
 PDF下载 ( 5357 KB)
PDF下载 ( 5357 KB)

瞬时弹性成像技术对自身免疫性肝病肝纤维化分期诊断价值的Meta分析
DOI: 10.3969/j.issn.1001-5256.2022.01.015
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:杨志然、陈润花负责研究的思路或设计;王林恒、王雨负责研究数据的获取分析;杨志然、刘福生、王建芳和李园负责起草或修改文章关键内容。
Diagnostic value of transient elastography in the staging of hepatic fibrosis in patients with autoimmune liver disease: A Meta-analysis
-
摘要:
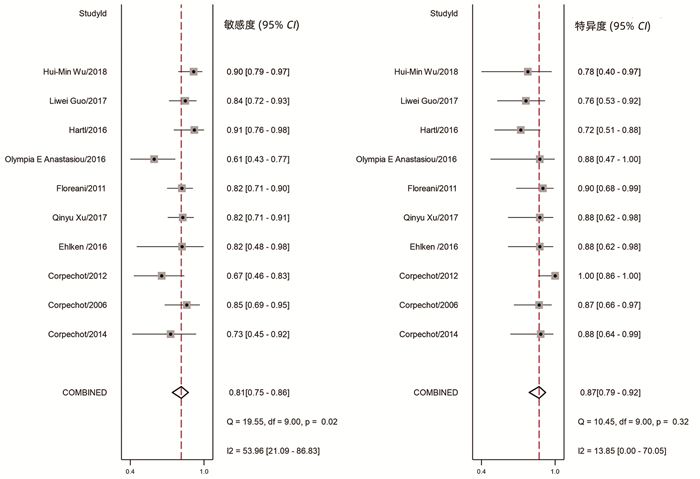
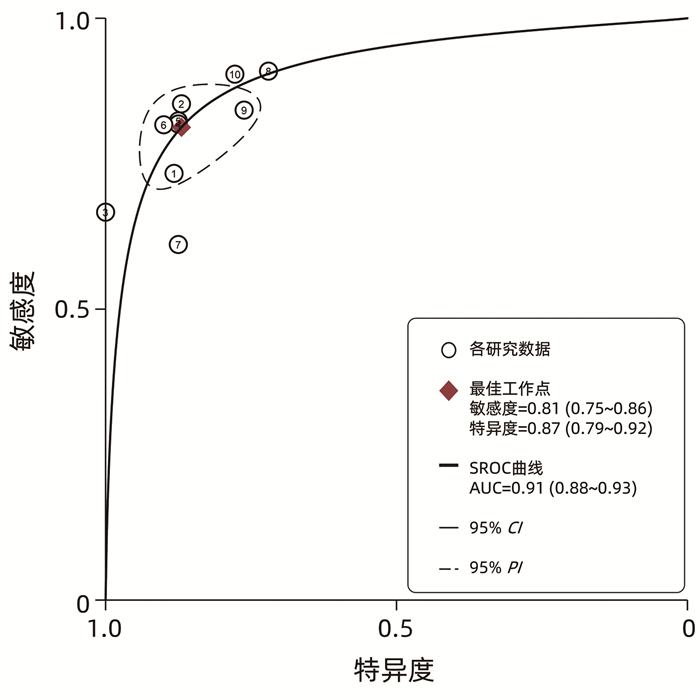
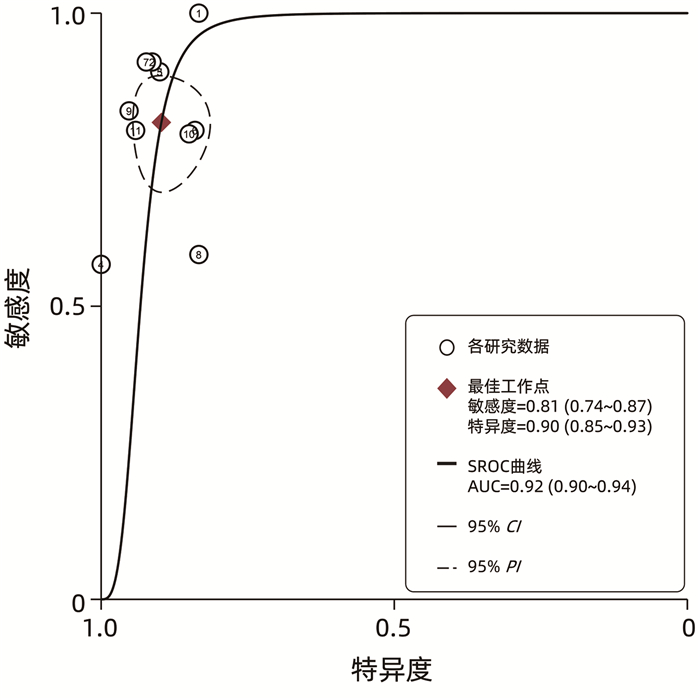
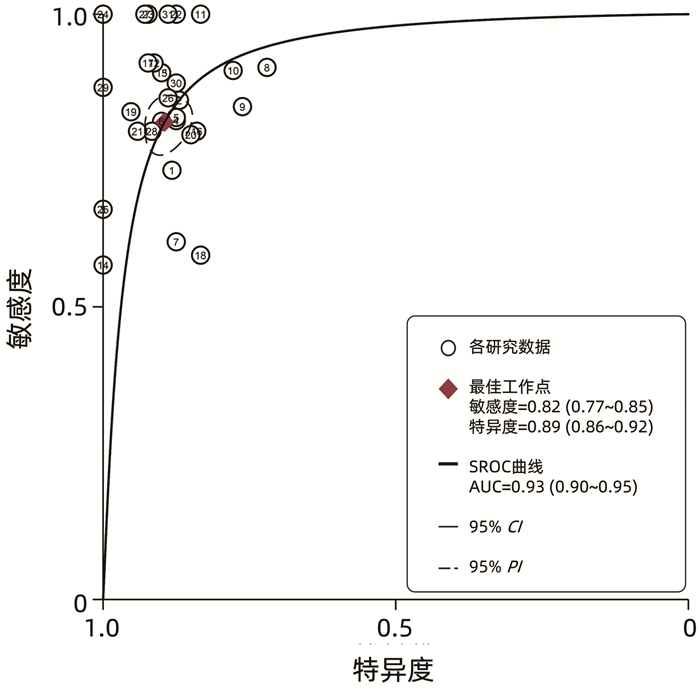
目的 系统评价瞬时弹性成像技术(TE)对自身免疫性肝病肝纤维化分期的诊断价值。 方法 系统检索PubMed、Embase、Cochrane Library、中国知网、万方、维普数据库中已发表的关于TE诊断自身免疫性肝病肝纤维化分期的中、英文文献,检索时限为2000年1月—2021年1月,由2位评价员对纳入文献进行数据提取,采用文献质量评价工具QUADAS2进行文献质量评价,并应用Stata 15.0软件中双变量混合效应模型进行Meta分析。 结果 纳入11篇文献,共1041例患者。TE诊断显著肝纤维化(≥F2)的合并敏感度、特异度和AUC分别为0.81(95%CI: 0.75~0.86)、0.87(95%CI: 0.79~ 0.92)和0.91(95%CI: 0.88~0.93),诊断进展期肝纤维化(≥F3)的合并敏感度、特异度和AUC分别为0.81(95%CI 0.74~0.87)、0.90(95%CI0.85~0.93)和0.92(95%CI0.90~0.94),诊断早期肝硬化(F4)的合并敏感度、特异度和AUC分别为0.87(95%CI: 0.74~0.93)、0.93(95%CI: 0.87~0.97)和0.96(95%CI: 0.94~0.97)。 结论 TE对于评估自身免疫性肝病显著肝纤维化、进展期肝纤维化以及早期肝硬化均具有较好的诊断价值,尤其是对早期肝硬化的诊断准确度较高。 -
关键词:
- 肝硬化 /
- 自身免疫疾病 /
- 弹性成像技术 /
- Meta分析(主题)
Abstract:Objective To investigate the value of transient elastography (TE) in the staging of hepatic fibrosis in patients with autoimmune liver disease (ALD). Methods PubMed, Embase, the Cochrane Library, CNKI, Wanfang Data, and VIP databases were searched for English and Chinese articles on TE in the staging of hepatic fibrosis in ALD published from January 2000 to January 2021. Two reviewers independently performed data extraction for the articles included, and QUADAS2 was used for quality assessment. The bivariate mixed effects model in Stata 15.0 software was used to perform the Meta-analysis. Results A total of 11 articles were included, with 1041 patients in total. In the diagnosis of significant hepatic fibrosis (F≥2), TE had a pooled sensitivity of 0.81 (95% CI: 0.75-0.86), a specificity of 0.87(95%CI 0.79-0.92), and an area under the receiver operating characteristic curve (AUC) of 0.91(95%CI 0.88-0.93); in the diagnosis of advanced hepatic fibrosis (F≥3), TE had a pooled sensitivity of 0.81(95%CI 0.74-0.87), a sensitivity of 0.90(95%CI 0.85-0.93), and an AUC of 0.92(95%CI 0.90-0.94); in the