
 PDF下载 ( 2262 KB)
PDF下载 ( 2262 KB)

常见临床指标及无创肝纤维化评分对中国肝病型Wilson病进展期肝纤维化的诊断价值
DOI: 10.3969/j.issn.1001-5256.2021.03.014
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突,特此声明。
作者贡献声明:梁晨负责资料查阅、写作;刘晖、郑素军负责写作框架设计;梁晨、刘晖、白洁、王泰龄参与数据收集、分析;任艳、刘念晨、白丽负责数据分析;刘霜、陈煜、段钟平、郑素军负责审核结果。
Value of common clinical indices and noninvasive liver fibrosis scores in the diagnosis of advanced liver fibrosis in hepatic-type Wilson's disease in China
-
摘要:
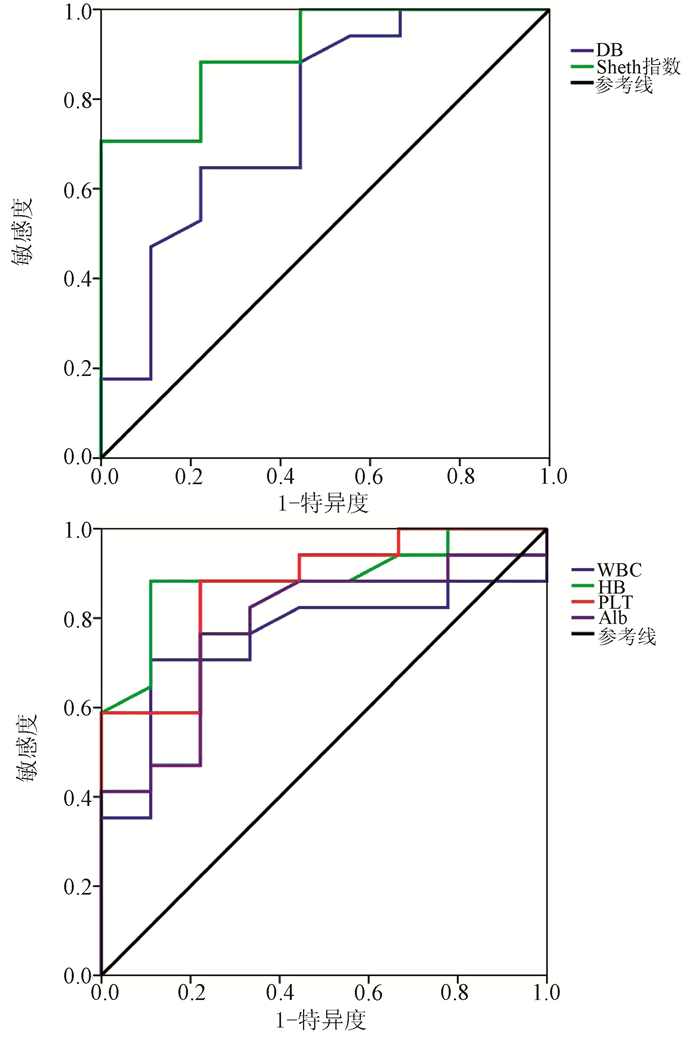
目的 探讨常见临床指标及无创肝纤维化评分与中国肝病型Wilson病(WD)的关系,及其对进展期肝纤维化的鉴别能力。 方法 回顾性收集1996年5月—2020年4月于北京佑安医院及中日友好医院诊治的236例中国WD患者临床资料,纳入有肝脏病理且临床资料齐全的肝病型WD患者26例,应用METAVIR评分判断肝纤维化分期,将患者分为进展期肝纤维化(F3期、F4期)和非进展期肝纤维化(F0期、F1期、F2期)两组,计算3种无创肝纤维化评分(Sheth指数、APRI指数、FIB-4指数),比较两组间上述指数、相关临床指标差异。计量资料两组间比较采用独立样本t检验或Mann-Whitney U秩和检验;计数资料两组间比较采用Fisher检验。应用Spearman秩相关对有差异的指标进一步分析,筛选出与肝纤维化程度相关的临床指标及评分标准,绘制受试者工作特征曲线(ROC曲线)并计算曲线下面积(AUC)。 结果 本研究患者多在儿童及青少年时期发病,其中有10例(38.5%)患者K-F环为阳性,17例(65%)患者处于进展期肝纤维化阶段。进展期和非进展期肝纤维化患者比较,WBC(Z=-2.102,P=0.036)、Hb(t=-2.860,P=0.009)、PLT(t=-4.053,P<0.001)、DBil(Z=-2.130,P=0.033)、Alb(t=-2.875,P=0.008)、Sheth指数(Z=-3.369,P=0.001)差异均有统计学意义。WBC、Hb、PLT、Alb水平与WD患者肝纤维化程度呈负相关(r值分别为-0.587、-0.610、-0.656、-0.411,P值均<0.05),DBil和Sheth指数与肝纤维化程度呈正相关(r值分别为0.486、0.711,P值均<0.05)。ROC曲线分析显示,WBC、DBil、Sheth指数、Hb、PLT、Alb的AUC均>0.7,其中Sheth指数的AUC最大,为0.908,其敏感度和特异度分别为70.6%和100.0%,阳性和阴性预测值分别为100.0%和64.3%。 结论 Sheth指数的诊断效能优于其余单一临床指标,对中国肝病型WD进展期肝纤维化有较好的鉴别能力。 Abstract:Objective To investigate the association of common clinical indices and noninvasive liver fibrosis scores with hepatic-type Wilson's disease (WD) in Chinese patients and their ability to identify advanced liver fibrosis. Methods A retrospective analysis was performed for the clinical data of 236 Chinese patients with WD who were diagnosed and treated in Beijing YouAn Hospital and China-Japan Friendship Hospital from May 1996 to April 2020. A total of 26 patients with hepatic-type WD who underwent liver pathological examination and had complete clinical data were enrolled; the METAVIR score was used to determine liver fibrosis stage, and the patients were divided into advanced liver fibrosis (F3 and F4 stages) group and non-advanced liver fibrosis (F0, F1, and F2 stages) groups. Three noninvasive liver fibrosis scores [Sheth index, aspartate aminotransferase-to-platelet ratio index (APRI), and fibrosis-4 (FIB-4) index] were calculated for both groups, and the above indices and related clinical indices