
 PDF下载 ( 1986 KB)
PDF下载 ( 1986 KB)

血清IgG4水平对IgG4相关胰-肝胆疾病与非IgG4相关胰-肝胆疾病的鉴别诊断价值
DOI: 10.3969/j.issn.1001-5256.2022.06.017
伦理学声明:本研究于2021年9月16日经由南京医科大学附属淮安第一医院伦理委员会批准,批号为YX-2021-086-01,患者均签署知情同意书。
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:姜玉章、李畅、叶耘峰负责课题设计;李畅、闫雷负责实验操作,资料分析和撰写论文;王丽、韩崇旭、闫雷参与收集部分数据,修改论文;姜玉章负责拟定写作思路,指导撰写文章并最后定稿。
Value of serum IgG4 level in differential diagnosis of IgG4-related pancreatic and hepatobiliary diseases and non-IgG4-related pancreatic and hepatobiliary diseases
-
摘要:
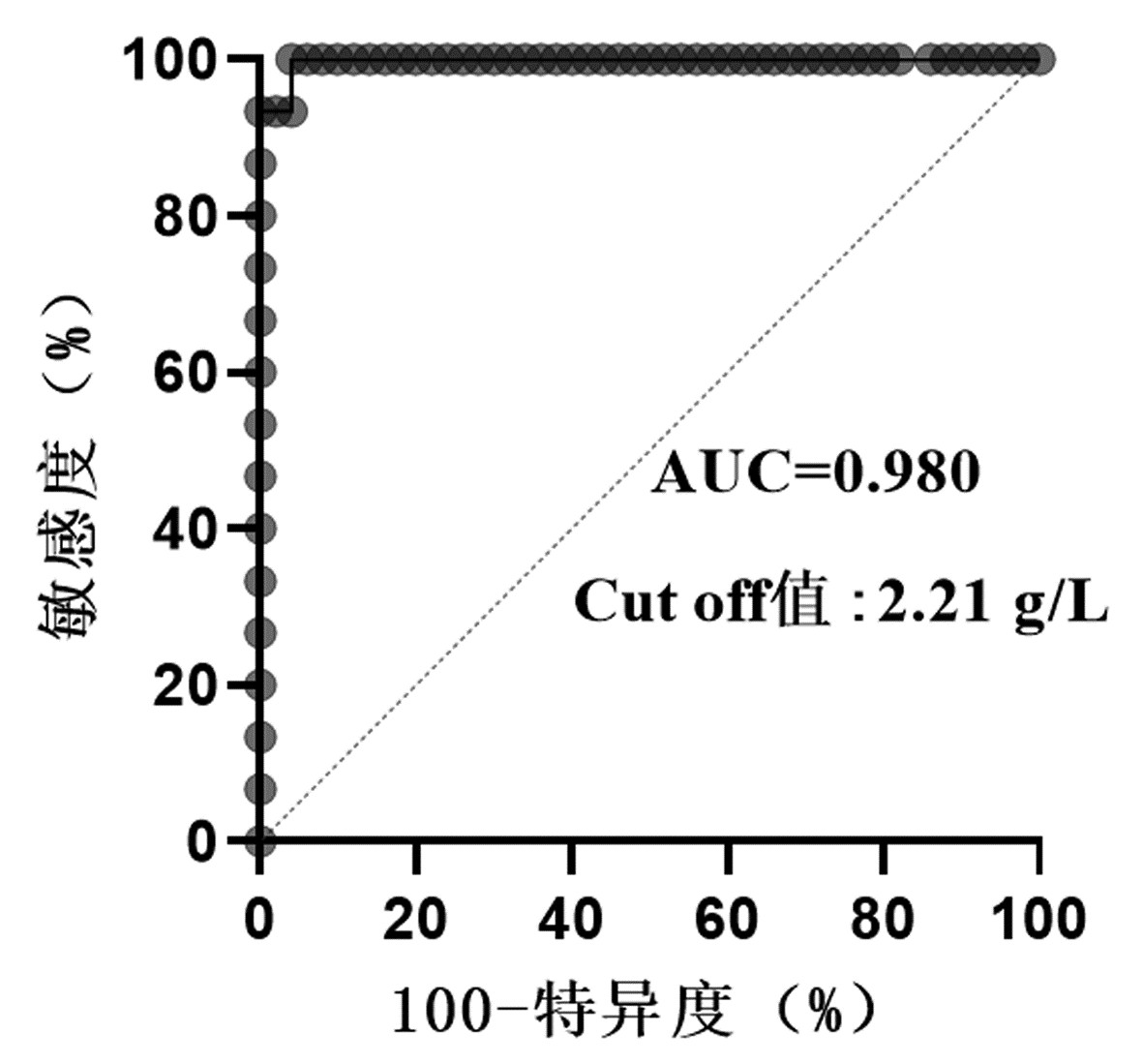
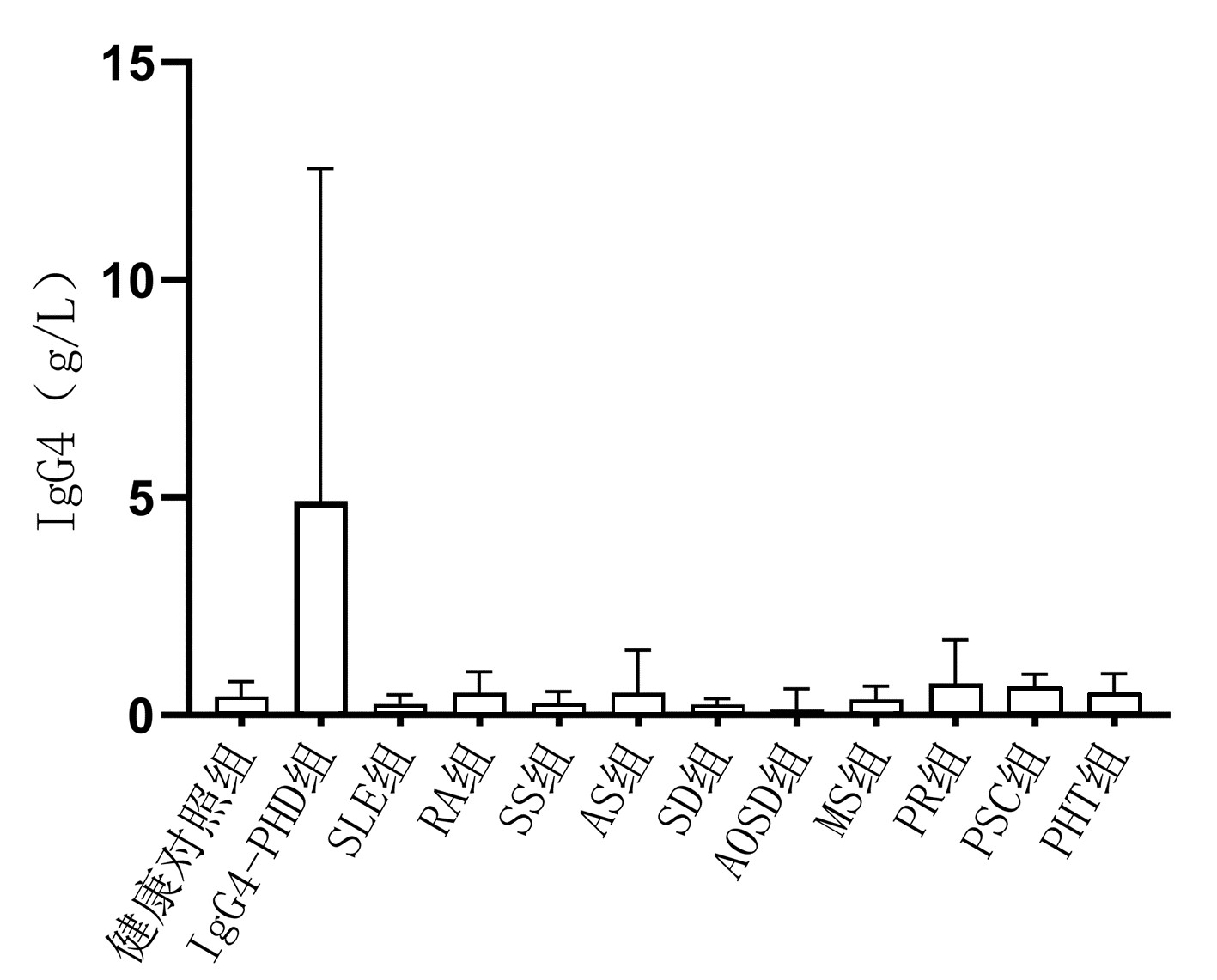
目的 探讨血清IgG4水平在鉴别诊断IgG4相关胰-肝胆疾病(IgG4-PHD)与非IgG4相关性疾病(IgG4-RD)的自身免疫性疾病中的应用价值。 方法 选择2014年8月— 2021年4月于南京医科大学附属淮安第一医院、苏北人民医院及徐州医科大学附属第一医院住院治疗的541例就诊患者和健康体检人群的临床资料,分为4组:IgG4-PHD组(n=20);非IgG4-RD自身免疫性疾病组(n=431),包括系统性红斑狼疮104例,类风湿性关节炎79例,干燥综合征174例,强直性脊柱炎16例,硬皮病11例,成人Still病4例,肌炎30例,银屑病3例,原发性硬化性胆管炎10例;胰腺肝脏胆囊恶性肿瘤组(n=40);健康对照组(n=50)。使用免疫散射比浊法测定各组样本血清IgG4水平。计量资料组间比较使用两样本Mann-Whitney U检验,计数资料组间比较采用Fisher精确检验。绘制受试者工作特征曲线(ROC曲线),确定IgG4诊断IgG4-PHD的最佳临界值。 结果 IgG4-PHD组血清IgG4水平均明显高于非IgG4-RD自身免疫性疾病各组、胰腺肝脏胆囊恶性肿瘤组和健康对照组(P值均<0.05),单独干燥综合征组血清IgG4水平显著低于健康对照组(Z=2.958,P<0.05)。分别以血清IgG4≥1.35 g/L和IgG4≥2.01 g/L作为临界值,IgG4-PHD组的阳性率明显高于非IgG4-RD自身免疫性疾病组和健康对照组,差异均具有统计学意义(P值均<0.05)。ROC曲线显示,以IgG4≥2.21 g/L作为鉴别诊断IgG4-PHD与非IgG4-RD自身免疫性疾病的临界值时,敏感度为100.00%,特异度为94.00%,AUC为0.980。 结论 非IgG4-RD自身免疫性疾病也可出现血清IgG4水平升高,而以2.21 g/L作为诊断临界值,能提升对IgG4-PHD与非IgG4-RD自身免疫性疾病的鉴别诊断效能,但仍需在临床中进一步验证。 Abstract:Objective To investigate the value of serum IgG4 level in the differential diagnosis of IgG4-related pancreatic and hepatobiliary disease (IgG4-PHD) and non-IgG4-related disease (non-IgG4-RD). Methods Clinical data were collected from 491 patients who were hospitalized and 50 individuals who underwent physical examination in Huaian No. 1 People's Hospital Affiliated to