
 PDF下载 ( 2074 KB)
PDF下载 ( 2074 KB)

经内镜逆行胰胆管造影术后StapferⅠ型十二指肠穿孔4例临床分析
DOI: 10.3969/j.issn.1001-5256.2021.06.037
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:张勇、汤善宏负责课题设计,资料分析,撰写论文;翁敏、何胜、黄怡、陈虹彬参与收集分析数据,修改论文;张勇负责拟定写作思路,指导撰写文章并最后定稿。
Stapfer type I duodenal perforation after endoscopic retrograde cholangiopancreatography: A clinical analysis of 4 cases
-
-
关键词:
- 胰胆管造影术, 内窥镜逆行 /
- 肠穿孔 /
- 治疗学
-
表 1 4例患者临床资料
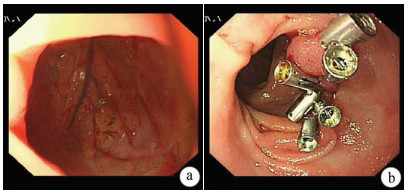
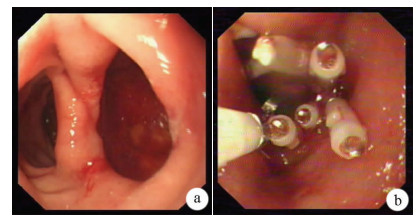
项目 病例1 病例2 病例3 病例4 性别 男 女 女 男 年龄(岁) 42 73 75 68 诊断 胆总管结石 缩窄性乳头炎 胰腺肿瘤、梗阻性黄疸、胆囊切除术后 胆囊肿瘤、梗阻性黄疸、胃穿孔修补术后 ERCP操作 EST取石+ENBD EST+ENBD 进镜时穿孔 进镜时穿孔 穿孔位置 乳头下方2.0 cm 乳头下方2.0 cm 球降交界 球降交界 穿孔大小 0.5 cm 1.2 cm 1.2 cm 1.0 cm 穿孔发现时间 ERCP术后2 h ERCP术中 ERCP术中 ERCP术中 处理方式 外科手术 8枚金属夹 6枚金属夹 8枚金属夹+尼龙绳 症状及体征 腹胀腹痛明显,腹肌紧,压痛反跳痛 腹胀,轻度腹痛,上腹轻度压痛、反跳痛 腹胀,轻度腹痛,上腹无压痛及无反跳痛 腹胀,轻度腹痛,上腹压痛,无反跳痛 住院时间(d) 14 20 16 15 操作者完成ERCP例数 100 200 300 350 预后 痊愈 痊愈 痊愈 痊愈  下载: 导出CSV
下载: 导出CSV
-
[1] ERCP group, Chinese Society of Digestive Endoscopology; Biliopancreatic group, Chinese Association ofGastroenterologist and hepatologist, National Clinical Research Center for Digestive Diseases. Chinese Guidelines for ERCP(2018)[J]. J Clin Hepatol, 2018, 34(12): 2537-2554. DOI: 10.3969/j.issn.1001-5256.2018.12.009.中华医学会消化内镜学分会ERCP学组, 中国医师协会消化医师分会胆胰学组, 国家消化系统疾病临床医学研究中心. 中国经内镜逆行胰胆管造影术指南(2018版)[J]. 临床肝胆病杂志, 2018, 34(12): 2537-2554. DOI: 10.3969/j.issn.1001-5256.2018.12.009. [2] STAPFER M, SELBY RR, STAIN SC, et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy[J]. Ann Surg, 2000, 232(2): 191-198. DOI: 10.1097/00000658-200008000-00007. [3] SRIVASTAVA S, SHARMA BC, PURI AS, et al. Impact of completion of primary biliary procedure on outcome of endoscopic retrograde cholangiopancreatographic related perforation[J]. Endosc Int Open, 2017, 5(8): e706-e709. DOI: 10.1055/s-0043-105494. [4] WEISER R, PENCOVICH N, MLYNARSKY L, et al. Management of endoscopicretrograde cholangiopancreatography-related perforations: Experience of a tertiary center[J]. Surgery, 2017, 161(4): 920-929. DOI: 10.1016/j.surg.2016.10.029. [5] WANG C, XU F, DAI CL. Value ofendoscopic ultrasonography combined with magnetic resonance cholangiopancreatography in diagnosis of patients suspected of common bile duct stones[J]. J Clin Hepatol, 2019, 35(1): 127-130. DOI: 10.3969/j.issn.1001-5256.2019.01.024.王超, 徐锋, 戴朝六. 超声内镜联合磁共振胰胆管造影对可疑胆总管结石的诊断价值[J]. 临床肝胆病杂志, 2019, 35(1): 127-130. DOI: 10.3969/j.issn.1001-5256.2019.01.024. [6] JIN YJ, JEONG S, KIM JH, et al. Clinical course and proposed treatment strategy for ERCP-related duodenal perforation: A multicenter analysis[J]. Endoscopy, 2013, 45(10): 806-812. DOI: 10.1055/s-0033-1344230. [7] DOǦANÜB, KESKIN MB, SÖKER G, et al. Endoscopic closure of an endoscope-related duodenal perforation using the over-the-scope clip[J]. Turk J Gastroenterol, 2013, 24(5): 436-440. DOI: 10.4318/tjg.2013.0594. [8] KNUDSON K, RAEBURN CD, MCINTYRE RC Jr, et al. Management of duodenal and pancreaticobiliary perforations associated with periampullary endoscopic procedures[J]. Am J Surg, 2008, 196(6): 975-981; discussion 981-982. DOI: 10.1016/j.amjsurg.2008.07.045. -


 本文二维码
本文二维码
图(3) / 表(1)
计量
- 文章访问数: 536
- HTML全文浏览量: 232
- PDF下载量: 49
- 被引次数: 0

