
 PDF下载 ( 2776 KB)
PDF下载 ( 2776 KB)

儿童颅咽管瘤术后出现肝肺综合征1例报告
DOI: 10.3969/j.issn.1001-5256.2022.07.030
Hepatopulmonary syndrome after craniopharyngioma operation in children: A case report
-
-
Key words:
- Craniopharyngioma /
- Hepatopulmonary Syndrome /
- Non-alcoholic Fatty Liver Disease /
- Child
-

图 1 术前、术后垂体MRI检查
注: a,术前,鞍上区占位,侧脑室扩大,第三脑室受压扩张;b,术前,增强扫描病变边缘强化;c,术后,鞍区术后改变,垂体柄未见显示。
Figure 1. MRI appearance of the patient's pituitary gland before and after surgery
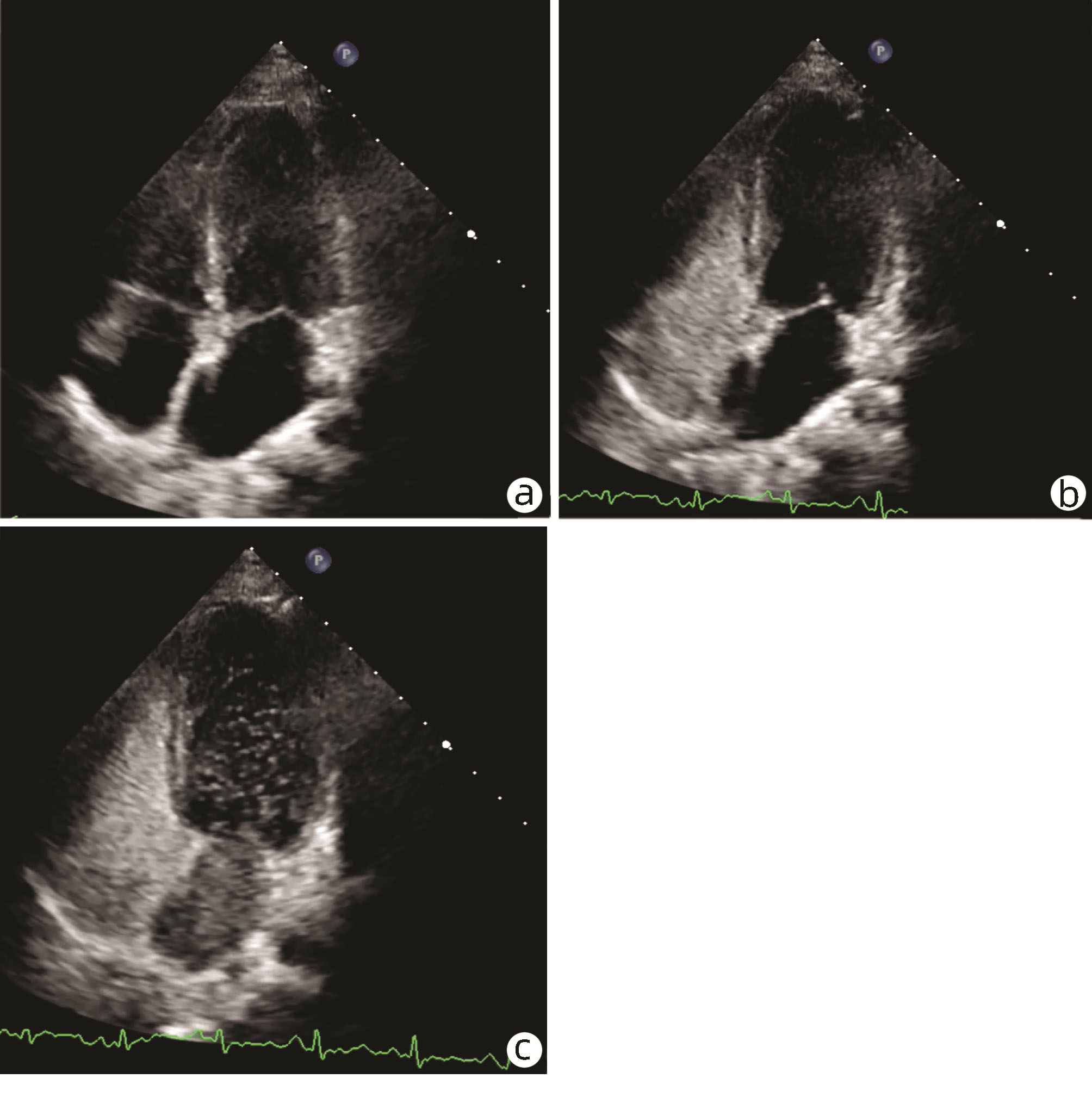
图 2 增强经胸超声心动图造影
注:a,注射震荡的生理盐水前;b,注射震荡的生理盐水右心房和右心室出现微泡显像;c,4个心动周期左右左心内出现较浓密的微泡显像。
Figure 2. Contrast-enhanced transthoracic echocardiography of the patient

图 3 血管造影检查
注:a,肺动脉造影显示,肺小动脉走行不规则、扩张;b,门静脉造影显示门静脉扩张,染色较淡。
Figure 3. Angiography of the patient
表 1 本例患儿治疗前后代谢指标及垂体功能变化
Table 1. Changes of metabolic indexes and pituitary hormone before and after treatment
项目 治疗前 出院1个月 出院3个月 出院6个月 正常范围 一般情况 不能离氧 间断吸氧 安静状态无需吸氧,行走数百米需吸氧 无氧情况下上3楼,行走数百米 身高(cm)(位于生长曲线百分位数) 135(<3rd NGC) 135.6(<3rd NGC) 137(<3rd NGC) 141(<3rd NGC) 体质量(kg) 35.5 35 38 38 ALT(U/L) 82 78 37 52 7~45 AST(U/L) 187 177 61 75 10~50 TC(mmol/L) 2.06 2.77 2.4 2.51 2.8~4.8 TG(mmol/L) 0.99 1.0 1.27 1.36 0.32~1.46 LDL(mmol/L) 1.74 1.71 1.52 1.62 1.55~2.86 TBil(μmol/L) 69.1 59.9 33.4 39.1 2~19 Alb(g/L) 38.9 43.7 44.3 44.1 39~53 血糖(mmol/L) 4.18 4.04 4.39 4.07 3.89~6.11 胰岛素(μIU/mL) 39.3 34.9 29.6 24.8 3~25 IGF-1(ng/mL) <25 222 279 361 183~850 TSH(μIU/mL) 2.59 0.743 0.331 0.658 0.51~6.27 FT3(pmol/L) 3.73 3.76 4.80 5.07 5.2~8.6 FT4(pmol/L) 7.34 10.59 12.83 14.32 12~22 ACTH(pg/mL) 12.7 <10 11.8 <10 0~46 皮质醇(nmol/L) <13.8 509.3 188.47 95.6 145.4~619.4 LH(mIU/mL) 0.03 - - <0.3 0.5~9.0 FSH(mIU/mL) 0.67 - - <0.07 0.4~8.6 E2(pmol/L) <43.31 - - <43.31 36.7~1101.0 泌乳素(μIU/mL) 1122.28 - - 616.73 63.60~305.28 透明质酸(ng/mL) 299 101 145 175 <100 层粘连蛋白(ng/mL) 60.7 31.5 26.7 27.9 <50 Ⅲ型前胶原N端(ng/mL) 422 105 325 353 <30 Ⅳ型胶原(ng/mL) 129 118 108 99 <30 注:LDL,低密度脂蛋白胆固醇血症;TSH,促甲状腺激素;FT3,游离三碘甲腺原氨酸;FT4,游离四碘甲状腺原氨酸;ACTH,促肾上腺皮质激素;LH,促黄体生成素;FSH,促卵泡刺激素;E2,雌二醇。  下载: 导出CSV
下载: 导出CSV
表 2 已报道的6例垂体功能减退伴HPS患者的临床特征