were compared between the two groups. The independent samples t-test or the Mann-Whitney U test was used for comparison of continuous data between two groups, and the Fisher's exact test was used for comparison of categorical data between two groups. The Spearman rank correlation test was used for further analysis of indices with statistical significance, and the clinical indices and scoring criteria correlated with liver fibrosis degree were screened out; the receiver operating characteristic (ROC) curve was plotted, and the area under the ROC curve (AUC) was calculated. Results Most of the patients in this study developed the disease in childhood and adolescence, and among these patients, 10 (38.5%) had positive K-F ring and 17 (65%) were in the stage of advanced liver fibrosis. There were significant differences between the advanced liver fibrosis group and the non-advanced liver fibrosis group in white blood cell count (WBC) (Z=-2.102, P=0.036), hemoglobin (Hb) (t=-2.860, P=0.009), platelet count (PLT) (t=-4.053, P < 0.001), direct bilirubin (DBil) (Z=-2.130, P=0.033), albumin (Alb) (t=-2.875, P=0.008), and Sheth index (Z=-3.369, P=0.001). WBC, Hb, PLT, and Alb were negatively correlated with liver fibrosis degree in WD patients (r=-0.587, -0.610, -0.656, and -0.411, all P < 0.05), and DBil and Sheth index were positively correlated with liver fibrosis degree (r=0.486 and 0.711, both P < 0.05). The ROC curve analysis showed that WBC, DBil, Sheth index, Hb, PLT, and Alb had an AUC of > 0.7, among which Sheth index had the largest AUC of 0.908, with a sensitivity of 70.6%, a specificity of 100.0%, a positive predictive value of 100.0%, and a negative predictive value of 64.3%. Conclusion Sheth index has a better diagnostic efficiency than the other clinical indices alone and can well identify advanced liver fibrosis in Chinese patients with hepatic-type WD. -
Key words:
- Liver Cirrhosis /
- Hepatolenticular Degeneration /
- Diagnosis /
- China
-
表 1 两组临床指标及无创肝纤维化评分比较
变量 全部患者 (n=26) 进展期纤维化组 (n=17) 非进展期纤维化组 (n=9) 统计值 P值 男/女(例) 14/12 8/9 6/3 0.429 K-F环(有/无或未知,例) 10/16 7/10 3/6 1.000 发病时年龄(岁) 19.77±14.37 20.18±16.34 19.00±10.52 t=0.195 0.847 WBC(×109/L) 4.62(3.94~5.69) 4.14(3.68~5.32) 5.58(4.74~6.31) Z=-2.102 0.036 Hb(g/L) 135.85±49.94 117.88±26.57 169.78±66.35 t=-2.860 0.009 PLT(×109/L) 157.24±93.75 114.60±61.44 237.78±93.55 t=-4.053 <0.001 ALT(U/L) 57.30(25.00~197.13) 52.60(23.00~150.00) 