
 PDF下载 ( 851 KB)
PDF下载 ( 851 KB)

辅助肝移植: 提升供肝利用率的机遇与挑战
DOI: 10.12449/JCH260633
Auxiliary liver transplantation: Opportunities and challenges in improving donor liver utilization rate
-
摘要: 肝移植是终末期肝病的标准疗法,但长期受限于供肝短缺。临床实践中,三类供肝(多米诺供肝、小尺寸移植肝和脂肪变性供肝)因代谢缺陷、体积不足和质量欠佳等问题面临使用限制。本综述系统梳理了多米诺供肝、小尺寸移植肝和脂肪变性供肝的定义、应用现状及使用瓶颈,重点阐述辅助肝移植(保留受体部分或全部自体肝脏、叠加供肝功能支持的特殊术式)在规避小肝综合征、弥补代谢缺陷和拓展边缘肝应用等方面的独特价值与临床实践进展,旨在为优化终末期肝病肝移植策略、提升供肝利用率提供针对性的临床实践参考。Abstract: Liver transplantation is the standard treatment for end-stage liver disease, but it has long been limited by the shortage of donor livers. In clinical practice, three types of donor liver (domino donor livers, small-for-size grafts, and steatotic donor livers) are limited due to issues such as metabolic defects, insufficient volume, and poor quality. This article systematically reviews the definition, clinical application, and bottlenecks of the above three types of donor livers and elaborates on the unique value and clinical practice advances of auxiliary liver transplantation (a special surgical procedure that retains part or all of the recipient’s own liver and superimposes donor liver function support) in avoiding small-for-size syndrome, compensating for metabolic defects, and expanding the application of marginal livers, in order to provide a targeted clinical practice reference for optimizing liver transplantation strategies for end-stage liver disease and improving donor liver utilization rate.
-
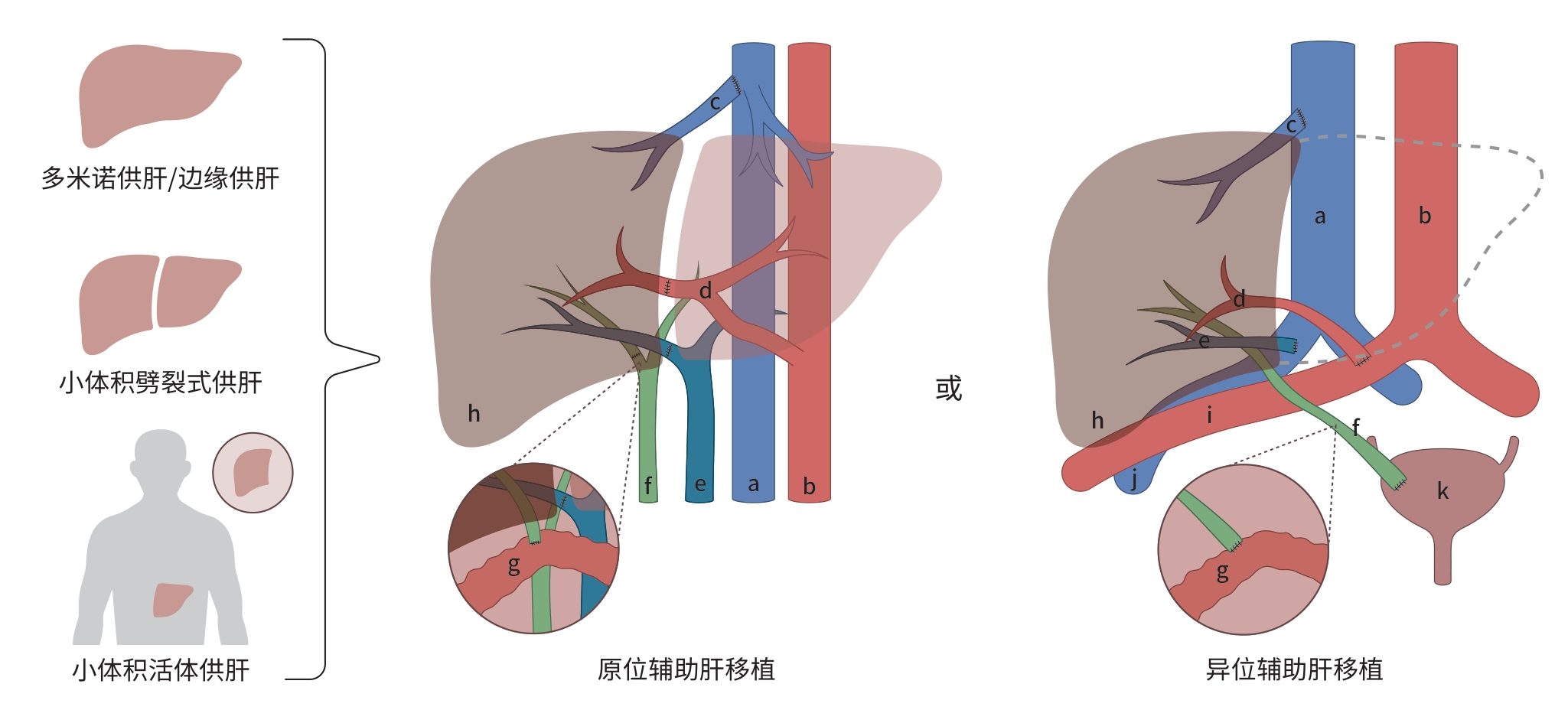
注: a,下腔静脉;b,腹主动脉;c,肝静脉;d,肝动脉;e,门静脉;f,胆管;g,肠管;h,肝脏;i,髂动脉;j,髂静脉;k,膀胱。
图 1 辅助肝移植示意图
Figure 1. Schematic diagram auxiliary liver transplantation
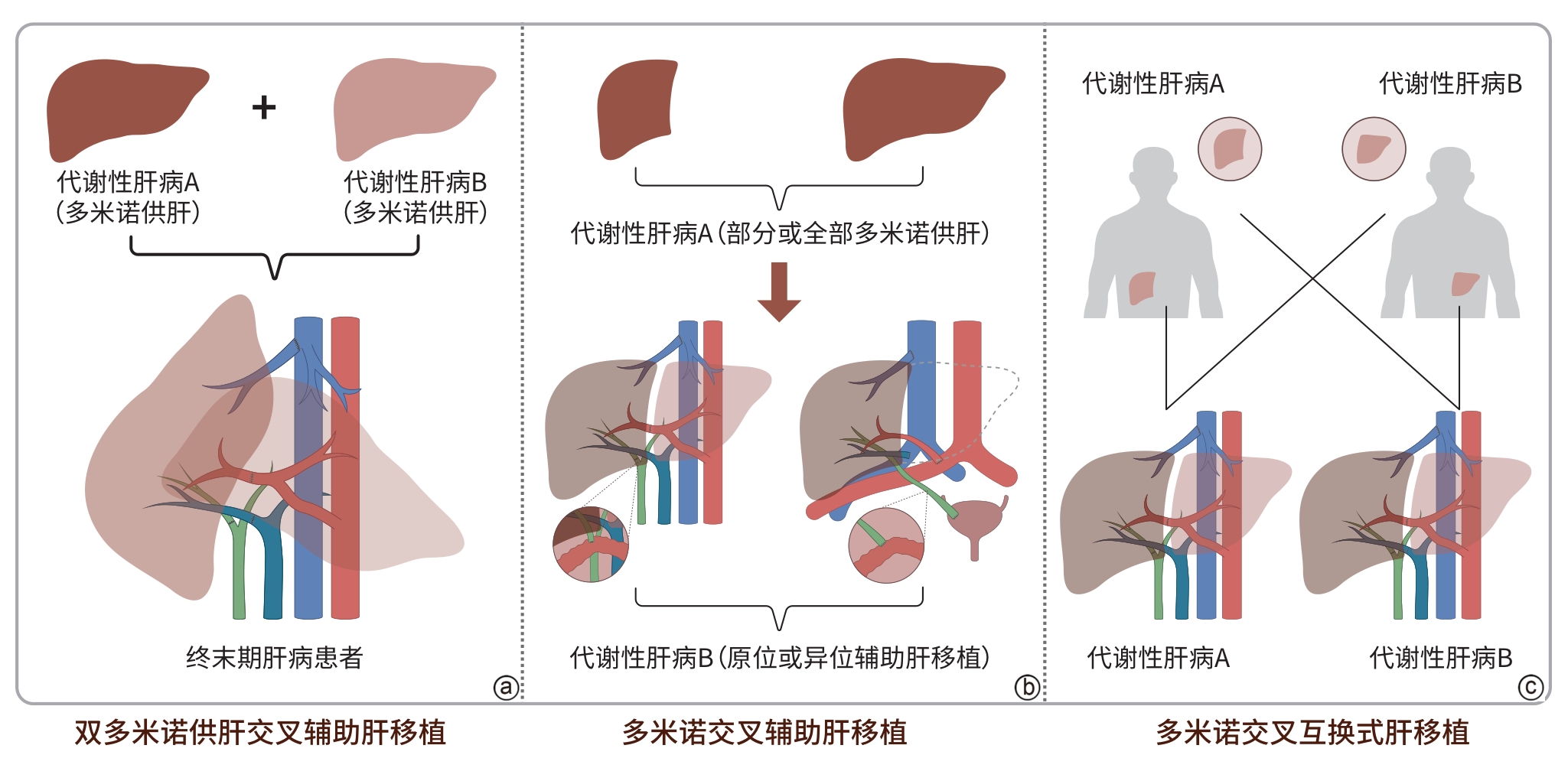
图 2 多米诺供肝交叉辅助式肝移植示意图
Figure 2. Schematic diagram cross-auxiliary domino liver transplantation
表 1 辅助肝移植与传统肝移植对比
Table 1. Comparison of adjuvant liver transplantation with conventional liver transplantation
项目 辅助肝移植 传统肝移植 适应证 急性/亚急性肝衰竭、高脱落风险者、NCIMLD患者、接
受小体积供肝者终末期肝硬化、急/慢加急性肝衰竭、米兰标准的恶性肿瘤、
自身免疫性/代谢性肝病体积要求 可采用GRWR<0.8%的小体积活体供肝、GRWR≤1.0%