Table 2. Clinical features of six reported cases of hypopituitarism with HPS
项目 病例1[8] 病例2[9] 病例3[10] 病例4[11] 病例5[12] 病例6[13] 诊断年龄 23岁 18岁 16岁 17岁 15岁 35岁 性别 男 女 男 女 男 男 垂体疾患 2岁诊断垂体柄阻断综合征 11岁行颅咽管瘤手术治疗 诊断HPS时发现鞍上区占位,活检未见肿瘤组织 14岁诊断朗格汉斯组织细胞增生症,予放疗及鞘内化疗 11岁时诊断成熟畸胎瘤,手术治疗 31岁时诊断垂体瘤,手术治疗 既往治疗情况 予rhGH及雄激素治疗至18岁停药 予优甲乐、氢化可的松、去氨加压素、雌激素治疗,15岁二甲双胍口服,后失访2年 既往诊断尿崩症,间断予鼻内去氨加压素 去氨加压素、雌二醇贴及生理剂量的糖皮质激素 术后鼻内去氨加压素、糖皮质激素、甲状腺素、rhGH治疗;术后1年半停药 术后未予垂体激素替代治疗;27岁时发现患乙型肝炎,未正规治疗 身高(cm) 172 168.3 160 160.1 - - 体质量(kg) 60 54.3 68 91.1 95 - BMI(kg/m2) 20.2 19.2 26.6 35.5 29.3 - 第二性征 无阴毛、第二性征发育不良 Tanner Ⅲ期 无第二性征发育 Tanner Ⅱ~Ⅲ期无初潮 - - 动脉血气分析 PaCO2 49.8 mmHgPaO2 39.5 mmHg - SO2 70% 静息时SO2 88%活动时SO2 76% PaO2 51 mmHg PaO2<50 mmHg 血脂 TG 72 mg/dL TG 123 mg/dLTC 113mg/dL - 描述有代谢综合征 - - 血糖 82 mg/dL 126 mg/dL - 描述有代谢综合征 72 mg/dL - 胰岛素 - - - 描述有代谢综合征 22.8 μIU/mLHOMA-IR 4.05 - 肝功能 ALT 42 U/LAST 78 U/LTBil 1.1 mg/dLAlb 3.5 g/dL ALT 103 U/LAST 104 U/LAlb 4.3 g/dL ALT 39 U/L描述胆红素和Alb正常范围 ALT 46 U/LAST 67 U/LTBil 0.7 mg/dL ALT 16 U/LAST 22 U/LTBil 2.9 mg/dLAlb 3.9 g/dL ALT 191 U/LAST 287 U/LTBil 63.1 μmol/LAlb 19.7 g/L 生长激素 0.03 ng/mL 激发后峰值0.1 ng/mL 全垂体功能低下 描述有垂体功能低下 激发后峰值0.1 ng/mL - IGF-1 <4 ng/mL 67.2 ng/mL 全垂体功能低下 描述有垂体功能低下 71 ng/mL - 甲状腺功能 促甲状腺激素释放激素刺激试验显示反应延迟 TSH 0.22 μU/mL(0.5~6.5)FT4 0.91 ng/dL(0.8~1.9) 全垂体功能低下 描述有垂体功能低下 TSH 0.152 μIU/mLFT3 1.12 pg/mLFT4 0.69 ng/mL TSH 2.4 mU/mLFT4 5.06 pmol/L 肾上腺功能 ACTH<2.0 pg/mL皮质醇24.5 μg/dL 激发后皮质醇峰值0.38 μg/dL(>20) 全垂体功能低下 描述有垂体功能低下 ACTH 6.0 pg/mL皮质醇14.3 μg/dL 皮质醇4.0 mmol/L 性激素 LH<0.2 mIU/mLFSH 0.3 mIU/mLTesto<5.0 ng/mLPRL 7.0 ng/mL 激发后LH峰值3.6 mIU/mL(>10);FSH峰值0.18 mIU/mL(>2)E2 12.6 pg/mL 全垂体功能低下 描述有垂体功能低下 LH<0.1 mIU/mLFSH 0.06 mIU/mLTesto<0.03 ng/mL LH 0.3 mIU/mLFSH 8 mIU/mLTesto 0.06 ng/mL 肝活检 NASH 3~4期 小结节性肝硬化 小结节性肝硬化 伴有再生结节的NASH和明显的纤维化 弥漫性脂肪变性和纤维化 - 治疗 再次予rhGH、Testo、左甲状腺素钠、氢化可的松替代,转氨酶下降;5个月后肝活检示NASH改善;肝纤维化指标下降;无氧情况下可正常活动及工作 予左旋甲状腺素、泼尼松龙、去氨加压素、rhGH、雌激素、醋酸甲羟孕酮、二甲双胍,转氨酶正常,但APTT持续延长,等待肝移植 诊断HPS后予甲状腺激素、rhGH、糖皮质激素、雄激素、去氨加压素治疗,7个月后,低氧血症恶化,肝移植 诊断HPS 6个月后进展为门静脉性肺动脉高压,后予华法林抗凝,西地那非和吸入伊洛前列素等肺血管扩张剂治疗 肝移植;术后1年再次出现脂肪肝,转氨酶升高,术后5年开始rhGH治疗;术后6年,二甲双胍及格列美脲治疗,随访10年,转氨酶正常,脂肪肝无进展 抗病毒、护肝,予糖皮质激素、甲状腺素治疗;呼吸困难有所改善,低氧血症仍存在;等待肝移植 注:Testo,睾酮;HOMA-IR,胰岛素抵抗指数;-,未描述。