191.30(30.65~227.25) Z=-1.617 0.106 AST(U/L) 68.00(24.40~108.80) 46.30(24.10~125.10) 71.80(25.30~103.30) Z=-0.081 0.936 TBil(μmol/L) 16.05(10.18~25.78) 17.00(12.55~35.40) 9.70(7.55~23.85) Z=-1.913 0.056 DBil(μmol/L) 5.45(2.50~9.75) 7.20(3.85~10.40) 2.50(1.20~6.30) Z=-2.130 0.033 Alb(g/L) 38.30±6.28 36.34±6.61 42.01±3.45 t=-2.875 0.008 GGT(U/L) 74.95(36.38~136.00) 82.00(41.30~139.00) 73.30(27.60~155.55) Z=-0.296 0.767 ALP(U/L) 162.20(66.75~332.13) 193.90(68.00~333.75) 130.50(65.55~311.25) Z=-0.189 0.850 Sheth指数 0.89(0.55~1.22) 0.98(0.80~1.59) 0.51(0.45~0.75) Z=-3.369 0.001 FIB-4指数 3.92(0.80~5.56) 2.62(0.82~4.84) 5.66(0.73~13.88) Z=-1.644 0.100 APRI指数 0.98(0.59~2.28) 1.72(0.69~3.31) 0.79(0.55~0.98) Z=-1.913 0.056  下载: 导出CSV
下载: 导出CSV
表 2 WD患者临床指标、无创肝纤维化评分与肝纤维化程度的相关性
变量 95%CI r值 P值 WBC(×109/L) 3.36~9.04 -0.587 0.002 Hb(g/L) 115.67~156.02 -0.610 0.001 PLT(×109/L) 119.37~195.10 -0.656 <0.001 DBil(μmol/L) 4.66~10.54 0.486 0.012 Alb(g/L) 35.77~40.84 -0.411 0.037 Sheth指数 0.70~1.43 0.711 <0.001
下载: 导出CSV
表 3 Sheth指数及相关临床指标对WD进展期肝纤维化的诊断效能结果
变量 AUC P值 预测临界值 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) WBC 0.755 0.036 4.615×109/L 70.6 88.9 92.3 61.5 DBil 0.758 0.033 2.800 μmol/L 88.2 55.6 78.9 71.4 Sheth指数 0.908 0.001 0.905 70.6 100.0 100.0 64.3 Hb 0.889 0.001 137.500 g/L 88.2 88.9 93.7 80.0 PLT 0.869 0.002 172.500×109/L 88.2 77.8 88.2 77.8 Alb 0.781 0.020 41.350 g/L 76.5 77.8 86.7 63.6
下载: 导出CSV
-
[1] CZŁONKOWSKA A, LITWIN T, DUSEK P, et al. Wilson disease[J]. Nat Rev Dis Primers, 2018, 4(1): 21. DOI: 10.1038/s41572-018-0018-3 [2] GITLIN JD. Wilson disease[J]. Gastroenterology, 2003, 125(6): 1868-1877. DOI: 10.1053/j.gastro.2003.05.010 [3] ZHONG HJ, SUN HH, XUE LF, et al. Differential hepatic features presenting in Wilson disease-associated cirrhosis and hepatitis B-associated cirrhosis[J]. World J Gastroenterol, 2019, 25(3): 378-387. DOI: 10.3748/wjg.v25.i3.378 [4] MERLE U, SCHAEFER M, FERENCI P, et al. Clinical presentation, diagnosis and long-term outcome of Wilson's disease: A cohort study[J]. Gut, 2007, 56(1): 115-120. DOI: 10.1136/gut.2005.087262 [5] BRUHA R, MARECEK Z, POSPISILOVA L, et al. Long-term follow-up of Wilson disease: Natural history, treatment, mutations analysis and phenotypic correlation[J]. Liver Int, 2011, 31(1): 83-91. DOI: 10.1111/j.1478-3231.2010.02354.x [6] ROCKEY DC, CALDWELL SH, GOODMAN ZD, et al. Liver biopsy[J]. Hepatology, 2009, 49(3): 1017-1044. DOI: 