diagnosis of early-stage liver cirrhosis (F4), TE had a pooled sensitivity of 0.87(95%CI 0.74-0.93), a specificity of 0.93(95%CI 0.87-0.97), and an AUC of 0.96(95%CI 0.94-0.97). Conclusion TE has a good diagnostic value in evaluating significant liver fibrosis, advanced liver fibrosis, and early-stage liver cirrhosis in patients with ALD, especially with a relatively high diagnostic accuracy for early-stage liver cirrhosis. -
表 1 纳入文献的基本特征
项目 Corpe- chot等[10] Corpe- chot等[14] Corpe- chot等[11] Gómez- Doming- uez等[15] Ehlken等[13] Xu等[8] Flore- ani等[6] E Anas- tasiou等[16] Hartl等[12] Guo等[9] Wu等[7] 发表年份 2014 2006 2012 2008 2016 2017 2011 2016 2016 2017 2018 国家 法国 法国 法国 西班牙 德国 中国 意大利 德国 德国 中国 中国 病因 PSC PBC、PSC PBC PBC PSC AIH PBC AIH AIH AIH OS 病例数量(例) 73 101 103 80 139 100 120 53 94 108 70 检查仪器 1 1 1 1 1 1 1 2 1 1 1 F2 AUC 0.84 0.92 0.91 NA 0.91 0.878 0.89 0.739 0.87 0.885 0.837 敏感度 0.72 0.84 0.67 NA 0.815 0.821 0.82 0.586 0.9 0.846 0.902 特异度 0.89 0.87 1 NA 0.886 0.875 0.92 0.833 0.72 0.767 0.778 阳性预测值 0.85 0.91 1 NA 0.846 0.971 0.97 0.809 0.83 0.904 0.965 阴性预测值 0.78 0.79 0.75 NA 0.861 0.486 0.59 0.624 0.84 0.657 0.538 F3 AUC 0.93 0.95 0.95 0.86 0.95 0.883 0.92 0.842 0.93 0.897 0.91 敏感度 0.93 0.91 0.9 0.56 0.9 0.8 0.9 0.818 0.83 0.796 0.844 特异度 0.83 0.9 0.93 1 0.905 0.84 0.92 0.929 0.98 0.852 0.921 阳性预测值 0.61 0.84 0.84 1 0.818 0.836 0.9 0.757 0.92 0.843 0.9 阴性预测值 0.98 0.95 0.96 0.83 0.95 0.805 0.92 0.951 0.91 0.807 0.875 F4 AUC 0.95 0.96 0.99 0.96 0.978 0.914 0.99 NA 0.96 0.878 0.966 敏感度 1 0.93 0.93 0.88 0.688 0.87 0.99 NA 0.88 0.875 1 特异度 0.88 0.95 0.99 0.98 0.978 0.896 0.94 NA 1 0.881 0.889 阳性预测值 0.56 0.78 0.93 0.88 0.917 0.713 0.77 NA 1 0.963 0.5 阴性预测值 1 0.99 0.99 0.98 0.9 0.959 1 NA 0.98 0.668 1 注:在“检查仪器”中,“1”代表“Echosens, Paris, France”,“2”代表“Siemens Healthcare Erlangen, Germany Erlangen, Germany”。  下载: 导出CSV
下载: 导出CSV
表 2 主要肝功能指标
作者 发表年份 ALT(U/L) AST(U/L) Corpechot等[10] 2014 68±60 Corpechot等[14] 2006 60 52 Corpechot等[11] 2012 76±64 60±44 Gómez-Dominguez等[15] 2008 Ehlken等[13] 2016 48 38 Xu等[8] 2017 131.5±135.7 122.5±149.9 Floreani等[6] 2011 44±36 36±20 E Anastasiou等[16] 2016 606.42±131.13 418.09±96.87 Hartl等[12] 2016 35.0±40.1 Guo等[9] 2017 146.51±137.74 115.38±91.11 Wu等[7] 2018 185.6±238.9 166.6±190.7
下载: 导出CSV
表 3 异质性检验、阈值效应、发表偏倚结果
项目 显著肝纤维化
(≥F2)进展期肝纤维化
(≥F3)早期肝硬化