下载: 导出CSV
-
[1] XI ST, WU XY, PAN J, et al. Craniopharyngioma treatment expert consensus (2016)[J]. Natl Med J China, 2017, 97(17): 1283-1289. DOI: 37.3760/cma.j.issn.0376-2491.2017.17.002.漆松涛, 伍学焱, 潘军, 等. 颅咽管瘤治疗专家共识(2016)[J]. 中华医学杂志, 2017, 97(17): 1283-1289. DOI: 37.3760/cma.j.issn.0376-2491.2017.17.002. [2] FUJIO A, KAWAGISHI N, ECHIZENYA T, et al. Long-term survival with growth hormone replacement after liver transplantation of pediatric nonalcoholic steatohepatitis complicating acquired hypopituitarism[J]. Tohoku J Exp Med, 2015, 235(1): 61-67. DOI: 10.1620/tjem.235.61. [3] KANG SJ, KWON A, JUNG MK, et al. High prevalence of nonalcoholic fatty liver disease among adolescents and young adults with hypopituitarism due to growth hormone deficiency[J]. Endocr Pract, 2021, 27(11): 1149-1155. DOI: 10.1016/j.eprac.2021.06.003. [4] YUAN XX, ZHU HJ, PAN H, et al. Clinical characteristics of non-alcoholic fatty liver disease in Chinese adult hypopituitary patients[J]. World J Gastroenterol, 2019, 25(14): 1741-1752. DOI: 10.3748/wjg.v25.i14.1741. [5] STEFAN N, HÄRING HU, CUSI K. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies[J]. Lancet Diabetes Endocrinol, 2019, 7(4): 313-324. DOI: 10.1016/S2213-8587(18)30154-2. [6] KROWKA MJ, FALLON MB, KAWUT SM, et al. International liver transplant society practice guidelines: diagnosis and management of hepatopulmonary syndrome and portopulmonary hypertension[J]. Transplantation, 2016, 100(7): 1440-1452. DOI: 10.1097/TP.0000000000001229. [7] CEZA MR, GARCIA E, ANSELMI CE, et al. Prevalence and characteristics of hepatopulmonary syndrome in children with cirrhosis in southern Brazil[J]. Eur J Gastroenterol Hepatol, 2019, 31(1): 10-15. DOI: 10.1097/MEG.0000000000001207. [8] TORⅡ N, ICHIHARA A, MIZUGUCHI Y, et al. Hormone-replacement therapy for hepatopulmonary syndrome and NASH associated with hypopituitarism[J]. Intern Med, 2018, 57(12): 1741-1745. DOI: 10.2169/internalmedicine.0027-17. [9] JUNG D, SEO GH, KIM YM, et al. Hepatopulmonary syndrome caused by