10.1002/hep.22742 [7] SIDDIQUI MS, YAMADA G, VUPPALANCHI R, et al. Diagnostic accuracy of noninvasive fibrosis models to detect change in fibrosis stage[J]. Clin Gastroenterol Hepatol, 2019, 17(9): 1877-1885. DOI: 10.1016/j.cgh.2018.12.031 [8] MARELLA HK, REDDY YK, JIANG Y, et al. Accuracy of noninvasive fibrosis scoring systems in African American and white patients with nonalcoholic fatty liver disease[J]. Clin Transl Gastroenterol, 2020, 11(4): e00165. DOI: 10.14309/ctg.0000000000000165 [9] SCHMOYER CJ, KUMAR D, GUPTA G, et al. Diagnostic accuracy of noninvasive tests to detect advanced hepatic fibrosis in patients with hepatitis C and end-stage renal disease[J]. Clin Gastroenterol Hepatol, 2020, 18(10): 2332-2339. DOI: 10.1016/j.cgh.2020.02.019 [10] PATERNOSTRO R, PFEIFFENBERGER J, FERENCI P, et al. Non-invasive diagnosis of cirrhosis and long-term disease monitoring by transient elastography in patients with Wilson disease[J]. Liver Int, 2020, 40(4): 894-904. DOI: 10.1111/liv.14368 [11] SINI M, SORBELLO O, CIVOLANI A, et al. Non-invasive assessment of hepatic fibrosis in a series of patients with Wilson's Disease[J]. Dig Liver Dis, 2012, 44(6): 487-491. DOI: 10.1016/j.dld.2011.12.010 [12] European Association for Study of Liver. EASL clinical practice guidelines: Wilson's disease[J]. J Hepatol, 2012, 56(3): 671-685. DOI: 10.1016/j.jhep.2011.11.007 [13] BEDOSSA P, POYNARD T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group[J]. Hepatology, 1996, 24(2): 289-293. DOI: 10.1002/hep.510240201 [14] FERENCI P, STREMMEL W, CZŁONKOWSKA A, et al. Age and sex but not ATP7B genotype effectively influence the clinical phenotype of Wilson disease[J]. Hepatology, 2019, 69(4): 1464-1476. DOI: 10.1002/hep.30280 [15] SOKOL RJ, TWEDT D, MCKIM JM Jr, et al. Oxidant injury to hepatic mitochondria in patients with Wilson's disease and Bedlington terriers with copper toxicosis[J]. Gastroenterology, 1994, 107(6): 1788-1798. DOI: 10.1016/0016-5085(94)90822-2 [16] CROSAS-MOLIST E, FABREGAT I. Role of NADPH oxidases in the redox biology of liver fibrosis[J]. Redox Biol, 2015, 6: 106-111. DOI: 10.1016/j.redox.2015.07.005 [17] ZISCHKA H, LICHTMANNEGGER J. Pathological mitochondrial copper overload in livers of Wilson's disease patients and related animal models[J]. Ann N Y Acad Sci, 2014, 1315: 6-15. DOI: 10.1111/nyas.12347 -

 本文二维码
本文二维码
图(1) / 表(3)
计量
- 文章访问数: 588
- HTML全文浏览量: 301
- PDF下载量: 66
- 被引次数: 0