的脑/心死亡劈裂供肝GRWR>0.8%或GV/SLV>40% 脂肪变性 可耐受大泡性脂肪变性>30% 大泡性脂肪变性<30% 供肝类型 多米诺供肝、小体积劈裂式/活体供肝、边缘供肝/弃肝 脑/心死亡供肝、足量体积劈裂/活体供肝、部分多米诺供肝 优势 保留自体肝,肝功能叠加;
供肝要求低,利用率高;
可停用免疫抑制剂肝脏置换彻底,长期疗效稳定;
技术成熟,术程标准化;
普及度高,为肝移植主流术式不足 技术复杂、仅少数中心开展;
依赖个体化方案,无统一标准;
长期预后存残肝相关风险;
部分需Ⅱ期切除残肝;
并发症及远期预后证据不足供肝短缺;
供肝要求严、利用率低;
终生服用免疫抑制剂;
受体等待期间脱落/死亡风险高注:NCIMLD,非硬化性遗传代谢性肝脏疾病;GRWR,移植物与受体重量比;GV/SLV,移植肝体积与标准肝体积比。
 下载: 导出CSV
下载: 导出CSV
-
[1] TREFTS E, GANNON M, WASSERMAN DH. The liver[J]. Curr Biol, 2017, 27( 21): R1147- R1151. DOI: 10.1016/j.cub.2017.09.019. [2] LUCEY MR, FURUYA KN, FOLEY DP. Liver transplantation[J]. N Engl J Med, 2023, 389( 20): 1888- 1900. DOI: 10.1056/nejmra2200923. [3] China Organ Transplantation Development Foundation. China Organ Donation and Transplantation Development Report(2024)[M]. Beijing: Tsinghua University Press, 2025: 26- 36.中国器官移植发展基金会. 中国器官捐献和移植发展报告(2024)[M]. 北京: 清华大学出版社, 2025: 26- 36. [4] Branch of Organ Transplant of China Medical Association. Clinical application guidelines for domino liver transplantation(2024 editon)[J]. Chin J Dig Surg, 2024, 23( 11): 1389- 1398. DOI: 10.3760/cma.j.cn115610-20241023-00463.中华医学会器官移植学分会. 多米诺肝移植临床应用指南(2024版)[J]. 中华消化外科杂志, 2024, 23( 11): 1389- 1398. DOI: 10.3760/cma.j.cn115610-20241023-00463. [5] TAO KS, YANG ZX, ZHANG X, et al. Gene-modified pig-to-human liver xenotransplantation[J]. Nature, 2025, 641( 8064): 1029- 1036. DOI: 10.1038/s41586-025-08799-1. [6] XIANG Z, LI JR, ZENG HX, et al. Current understanding of marginal grafts in liver transplantation[J]. Aging Dis, 2024, 16( 2): 1036- 1058. DOI: 10.14336/AD.2024.0214. [7] Branch of Organ Transplant of China Medical Association. Clinical application guidelines for auxiliary liver transplantation(2024 edition)[J]. Chin J Dig Surg, 2024, 23( 11): 1373- 1388. DOI: 10.3760/cma.j.cn115610-20241023-00462.中华医学会器官移植学分会. 辅助肝移植临床应用指南(2024版)[J]. 