hypothalamic obesity and nonalcoholic fatty liver disease after surgery for craniopharyngioma: a case report[J]. Ann Pediatr Endocrinol Metab, 2018, 23(1): 51-55. DOI: 10.6065/apem.2018.23.1.51. [10] JONAS MM, KRAWCZUK LE, KIM HB, et al. Rapid recurrence of nonalcoholic fatty liver disease after transplantation in a child with hypopituitarism and hepatopulmonary syndrome[J]. Liver Transpl, 2005, 11(1): 108-110. DOI: 10.1002/lt.20332. [11] JUSTINO H, SANDERS K, MCLIN VA. Rapid progression from hepatopulmonary syndrome to portopulmonary hypertension in an adolescent female with hypopituitarism[J]. J Pediatr Gastroenterol Nutr, 2010, 50(3): 334-336. DOI: 10.1097/MPG.0b013e3181a1c496. [12] FUJIO A, KAWAGISHI N, ECHIZENYA T, et al. Long-term survival with growth hormone replacement after liver transplantation of pediatric nonalcoholic steatohepatitis complicating acquired hypopituitarism[J]. Tohoku J Exp Med, 2015, 235(1): 61-67. DOI: 10.1620/tjem.235.61. [13] LIU SH, YANG XD, WANG YT. Hepatopulmonary syndrome complicated with hypophysis: a case report and literature review[J]. Chongqing Med, 2013, 42(1): 114-115. DOI: 10.3969/j.issn.1671-8348.2013.01.046.刘韶华, 杨小东, 王妍亭. 肝肺综合征合并腺垂体功能减退症1例的报道及文献复习[J]. 重庆医学, 2013, 42(1): 114-115. DOI: 10.3969/j.issn.1671-8348.2013.01.046. [14] KHAN MJ, HUMAYUN KN, DONALDSON M, et al. Longitudinal changes in body mass index in children with craniopharyngioma[J]. Horm Res Paediatr, 2014, 82(6): 372-379. DOI: 10.1159/000368798. [15] XIAO WS, LE YY, ZENG SL, et al. Research advances in the pathogenesis of nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2020, 36(8): 1874-1879. DOI: 10.3969/j.issn.1001-5256.2020.08.043.肖伟松, 乐滢玉, 曾胜澜, 等. 非酒精性脂肪性肝病的发病机制研究进展[J]. 临床肝胆病杂志, 2020, 36(8): 1874-1879. DOI: 10.3969/j.issn.1001-5256.2020.08.043. [16] WILLIAMS KW, ELMQUIST JK. From neuroanatomy to behavior: central integration of peripheral signals regulating feeding behavior[J]. Nat Neurosci, 2012, 15(10): 1350-1355. DOI: 10.1038/nn.3217. [17] HILL JW, ELIAS CF, FUKUDA M, et al. Direct insulin and leptin action on pro-opiomelanocortin