Nanjing Medical University, Subei People's Hospital, and The First Affiliated Hospital of Xuzhou Medical University from August 2014 to April 2021. The 491 patients were divided into IgG4-PHD group with 20 patients, non-IgG4-RD autoimmune disease group with 431 patients (104 patients with systemic lupus erythematosus, 79 with rheumatoid arthritis, 174 with Sjogren's syndrome, 16 with ankylosing spondylitis, 11 with scleroderma, 4 with adult-onset Still's disease, 30 with myositis, 3 with psoriasis, and 10 with primary sclerosing cholangitis), and malignant pancreatic/hepatobiliary tumor group with 40 patients, and the 50 individuals undergoing physical examination were enrolled as healthy control group. Scattering immunoturbidimetric assay was used to measure serum IgG4 concentration. The two-sample Mann-Whitney U test was used for comparison of normally distributed continuous data between groups, and the Fisher's exact test was used for comparison of categorical data between groups. The receiver operating characteristic (ROC) curve was plotted to determine the optimal cut-off value of serum IgG4 in the diagnosis of IgG4-PHD. Results The IgG4-PHD group had a significantly higher serum IgG4 level than the non-IgG4-RD autoimmune disease groups, the malignant pancreatic/hepatobiliary tumor group, and the healthy control group (all P < 0.05), and the Sjogren's syndrome group had a significantly lower serum IgG4 level than the healthy control group (Z=2.958, P < 0.05). With serum IgG4 ≥1.35 g/L and IgG4 ≥2.01 g/L as the cut-off values, the IgG4-PHD group had a significantly higher positive rate than the non-IgG4-RD autoimmune disease group and the healthy control group (all P < 0.05). The ROC curve analysis showed that IgG4 had an area under the ROC curve of 0.980 in the differential diagnosis