中华消化外科杂志, 2024, 23( 11): 1373- 1388. DOI: 10.3760/cma.j.cn115610-20241023-00462. [8] PRAVISANI R, COCCHI L, CESARETTI M, et al. Refining auxiliary orthotopic liver transplantation(AOLT) improves outcomes in adult patients with acute liver failure[J]. Ann Surg, 2023, 278( 5): 790- 797. DOI: 10.1097/SLA.0000000000006019. [9] Liver Transplantation Group, Branch of Organ Transplantation of Chinese Medical Association; Branch of Organ Transplant Physicians of Chinese Medical Doctor Association. Chinese clinical practice guidelines for extended criteria donor grafts in liver transplantation[J/OL]. Chin J Transpl(Electronic Edition), 2025, 19( 2): 65- 75. DOI: 10.3877/cma.j.issn.1674-3903.2025.02.001.中华医学会器官移植学分会肝移植学组, 中国医师协会器官移植医师分会. 中国扩大标准供肝移植临床应用指南(2025版)[J/OL]. 中华移植杂志(电子版), 2025, 19( 2): 65- 75. DOI: 10.3877/cma.j.issn.1674-3903.2025.02.001. [10] QUADROS J, PIEDADE C, LOPES MF. Auxiliary liver transplantation for management of acute liver failure in children-Systematic review[J]. Transplant Rev, 2021, 35( 4): 100631. DOI: 10.1016/j.trre.2021.100631. [11] KASAHARA M, HONG JC, DHAWAN A. Evaluation of living donors for hereditary liver disease(siblings, heterozygotes)[J]. J Hepatol, 2023, 78( 6): 1147- 1156. DOI: 10.1016/j.jhep.2022.10.013. [12] ZHOU GP, SUN LY, ZHU ZJ. The concept of“domino” in liver and hepatocyte transplantation[J]. Therap Adv Gastroenterol, 2020, 13: 1756284820968755. DOI: 10.1177/1756284820968755. [13] MARQUES HP, BARROS I, LI J, et al. Current update in domino liver transplantation[J]. Int J Surg, 2020, 82: 163- 168. DOI: 10.1016/j.ijsu.2020.03.017. [14] ADAMS D, KOIKE H, SLAMA M, et al. Hereditary transthyretin amyloidosis: A model of medical progress for a fatal disease[J]. Nat Rev Neurol, 2019, 15( 7): 387- 404. DOI: 10.1038/s41582-019-0210-4. [15] DEON M, GUERREIRO G, GIRARDI J, et al. Treatment of maple syrup urine disease: Benefits, risks, and challenges of liver transplantation[J]. Int J Dev Neurosci, 2023, 83( 6): 489- 504. DOI: 10.1002/jdn.10283. [16] EWING CB, SOLTYS KA, STRAUSS KA, et al. Metabolic control and“ideal” outcomes in liver transplantation for maple syrup urine