neurons is required for normal glucose homeostasis and fertility[J]. Cell Metab, 2010, 11(4): 286-297. DOI: 10.1016/j.cmet.2010.03.002. [18] FUJⅡ H, KAWADA N, JSG-NAFLD JSGON. The role of insulin resistance and diabetes in nonalcoholic fatty liver disease[J]. Int J Mol Sci, 2020, 21(11): 4753-4761. DOI: 10.3390/ijms21113863. [19] NISHIZAWA H, TAKAHASHI M, FUKUOKA H, et al. GH-independent IGF-I action is essential to prevent the development of nonalcoholic steatohepatitis in a GH-deficient rat model[J]. Biochem Biophys Res Commun, 2012, 423(2): 295-300. DOI: 10.1016/j.bbrc.2012.05.115. [20] EVANS LM, DAVIES JS, ANDERSON RA, et al. The effect of GH replacement therapy on endothelial function and oxidative stress in adult growth hormone deficiency[J]. Eur J Endocrinol, 2000, 142(3): 254-262. DOI: 10.1530/eje.0.1420254. [21] LU XL, JIANG YY, CAO Q. The role of oxidative stress and nuclear factor erythroid 2-related factor 2 in nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2020, 36(4): 924-927. DOI: 10.3969/j.issn.1001-5256.2020.04.048.陆孝良, 蒋元烨, 曹勤. 氧化应激与核因子E2相关因子2在非酒精性脂肪性肝病中的作用[J]. 临床肝胆病杂志, 2020, 36(4): 924-927. DOI: 10.3969/j.issn.1001-5256.2020.04.048. [22] The Subspecialty Group of Endocrinologic, Hereditary and Metabolic Diseases, the Society of Pediatrics, Chinese Medical Association. Expert consensus on the diagnosis and management of growth hormone deficiency during the transition period[J]. China J Pediatr, 2020, 58(6): 455-460. DOI: 10.3760/cma.j.cn112140-20200314-00237.中华医学会儿科学分会内分泌遗传代谢学组, 中华儿科杂志编辑委员会. 过渡期生长激素缺乏症诊断及治疗专家共识[J]. 中华儿科杂志, 2020, 58(6): 455-460. DOI: 10.3760/cma.j.cn112140-20200314-00237. [23] TAKANO S, KANZAKI S, SATO M, et al. Effect of growth hormone on fatty liver in panhypopituitarism[J]. Arch Dis Child, 1997, 76(6): 537-538. DOI: 10.1136/adc.76.6.537. [24] GRILO-BENSUSAN I, PASCASIO-ACEVEDO JM. Hepatopulmonary syndrome: What we know and what we would like to know[J]. World J Gastroenterol, 2016, 22(25): 5728-5741. DOI: 10.3748/wjg.v22.i25.5728. -

 本文二维码
本文二维码
计量
- 文章访问数: 486
- HTML全文浏览量: 126
- PDF下载量: 44
- 被引次数: 0

