
 PDF下载 ( 2651 KB)
PDF下载 ( 2651 KB)

急性重症胆管炎的影响因素分析及风险预测评分模型的建立与评价
DOI: 10.3969/j.issn.1001-5256.2022.08.024
A multivariate analysis of acute severe cholangitis and the establishment and evaluation of a risk prediction scoring model
-
摘要:
目的 探讨急性重症胆管炎的独立危险因素与保护因素,构建急性重症胆管炎风险预测评分模型。 方法 回顾性分析中国人民解放军联勤保障部队第九四〇医院肝胆外科2016年1月—2021年7月收治的381例急性胆管炎患者的临床资料,其中非重症胆管炎患者273例,重症胆管炎患者108例。通过单因素及logistic回归分析筛选出急性重症胆管炎的独立危险因素与保护因素,并构建logistic回归模型。采用受试者工作特征曲线(ROC曲线)评估模型的区分度,校准曲线评估模型的预测精度,决策曲线分析评估模型的临床价值。运用加强Bootstrap法对模型进行内部验证,并评估模型在内部验证中的表现。通过构建网页计算器、列线图与评分系统,对模型进行可视化呈现。符合正态分布的计量资料两组间比较采用两独立样本t检验;不符合正态分布的计量资料两组间比较采用Mann-Whitney U检验;计数资料两组间比较采用χ2检验。 结果 单因素及logistic回归分析结果显示TBil(OR=1.014,95%CI:1.009~1.020,P<0.001)、中性粒细胞百分比(OR=1.128,95%CI:1.088~1.175,P<0.001)、年龄(OR=1.053,95%CI:1.027~1.082,P<0.001)为独立危险因素,Alb(OR=0.871,95%CI:0.817~0.924,P<0.001)为保护因素。将上述独立危险因素与保护因素再次纳入logistic回归进行模型拟合,得到预测模型的ROC曲线下面积为0.925(95%CI:0.897~0.952),其最佳截断值为0.245(特异度为0.817,灵敏度为0.935)。绘制校准曲线见模型预测概率近似等于实际概率,Brier值为0.098。决策曲线分析见模型在阈概率为0.1~0.9内有更高的净收益。通过内部验证,结果显示ROC曲线下面积内部验证为0.915,Brier值内部验证为0.106。 结论 TBil、中性粒细胞百分比、年龄为急性重症胆管炎的独立危险因素,Alb为保护因素,构建的风险预测评分模型有良好的区分度、校准度与临床价值,可早期对急性重症胆管炎患者进行识别,为后续的诊疗提供一定的参考。 -
关键词:
- 胆管炎 /
- Logistic模型 /
- 危险因素
Abstract:Objective To investigate the independent risk factors for acute severe cholangitis and related protective factors, and to construct a risk prediction scoring model for acute severe cholangitis. Methods A retrospective analysis was performed for the clinical data of 381 patients with acute cholangitis who were admitted to Department of Hepatobiliary Surgery, The 940th Hospital of Joint Logistics Support Force of Chinese People's Liberation Army, from January 2016 to July 2021, among whom there were 273 patients with non-severe cholangitis and 108 patients with severe cholangitis. Univariate and multivariate logistic regression analyses were used to screen out the independent risk factors for acute severe cholangitis and related protective factors, and then a logistic regression model was established. The receiver operating characteristic (ROC) curve was used to evaluate the discriminatory ability of the model, the calibration curve was used to evaluate the prediction accuracy of the model, and decision curve analysis (DCA) was used to evaluate the clinical value of the model. Moreover, the enhanced Bootstrap method was used to perform internal validation of the model and evaluate the performance of the model in internal validation. The model was visualized by the construction of Web calculator, nomogram, and scoring system. The two-independent-samples t test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the chi-square test was used for comparison of categorical data between groups. Results The univariate and multivariate logistic regression analyses showed that total bilirubin (TBil) (odds ratio [OR]=1.014, 95% confidence interval [CI]: 1.009-1.020, P < 0.001), percentage of neutrophils (OR=1.128, 95%CI: 1.088-1.175, P < 0.001), and age (OR=1.053, 95%CI: 1.027-1.082, P < 0.001) were independent risk factors, and albumin (Alb) (OR=0.871, 95%CI: 0.817-0.924, P < 0.001) was a protective factor. The above independent risk factors and protective factor were included in the logistic regression analysis for model fitting, and the predictive model obtained had an area under the ROC curve (AUC) of 0.925 (95%CI: 0.897-0.952), with a specificity of 0.817 and a sensitivity of 0.935 at the optimal cut-off value of 0.245. The calibration curve showed that the predicted probability of the model was approximately equal to the actual probability, with a Brier value of 0.098, and the decision curve analysis showed that the model had a higher net income within the threshold probability interval of 0.1-0.9. Internal validation showed an AUCinternal validation of 0.915 and a Brier valueinternal verification of 0.106. Conclusion TBil, percentage of neutrophils, and age are independent risk factors for acute severe cholangitis, while Alb is a protective factor. The established risk prediction scoring model has good discriminatory ability, calibration, and clinical value and can identify patients with acute severe cholangitis at an early stage, which provides a reference for subsequent diagnosis and treatment. -
Key words:
- Cholangitis /
- Logistic Models /
- Risk Factors
-

图 2 急性重症胆管炎风险预测模型的ROC曲线
Figure 2. ROC curve of the risk prediction model for acute severe cholangitis