disease[J]. J Pediatr, 2021, 237: 59- 64.e1. DOI: 10.1016/j.jpeds.2021.06.028. [17] STRAUSS KA, MAZARIEGOS GV, SINDHI R, et al. Elective liver transplantation for the treatment of classical maple syrup urine disease[J]. Am J Transplant, 2006, 6( 3): 557- 564. DOI: 10.1111/j.1600-6143.2005.01209.x. [18] BARSHOP BA, KHANNA A. Domino hepatic transplantation in maple syrup urine disease[J]. N Engl J Med, 2005, 353( 22): 2410- 2411. DOI: 10.1056/NEJM200512013532220. [19] CELIK N, KELLY B, SOLTYS K, et al. Technique and outcome of domino liver transplantation from patients with maple syrup urine disease: Expanding the donor pool for live donor liver transplantation[J]. Clin Transplant, 2019, 33( 11): e13721. DOI: 10.1111/ctr.13721. [20] ABIFADEL M, BOILEAU C. Genetic and molecular architecture of familial hypercholesterolemia[J]. J Intern Med, 2023, 293( 2): 144- 165. DOI: 10.1111/joim.13577. [21] THOMPSON GR, WALJI S, CEGLA J. Liver transplantation for homozygous familial hypercholesterolaemia[J]. Curr Opin Lipidol, 2025, 36( 6): 310- 317. DOI: 10.1097/MOL.0000000000001007. [22] GOLBUS JR, FARHAT L, FONTANA RJ, et al. Rapidly progressive atherosclerosis after domino liver transplantation from a teenage donor with homozygous familial hypercholesterolemia[J]. J Clin Lipidol, 2017, 11( 5): 1284- 1288. DOI: 10.1016/j.jacl.2017.07.006. [23] QU W, ZHU ZJ, WEI L, et al. Feasibility of domino liver transplantation from hyperhomocsyteinemia[J]. Clin Res Hepatol Gastroenterol, 2019, 43( 5): 527- 532. DOI: 10.1016/j.clinre.2019.01.010. [24] KHANNA A, GISH R, WINTER SC, et al. Successful domino liver transplantation from a patient with methylmalonic acidemia[M]. Berlin, Heidelberg: Springer, 2015: 87- 94. DOI: 10.1007/8904_2015_480. [25] MOGUILEVITCH M, DELPHIN E. Domino liver transplantation from a child with propionic acidemia to a child with idiopathic fulminant hepatic failure[J]. Case Rep Transplant, 2018, 2018: 1897495. DOI: 10.1155/2018/1897495. [26] VOLLMAR J, SCHMID JC, HOPPE-LOTICHIUS