of IgG4-PHD and non-IgG4-RD autoimmune diseases, with a sensitivity of 100.00% and a specificity of 94.00% at the optimal cut-off value of 2.21 g/L. Conclusion Serum IgG4 level may also increase in non-IgG4-RD autoimmune diseases, while the cut-off value of 2.21 g/L can improve the differential diagnosis of IgG4-PHD and non-IgG4-RD autoimmune diseases, which requires further verification in clinical practice. -
Key words:
- Immunoglobulin G /
- Autoimmune Diseases /
- Diagnosis
-
表 1 各组研究对象资料
Table 1. Basic information of subjects in each group
组别 例数 男/女(例) 年龄(岁) IgG4-PHD组 20 18/2 65(61~69) 非IgG4-RD自身免疫性疾病组 SLE 104 10/94 40±14 RA 79 20/59 56±12 SS 174 20/154 54±13 AS 16 7/9 41±15 SD 11 2/9 47±10 AOSD 4 3/1 42±4 MS 30 17/13 56(43~67) PR 3 2/1 51±13 PSC 10 4/6 59±15 PHT组 40 27/13 56±16 健康对照组 50 24/26 47±15 注:SLE,系统性红斑狼疮;RA,类风湿性关节炎;SS,干燥综合征;AS,强直性脊柱炎;SD,硬皮病;AOSD,成人Still病;MS,肌炎;PR,银屑病;PSC,原发性硬化性胆管炎。  下载: 导出CSV
下载: 导出CSV
表 2 不同IgG4诊断标准下各组血清IgG4阳性率比较
Table 2. Comparison of the positive rate of serum IgG4 in each group under different diagnostic criteria of IgG4
组别 例数 阳性[例(%)] IgG4≥1.35 g/L IgG4≥2.01 g/L IgG4-PHD组 20 20(100.00) 20(100.00) 非IgG4-RD自身免疫性疾病组 431 48(11.14)1) 27(6.26)1) PHT组 40 6(15.00)1) 01) 健康对照组 50 4(8.00)1) 2(4.00)1) P值 <0.001 <0.001 注:与IgG4-PHD组比较,1)P<0.001。
下载: 导出CSV
-
[1] LANZILLOTTA M, MANCUSO G, DELLA-TORRE E. Advances in the diagnosis and management of IgG4 related disease[J]. BMJ, 2020, 369: m1067. DOI: 10.1136/bmj.m1067. [2] YANG C, LI J, ZHANG YY, et al. Imaging findings of IgG4-related sclerosing mass pancreatitis and analysis of misdiagnosis[J]. Clin Misdiagn Misther, 2021, 305(1): 13-16. DOI: 10.3969/j.issn.1002-3429.2021.01.004.杨超, 李进, 张优仪, 等. IgG4相关硬化性肿块型胰腺炎影像学表现及误诊分析[J]. 