J]. Radiol Pract, 2025, 40( 2): 243- 247. DOI: 10.13609/j.cnki.1000-0313.2025.02.016.鹿佩瑶, 翟建, 李云成, 等. 术前定量CT分析身体组分对根治性切除术胰腺导管腺癌患者预后的预测价值[J]. 放射学实践, 2025, 40( 2): 243- 247. DOI: 10.13609/j.cnki.1000-0313.2025.02.016. [6] LI RT, ZHAO HF, WANG XD, et al. Research progress of artificial intelligence and radiomics in preoperative prediction of lymph node metastasis in pancreatic ductal adenocarcinoma[J]. Chin J Magn Reson Imag, 2025, 16( 3): 211- 215. DOI: 10.12015/issn.1674-8034.2025.03.036.李锐彤, 赵海峰, 王晓东, 等. 人工智能及影像组学在术前预测胰腺导管腺癌淋巴结转移中的研究进展[J]. 磁共振成像, 2025, 16( 3): 211- 215. DOI: 10.12015/issn.1674-8034.2025.03.036. [7] TAO XF, XIANG H, PAN Y, et al. Pancreatitis initiated pancreatic ductal adenocarcinoma: Pathophysiology explaining clinical evidence[J]. Pharmacol Res, 2021, 168: 105595. DOI: 10.1016/j.phrs.2021.105595. [8] FAN WJ, DENG XQ, ZHENG LC, et al. Clinical value of ultrasound and contrast enhanced ultrasound in the differential diagnosis of pancreatic neuroendocrine tumors and pancreatic ductal adenocarcinoma[J]. J China Med Univ, 2025, 54( 4): 359- 363. DOI: 10.12007/j.issn.0258-4646.2025.04.013.樊维娟, 邓小倩, 郑立春, 等. 超声及超声造影在鉴别胰腺神经内分泌瘤与胰腺导管腺癌中的临床价值[J]. 中国医科大学学报, 2025, 54( 4): 359- 363. DOI: 10.12007/j.issn.0258-4646.2025.04.013. [9] XIE D, LIANG HW, ZHOU Y, et al. Value of dual-energy CT parameters in evaluating the pathological grade of pancreatic ductal adenocarcinoma[J]. Chin J Endocr Surg, 2025, 19( 2): 266- 270. DOI: 10.3760/cma.j.cn.115807-20231030-00126.谢丹, 梁洪伟, 周旸, 等. 双能量CT参数对胰腺导管腺癌病理分级的评估价值[J]. 中华内分泌外科杂志(中英文), 2025, 19( 2): 266- 270. DOI: 10.3760/cma.j.cn.115807-20231030-00126. [10] TONG T, GU JH, XU D, et al. Deep learning radiomics based on contrast-enhanced ultrasound images for assisted diagnosis of pancreatic ductal adenocarcinoma and chronic pancreatitis[J]. BMC Med, 2022, 20( 1): 74. DOI: 10.1186/s12916-022-02258-8. [11] PAPADAKOS SP, DEDES N, GKOLEMI N, et al. The EPH/ephrin system in pancreatic ductal adenocarcinoma(PDAC): From pathogenesis to treatment[J]. Int J Mol Sci, 2023, 24( 3): 3015. DOI: 10.3390/ijms24033015. [12] DU YS, GAO HY, LIU DX, et al. Predictive value of CT based radiomics model for the prognosis of patients with pancreatic ductal adenocarcinoma[J]. Chin J Dig Surg, 2025, 24( 8): 1067- 1074. DOI: 10.3760/cma.j.cn115610-20250801-00506.杜岳姗, 高华钰, 刘丁瑕, 等. CT检查影像组学模型对胰腺导管腺癌预后的预测价值[J]. 