M, et al. Progression of transthyretin(TTR) amyloidosis in donors and recipients after domino liver transplantation-a prospective single-center cohort study[J]. Transpl Int, 2018, 31( 11): 1207- 1215. DOI: 10.1111/tri.13326. [27] DIXIT N, CASTANO A, FARR MJ, et al. Rapidly progressive transthyretin-mediated amyloidosis in a domino liver transplant recipient of a Ser23Asn donor[J]. J Clin Neuromuscul Dis, 2016, 17( 3): 142- 145. DOI: 10.1097/CND.0000000000000110. [28] ZHU ZJ, WEI L, QU W, et al. First case of cross-auxiliary double domino donor liver transplantation[J]. World J Gastroenterol, 2017, 23( 44): 7939- 7944. DOI: 10.3748/wjg.v23.i44.7939. [29] HUANG YF, ZHU ZJ.“No-donor” liver transplantation[J]. Hepatobiliary Pancreat Dis Int, 2025, 24( 1): 23- 28. DOI: 10.1016/j.hbpd.2024.10.006. [30] FUKAZAWA K, NISHIDA S. Size mismatch in liver transplantation[J]. J Hepatobiliary Pancreat Sci, 2016, 23( 8): 457- 466. DOI: 10.1002/jhbp.371. [31] MASUDA Y, YOSHIZAWA K, OHNO Y, et al. Small-for-size syndrome in liver transplantation: Definition, pathophysiology and management[J]. Hepatobiliary Pancreat Dis Int, 2020, 19( 4): 334- 341. DOI: 10.1016/j.hbpd.2020.06.015. [32] LAW JH, KOW AW. Prediction and management of small-for-size syndrome in living donor liver transplantation[J]. Clin Mol Hepatol, 2025, 31( Suppl): S301- S326. DOI: 10.3350/cmh.2024.0870. [33] OGURA Y, HORI T, MOGHAZY WM EL, et al. Portal pressure<15 mm Hg is a key for successful adult living donor liver transplantation utilizing smaller grafts than before[J]. Liver Transpl, 2010, 16( 6): 718- 728. DOI: 10.1002/lt.22059. [34] IKEGAMI T, YOSHIZUMI T, SAKATA K, et al. Left lobe living donor liver transplantation in adults: What is the safety limit?[J]. Liver Transpl, 2016, 22( 12): 1666- 1675. DOI: 10.1002/lt.24611. [35] UEMURA T, WADA S, KAIDO T, et al. How far can we lower graft-to-recipient weight ratio for living donor liver transplantation under modulation of portal venous pressure?