(F4)P值 结果 P值 结果 P值 结果 异质性 <0.1 有 >0.1 无 >0.1 无 阈值效应 1 无 1 无 0.95 无 发表偏倚 0.37 无 0.98 无 0.14 无
下载: 导出CSV
-
[1] LYU J, ZHANG H, WANG L. Study progress of the molecular mechanisms and therapies of liver fibrosis[J]. Chin Hosp Pharm J, 2017, 37(18): 1873-1876, 1881. DOI: 10.13286/j.cnki.chinhosppharmacyj.2017.18.24.吕舰, 张洪, 王丽. 肝纤维化分子机制及治疗研究进展[J]. 中国医院药学杂志, 2017, 37(18): 1873-1876, 1881. DOI: 10.13286/j.cnki.chinhosppharmacyj.2017.18.24. [2] XIE AZ, LYU C, SHI QL, et al. Research progress on prevention and treatment of liver fibrosis by traditional Chinese medicine[J]. China Med Herald, 2020, 547(17): 34-37. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202017009.htm谢爱泽, 吕超, 石清兰, 等. 中医药防治肝纤维化机制的研究进展[J]. 中国医药导报, 2020, 547(17): 34-37. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202017009.htm [3] LIU YY, WANG XF, LI CY, et al. Effects of hepcidin on liver fibrosis by inhibiting hepatocytes apoptosis[J]. J Clin Exp Med, 2021, 20(10): 1013-1017. DOI: 10.3969/j.issn.1671-4695.2021.10.002.刘莹莹, 王晓凡, 李长英, 等. 铁调素通过抑制肝细胞凋亡在肝纤维化中的作用机制研究[J]. 临床和实验医学杂志, 2021, 20(10): 1013-1017. DOI: 10.3969/j.issn.1671-4695.2021.10.002. [4] WANG QX, MA X. Current status and perspectives of autoimmune hepatitis[J]. J Clin Hepatol, 2020, 36(4): 721-723. DOI: 10.3969/j.issn.1001-5256.2020.04.001.王绮夏, 马雄. 自身免疫性肝炎的研究现状与展望[J]. 临床肝胆病杂志, 2020, 36(4): 721-723. DOI: 10.3969/j.issn.1001-5256.2020.04.001. [5] Chinese Foundation for Hepatitis Prevention and Control; Chinese Society of Infectious Disease and Chinese Society of Hepatology, Chinese Medical Association; Liver Disease Committee of Chinese Research Hospital Association. Consensus on clinical application of transient elastography detecting liver fibrosis: A 2018 update[J]. Chin J Hepatol, 2019, 27(3): 182-191. DOI: 10.3760/cma.j.issn.1007-3418.2019.03.004.中国肝炎防治基金会, 中华医学会感染病学分会, 中华医学会肝病学分会和中国研究型医院学会肝病专业委员会. 瞬时弹性成像技术诊断肝纤维化专家共识(2018年更新版)[J]. 中华肝脏病杂志, 2019, 27(3): 182-191. DOI: 10.3760/cma.j.issn.1007-3418.2019.03.004. [6] FLOREANI A, CAZZAGON N, MARTINES D, et al. Performance and utility of transient elastography and noninvasive markers of liver fibrosis in primary biliary cirrhosis[J]. Dig Liver Dis, 2011, 43(11): 887-892. DOI: 10.1016/j.dld.2011.06.011. [7] WU HM, SHENG L, WANG Q, et al. Performance of transient elastography in assessing liver fibrosis in