中华消化外科杂志, 2025, 24( 8): 1067- 1074. DOI: 10.3760/cma.j.cn115610-20250801-00506. [13] ZENG LL, LI SS, YUE PF, et al. The value of clinical characteristics and hematological parameters for prognostic assessment of pancreatic cancer patients undergoing radical resection[J]. J Sichuan Univ Med Sci, 2024, 55( 3): 708- 716. DOI: 10.12182/20240560604.曾莲丽, 李双双, 岳鹏飞, 等. 一般临床特征与血液学参数在胰腺导管腺癌根治性切除术患者中的预后价值研究[J]. 四川大学学报(医学版), 2024, 55( 3): 708- 716. DOI: 10.12182/20240560604. [14] ZHAO LH, HOU WJ, ZHAO J, et al. Application of qualitative and quantitative analysis of contrast-enhanced ultrasound in the differential diagnosis of pancreatic ductal adenocarcinoma and non-pancreatic ductal adenocarcinoma[J]. Chin J Ultrason, 2024, 33( 10): 855- 861. DOI: 10.3760/cma.j.cn131148-20240407-00214.赵利辉, 侯文静, 赵静, 等. 超声造影定性及定量分析在胰腺导管腺癌与非导管腺癌鉴别诊断中的应用价值[J]. 中华超声影像学杂志, 2024, 33( 10): 855- 861. DOI: 10.3760/cma.j.cn131148-20240407-00214. [15] WANG HZ, YANG X, CHEN XY, et al. The role of KRT6A in regulating the biological behavior of pancreatic ductal adenocarcinoma PANC1 cells and its role as a target for diagnosis and prognosis[J]. Chin J Cancer Biother, 2024, 31( 5): 462- 468. DOI: 10.3872/j.issn.1007-385x.2024.05.005.王浩泽, 杨轩, 陈昕苑, 等. KRT6A调控胰腺导管腺癌细胞生物学行为的作用及作为诊断与预后判断靶标的研究[J]. 中国肿瘤生物治疗杂志, 2024, 31( 5): 462- 468. DOI: 10.3872/j.issn.1007-385x.2024.05.005. [16] BARARIA A, DEY S, GULATI S, et al. Differential methylation landscape of pancreatic ductal adenocarcinoma and its precancerous lesions[J]. Hepatobiliary Pancreat Dis Int, 2020, 19( 3): 205- 217. DOI: 10.1016/j.hbpd.2020.03.010. [17] LIU S, XIE C, LIU YH. Value of a nomogram model in early recurrence of pancreatic ductal adenocarcinoma after laparoscopic pancreaticoduodenectomy[J]. J Clin Hepatol, 2024, 40( 1): 138- 146. DOI: 10.12449/JCH240123.刘舜, 谢诚, 刘亚辉. 胰腺导管腺癌行腹腔镜下胰十二指肠切除术后早期复发的列线图模型及其预测价值分析[J]. 临床肝胆病杂志, 2024, 40( 1): 138- 146. DOI: 10.12449/JCH240123. [18] XU YW, WANG YF, HÖTI N, et al. The next"sweet" spot for pancreatic ductal adenocarcinoma: Glycoprotein for early detection[J]. Mass Spectrom Rev, 2023, 42( 2): 822- 843. DOI: 10.1002/mas.21748. [19] LIN GH, CHEN WY, XU CR, et al. Application value of dual-energy CT multi-parameter imaging in predicting the pathological grade of pancreatic ductal adenocarcinoma[J]. Chin J Dig Surg, 2025, 24( 1): 127- 136. DOI: 10.3760/cma.j.cn115610-20241213-00554.林桂涵, 陈炜越, 许彩如, 等. 双能量CT检查多参数成像预测胰腺导管腺癌病理学分级的应用价值[J]. 中华消化外科杂志, 2025, 24( 1): 127- 136. DOI: 10.3760/cma.j.cn115610-20241213-00554. [20] WANG J, LIAO JX, QIU Y, et al. Construction of a prognostic model for pancreatic ductal adenocarcinoma based on m6A-and m5C-related lncRNAs and its relationship with the immune microenvironment[J]. China J Gen Surg, 2025, 34( 3): 475- 484. DOI: 10.7659/j.issn.1005-6947.240563.