临床误诊误治, 2021, 305(1): 13-16. DOI: 10.3969/j.issn.1002-3429.2021.01.004. [3] DELLA-TORRE E, LANZILLOTTA M, DOGLIONI C. Immunology of IgG4-related disease[J]. Clin Exp Immunol, 2015, 181(2): 191-206. DOI: 10.1111/cei.12641. [4] WALLACE ZS, ZHANG Y, PERUGINO CA, et al. Clinical phenotypes of IgG4-related disease: an analysis of two international cross- sectional cohorts[J]. Ann Rheum Dis, 2019, 78(3): 406-412. DOI: 10.1136/annrheumdis-2018-214603. [5] LANZILLOTTA M, CAMPOCHIARO C, MANCUSO G, et al. Clinical phenotypes of IgG4-related disease reflect different prognostic outcomes[J]. Rheumatology (Oxford), 2020, 59(9): 2435-2442. DOI: 10.1093/rheumatology/keaa221. [6] MILOSLAVSKY EM, NADEN RP, BIJLSMA JW, et al. Development of a Glucocorticoid Toxicity Index (GTI) using multicriteria decision analysis[J]. Ann Rheum Dis, 2017, 76(3): 543-546. DOI: 10.1136/annrheumdis-2016-210002. [7] GHAZALE A, CHARI ST, ZHANG L, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy[J]. Gastroenterology, 2008, 134(3): 706-715. DOI: 10.1053/j.gastro.2007.12.009. [8] OTSUKI M, CHUNG JB, OKAZAKI K, et al. Asian diagnostic criteria for autoimmune pancreatitis: consensus of the Japan-Korea Symposium on Autoimmune Pancreatitis[J]. J Gastroenterol, 2008, 43(6): 403-408. DOI: 10.1007/s00535-008-2205-6. [9] WALLACE ZS, NADEN RP, CHARI S, et al. The 2019 American College of Rheumatology/European League Against Rheumatism classification criteria for IgG4-related disease[J]. Ann Rheum Dis, 2020, 79(1): 77-87. DOI: 10.1136/annrheumdis-2019-216561. [10] ZHANG DH, ZHAO J. Pathogenesis of immunoglobulin G4-related hepatobiliary and pancreatic diseases[J]. J Clin Hepatol, 2019, 35(6): 1401-1405. DOI: 10.3969/j.issn.1001-5256.2019.06.050.张德华, 赵婕. IgG4相关性肝胆胰疾病的发病机制[J]. 