[J]. Surgery, 2016, 159( 6): 1623- 1630. DOI: 10.1016/j.surg.2016.01.009. [36] KOW AWC, LIU J, PATEL MS, et al. Post living donor liver transplantation small-for-size syndrome: Definitions, timelines, biochemical, and clinical factors for diagnosis: Guidelines from the ILTS-iLDLT-LTSI consensus conference[J]. Transplantation, 2023, 107( 10): 2226- 2237. DOI: 10.1097/TP.0000000000004770. [37] HAKEEM AR, MATHEW JS, AUNÉS CV, et al. Preventing small-for-size syndrome in living donor liver transplantation: Guidelines from the ILTS-iLDLT-LTSI consensus conference[J]. Transplantation, 2023, 107( 10): 2203- 2215. DOI: 10.1097/TP.0000000000004769. [38] MAIWALL R, KULKARNI AV, ARAB JP, et al. Acute liver failure[J]. Lancet, 2024, 404( 10454): 789- 802. DOI: 10.1016/S0140-6736(24)00693-7. [39] LIM C, TURCO C, BALCI D, et al. Auxiliary liver transplantation for cirrhosis: From APOLT to RAPID: A scoping review[J]. Ann Surg, 2022, 275( 3): 551- 559. DOI: 10.1097/SLA.0000000000005336. [40] ZHANG QZ, LIU ST, ZHANG LH, et al. Value of body roundness index in predicting the risk of metabolic dysfunction-associated fatty liver disease[J]. J Clin Hepatol, 2025, 41( 10): 2054- 2061. DOI: 10.12449/JCH251015.张琪振, 刘素彤, 张丽慧, 等. 体圆指数对代谢相关脂肪性肝病发生风险的预测价值[J]. 临床肝胆病杂志, 2025, 41( 10): 2054- 2061. DOI: 10.12449/JCH251015. [41] GEDALLOVICH SM, LADNER DP, VANWAGNER LB. Liver transplantation in the era of non-alcoholic fatty liver disease/metabolic(dysfunction) associated fatty liver disease: The dilemma of the steatotic liver graft on transplantation and recipient survival[J]. Hepatobiliary Surg Nutr, 2022, 11( 3): 425- 429. DOI: 10.21037/hbsn-22-9. [42] CHANG YC, YEN KC, LIANG PC, et al. Automated liver volumetry and hepatic steatosis quantification with magnetic resonance imaging proton density fat fraction[J]. J Formos Med Assoc, 2025, 124( 3): 264- 270. DOI: 10.1016/j.jfma.2024.04.012. [43] NORTHUP PG, INTAGLIATA NM, DAVIS JPE, et al. Macrosteatotic allografts and obese recipients have nearly equal negative