王婕, 廖俊熙, 邱熠, 等. 基于m6A和m5C相关lncRNA的胰腺导管腺癌预后模型及其与免疫微环境的关系[J]. 中国普通外科杂志, 2025, 34( 3): 475- 484. DOI: 10.7659/j.issn.1005-6947.240563. [21] DU JL, GU JC, LI J. Mechanisms of drug resistance of pancreatic ductal adenocarcinoma at different levels[J]. Biosci Rep, 2020, 40( 7): BSR20200401. DOI: 10.1042/BSR20200401. [22] CHEN G, SONG GX, HAN X, et al. Expression of Claudin18.2 in pancreatic ductal adenocarcinoma and its clinical pathological significance[J]. J Clin Pathol Res, 2024, 44( 10): 1352- 1358. DOI: 10.11817/j.issn.2095-6959.2024.240763.陈刚, 宋国新, 韩雪, 等. 胰腺导管腺癌中Claudin18.2的表达及其临床病理意义[J]. 临床与病理杂志, 2024, 44( 10): 1352- 1358. DOI: 10.11817/j.issn.2095-6959.2024.240763. [23] HASHIMOTO D, SATOI S, FUJII T, et al. Is surgical resection justified for pancreatic ductal adenocarcinoma with distant abdominal organ metastasis? A position paper by experts in pancreatic surgery at the Joint Meeting of the International Association of Pancreatology(IAP)& the Japan Pancreas Society(JPS) 2022 in Kyoto[J]. Pancreatology, 2023, 23( 6): 682- 688. DOI: 10.1016/j.pan.2023.07.005. [24] ZHANG R, TIAN CJ, ZHANG X. Diagnostic value of contrast-enhanced computed tomography for mass-forming pancreatitis and pancreatic ductal adenocarcinoma[J]. Chin J Surg Integr Tradit West Med, 2024, 30( 5): 711- 715. DOI: 10.3969/j.issn.1007-6948.2024.05.021.张蕊, 田春江, 张翔. 增强CT对肿块型胰腺炎与胰腺导管腺癌的诊断价值研究[J]. 中国中西医结合外科杂志, 2024, 30( 5): 711- 715. DOI: 10.3969/j.issn.1007-6948.2024.05.021. [25] KONG M, XIA HC, ZHU FL. Imaging differential diagnosis of autoimmune pancreatitis from pancreatic ductal adenocarcinoma[J]. J Pract Radiol, 2023, 39( 1): 75- 78. DOI: 10.3969/j.issn.1002-1671.2023.01.019.孔梅, 夏好成, 朱付立. 自身免疫性胰腺炎和胰腺导管腺癌影像学鉴别[J]. 实用放射学杂志, 2023, 39( 1): 75- 78. DOI: 10.3969/j.issn.1002-1671.2023.01.019. [26] SAKURAI Y, YOKOYAMA K, KANNO A, et al. Pancreatic ductal adenocarcinoma with autoimmune pancreatitis: A case report and literature review[J]. Intern Med, 2025, 64( 10): 1525- 1533. DOI: 10.2169/internalmedicine.4361-24. [27] ZHUANG Y, CHEN J, LI JY, et al. Value of multiparameter MRI radiomics model in predicting the pathological diferentiation of pancreatic ductal adenocarcinoma[J]. J Clin Radiol, 2023, 42( 11): 1768- 1773. DOI: 10.13437/j.cnki.jcr.2023.11.015.庄雨, 陈杰, 李静燕, 等. 多参数MRI影像组学模型预测胰腺导管腺癌病理分化程度的价值[J]. 临床放射学杂志, 2023, 42( 11): 1768- 1773. DOI: 10.13437/j.cnki.jcr.2023.11.015. -

 本文二维码
本文二维码
计量
- 文章访问数: 6
- HTML全文浏览量: 2
- PDF下载量: 1
- 被引次数: 0