patients with autoimmune hepatitis-primary biliary cholangitis overlap syndrome[J]. World J Gastroenterol, 2018, 24(6): 737-743. DOI: 10.3748/wjg.v24.i6.737. [8] XU Q, SHENG L, BAO H, et al. Evaluation of transient elastography in assessing liver fibrosis in patients with autoimmune hepatitis[J]. J Gastroenterol Hepatol, 2017, 32(3): 639-644. DOI: 10.3748/wjg.v24.i6.737. [9] GUO L, ZHENG L, HU L, et al. Transient elastography (FibroScan) performs better than non-invasive markers in assessing liver fibrosis and cirrhosis in autoimmune hepatitis patients[J]. Med Sci Monit, 2017, 23: 5106-5112. DOI: 10.12659/msm.907300. [10] CORPECHOT C, GAOUAR F, EL NAGGAR A, et al. Baseline values and changes in liver stiffness measured by transient elastography are associated with severity of fibrosis and outcomes of patients with primary sclerosing cholangitis[J]. Gastroenterology, 2014, 146(4): 970-979; quiz e15-e16. DOI: 10.1053/j.gastro.2013.12.030. [11] CORPECHOT C, CARRAT F, POUJOL-ROBERT A, et al. Noninvasive elastography-based assessment of liver fibrosis progression and prognosis in primary biliary cirrhosis[J]. Hepatology, 2012, 56(1): 198-208. DOI: 10.1002/hep.25599. [12] HARTL J, DENZER U, EHLKEN H, et al. Transient elastography in autoimmune hepatitis: Timing determines the impact of inflammation and fibrosis[J]. J Hepatol, 2016, 65(4): 769-775. DOI: 10.1016/j.jhep.2016.05.023. [13] EHLKEN H, WROBLEWSKI R, CORPECHOT C, et al. Validation of transient elastography and comparison with spleen length measurement for staging of fibrosis and clinical prognosis in primary sclerosing cholangitis[J]. PLoS One, 2016, 11(10): e0164224. DOI: 10.1371/journal.pone.0164224. [14] CORPECHOT C, EL NAGGAR A, POUJOL-ROBERT A, et al. Assessment of biliary fibrosis by transient elastography in patients with PBC and PSC[J]. Hepatology, 2006, 43(5): 1118-1124. DOI: 10.1002/hep.21151. [15] GÓMEZ-DOMINGUEZ E, MENDOZA J, GARCíA-BUEY L, et al. Transient elastography to assess hepatic fibrosis in primary biliary cirrhosis[J]. Aliment Pharmacol Ther, 2008, 27(5): 441-447. DOI: 10.1111/j.1365-2036.2007.03585.x. [16] E ANASTASIOU O, BVCHTER M, A BABA H, et al. Performance and utility of transient elastography and non-invasive markers of liver fiibrosis in patients with autoimmune hepatitis: A single centre