impact on liver transplant survival[J]. Transplantation, 2020, 104( 6): 1193- 1200. DOI: 10.1097/TP.0000000000002990. [44] KIM DS, YOON YI, KIM BK, et al. Asian Pacific Association for the Study of the Liver clinical practice guidelines on liver transplantation[J]. Hepatol Int, 2024, 18( 2): 299- 383. DOI: 10.1007/s12072-023-10629-3. [45] ORCI LA, BERNEY T, MAJNO PE, et al. Donor characteristics and risk of hepatocellular carcinoma recurrence after liver transplantation[J]. Br J Surg, 2015, 102( 10): 1250- 1257. DOI: 10.1002/bjs.9868. [46] BACCARANI U, ADANI GL, ISOLA M, et al. Steatosis of the graft is a risk factor for posttransplantation biliary complications[J]. Transplant Proc, 2009, 41( 4): 1313- 1315. DOI: 10.1016/j.transproceed.2009.03.084. [47] KONG DC, ZHANG XJ, YUN YG, et al. Risk factors for biliary stricture and prognosis after orthotopic liver transplantation[J]. J Clin Hepatol, 2024, 40( 11): 2253- 2259. DOI: 10.12449/JCH241119.孔德财, 张小静, 员阳光, 等. 原位肝移植术后胆道狭窄的危险因素及预后分析[J]. 临床肝胆病杂志, 2024, 40( 11): 2253- 2259. DOI: 10.12449/JCH241119. [48] ZHANG HY, JIANG J, HU ZQ. Mechanisms and repair strategies of ischemia-reperfusion injury in steatotic donor livers[J]. Organ Transpl, 2025, 16( 4): 620- 625. DOI: 10.12464/j.issn.1674-7445.2025093.张黄燕, 江杰, 胡宗强. 脂肪变性供肝缺血-再灌注损伤的发生机制及修复策略[J]. 器官移植, 2025, 16( 4): 620- 625. DOI: 10.12464/j.issn.1674-7445.2025093. [49] DUAN WD, WANG XT, WANG HG, et al. Auxiliary partial liver transplantation for acute liver failure using“high risk” grafts: Case report[J]. World J Gastroenterol, 2016, 22( 5): 1919- 1924. DOI: 10.3748/wjg.v22.i5.1919. [50] WANG Z, HUANG XW, SHI YH, et al. Auxiliary liver transplantation using otherwise-discarded liver allograft combined with associating liver partition and portal vein ligation for staged hepatectomy for unresectable colorectal liver metastases[J]. Hepatobiliary Surg Nutr, 2025, 14( 4): 683- 688. DOI: 10.21037/hbsn-2025-392. -

 本文二维码
本文二维码
计量
- 文章访问数: 8
- HTML全文浏览量: 0
- PDF下载量: 2
- 被引次数: 0