临床肝胆病杂志, 2019, 35(6): 1401-1405. DOI: 10.3969/j.issn.1001-5256.2019.06.050. [11] OKAZAKI K, UCHIDA K, IKEURA T, et al. Current concept and diagnosis of IgG4-related disease in the hepato-bilio-pancreatic system[J]. J Gastroenterol, 2013, 48(3): 303-314. DOI: 10.1007/s00535-012-0744-3. [12] TANAKA A. IgG4-related sclerosing cholangitis and primary sclerosing cholangitis[J]. Gut Liver, 2019, 13(3): 300-307. DOI: 10.5009/gnl18085. [13] XU WL, LING YC, WANG ZK, et al. Diagnostic performance of serum IgG4 level for IgG4-related disease: A meta-analysis[J]. Sci Rep, 2016, 6(2): 32035. DOI: 10.1038/srep32035. [14] KHOSROSHAHI A, WALLACE ZS, CROWE JL, et al. International consensus guidance statement on the management and treatment of IgG4-related disease[J]. Arthritis Rheumatol, 2015, 67(7): 1688-1699. DOI: 10.1002/art.39132. [15] BERNASCONI L, MUNDWILER E, REGENASS S, et al. Variable and inaccurate serum IgG4 levels resulting from lack of standardization in IgG subclass assay calibration[J]. Clin Chem Lab Med, 2019, 57(11): 1777-1783. DOI: 10.1515/cclm-2019-0261. [16] TANG J, CAI S, YE C, et al. Biomarkers in IgG4-related disease: A systematic review[J]. Semin Arthritis Rheum, 2020, 50(2): 354-359. DOI: 10.1016/j.semarthrit.2019.06.018. [17] VALENZUELA NM, SCHAUB S. The biology of IgG subclasses and their clinical relevance to transplantation[J]. Transplantation, 2018, 102(1S Suppl 1): S7-S13. DOI: 10.1097/TP.0000000000001816. [18] USAMI Y, SUGANO M, UEHARA T, et al. Cut-off values of serum IgG4 among three reagents, including a novel IgG4 reagent: A multicenter study[J]. Sci Rep, 2021, 11(1): 7280. DOI: 10.1038/s41598-021-86024-5. [19] ZEGERS I, KELLER T, SCHREIBER W, et al. Characterization of the new serum protein reference material ERM-DA470k/IFCC: Value assignment by immunoassay[J]. Clin Chem, 2010, 56(12): 1880-1888. DOI: 10.1373/clinchem.2010.148809. -

 本文二维码
本文二维码
图(2) / 表(2)
计量
- 文章访问数: 482
- HTML全文浏览量: 125
- PDF下载量: 50
- 被引次数: 0