experience[J]. Hepat Mon, 2016, 16(11): e40737. DOI: 10.5812/hepatmon.40737. [17] HASHEMI SA, ALAVIAN SM, GHOLAMI-FESHARAKI M. Assessment of transient elastography (FibroScan) for diagnosis of fibrosis in non-alcoholic fatty liver disease: A systematic review and meta-analysis[J]. Caspian J Intern Med, 2016, 7(4): 242-252. [18] GENG XX, HUANG RG, LIN JM, et al. Transient elastography in clinical detection of liver cirrhosis: A systematic review and meta-analysis[J]. Saudi J Gastroenterol, 2016, 22(4): 294-303. DOI: 10.4103/1319-3767.187603. [19] TALWALKAR JA, KURTZ DM, SCHOENLEBER SJ, et al. Ultrasound-based transient elastography for the detection of hepatic fibrosis: systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2007, 5(10): 1214-1220. DOI: 10.1016/j.cgh.2007.07.020. [20] MATTOS AZ, MATTOS AA. Transient Elastography vs. aspartate aminotransferase to platelet ratio index in hepatitis C: A meta-analysis[J]. Ann Hepatol, 2017, 16(3): 349-357. DOI: 10.5604/16652681.1235477. [21] SHⅡNA T, NIGHTINGALE KR, PALMERI ML, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: basic principles and terminology[J]. Ultrasound Med Biol, 2015, 41(5): 1126-1147. DOI: 10.1016/j.ultrasmedbio.2015.03.009. [22] CASTÉRA L, FOUCHER J, BERNARD PH, et al. Pitfalls of liver stiffness measurement: A 5-year prospective study of 13, 369 examinations[J]. Hepatology, 2010, 51(3): 828-835. DOI: 10.1002/hep.23425. [23] ARENA U, LUPSOR PLATON M, STASI C, et al. Liver stiffness is influenced by a standardized meal in patients with chronic hepatitis C virus at different stages of fibrotic evolution[J]. Hepatology, 2013, 58(1): 65-72. DOI: 10.1002/hep.26343. [24] de LÉDINGHEN V, WONG VW, VERGNIOL J, et al. Diagnosis of liver fibrosis and cirrhosis using liver stiffness measurement: Comparison between M and XL probe of FibroScan®[J]. J Hepatol, 2012, 56(4): 833-839. DOI: 10.1016/j.jhep.2011.10.017. [25] LUO WP, MA H, WANG Y. Advances in the application of transient elastography in noninvasive diagnosis of liver fibrosis[J]. J Clin Hepatol, 2019, 35(3): 635-639. DOI: 10.3969/j.issn.1001-5256.2019.03.041.罗文萍, 马红, 王宇. 瞬时弹性成像在肝纤维化无创诊断中的应用进展[J]. 临床肝胆病杂志, 2019, 35(3): 635-639. DOI: 10.3969/j.issn.1001-5256.2019.03.041. -





 本文二维码
本文二维码

图(9) / 表(3)
计量
- 文章访问数: 833
- HTML全文浏览量: 438
- PDF下载量: 85
- 被引次数: 0