图 3 急性重症胆管炎风险预测模型的校准曲线
Figure 3. Calibration curve of the risk prediction model for acute severe cholangitis
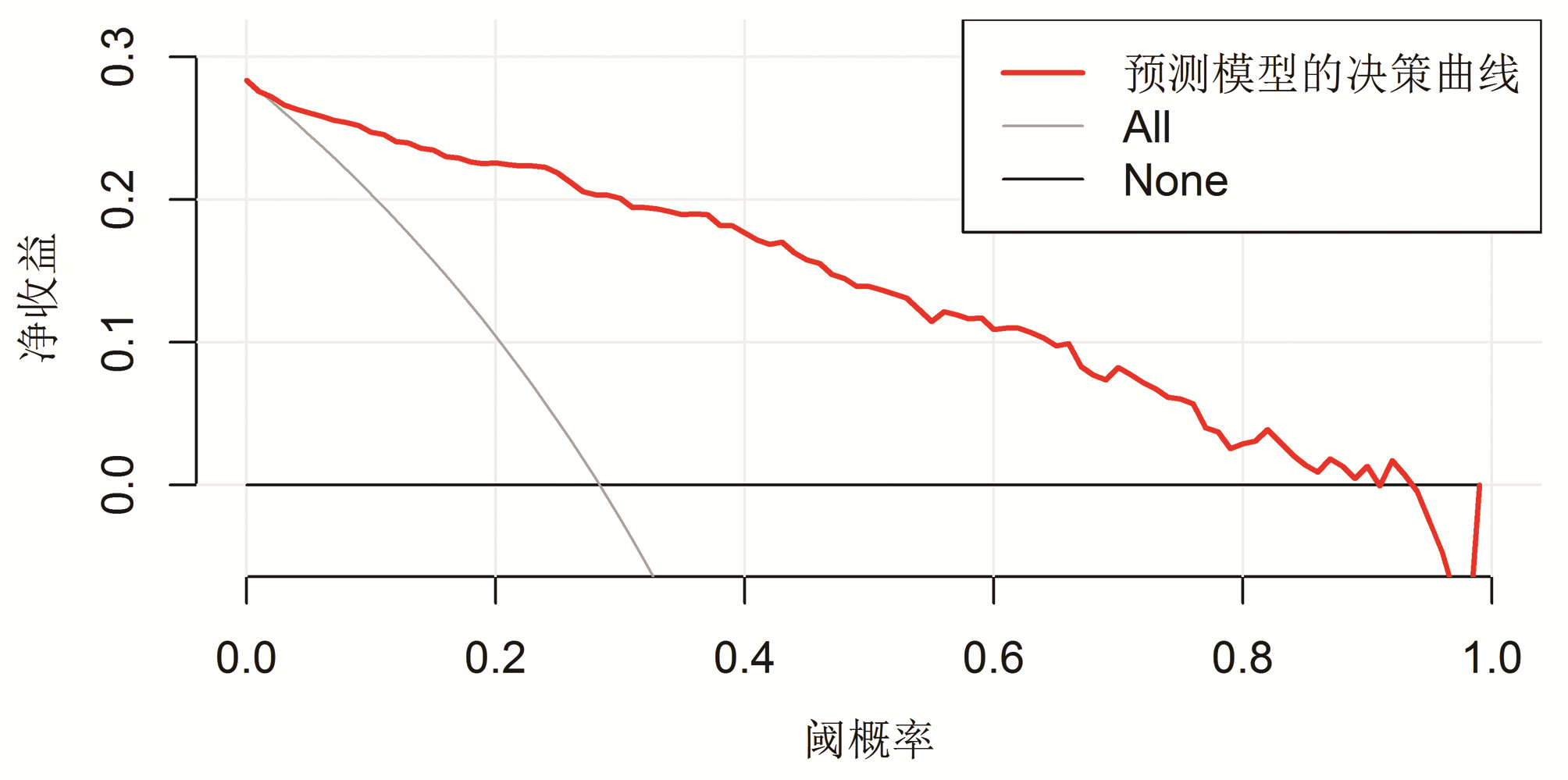
图 4 急性重症胆管炎风险预测模型的决策曲线
注:None,表示对所有患者均不进行临床干预的决策曲线;All,表示对所有患者均进行临床干预的决策曲线。
Figure 4. Decision curve of the risk prediction model for acute severe cholangitis

图 5 急性重症胆管炎风险预测模型内部验证后的校准曲线
Figure 5. Calibration curve after internal verification of the risk prediction model for acute severe cholangitis

图 6 急性重症胆管炎风险预测模型列线图
Figure 6. Nomogram of the risk prediction model for acute severe cholangitis
表 1 两组患者一般资料比较
Table 1. Comparison of general data between the two groups
项目 非重症胆管炎组(n=273) 重症胆管炎组(n=108) 统计值 P值 性别[例(%)] χ2=0.276 0.599 男 141(51.6) 59(54.6) 女 132(48.4) 49(45.4) 高血压[例(%)] 48(17.6) 30(27.8) χ2=4.941 0.026 腹部手术史[例(%)] 44(16.1) 33(30.6) χ2=10.004 0.002 贫血[例(%)] 20(7.3) 16(14.8) χ2=5.072 0.024 冠心病[例(%)] 4(1.5) 6(5.6) χ2=3.592 0.058 糖尿病[例(%)] 26(9.5) 12(11.1) χ2=0.217 0.641 年龄(岁) 56.00(38.50~68.00) 71.50(60.25~77.00) Z=-7.452 <0.001 入院体温(℃) 36.60(36.50~36.80) 36.90(36.60~37.78) Z=-6.693 <0.001 BMI(kg/m2) 23.48±3.49 23.53±3.54 t=-0.135 0.893 平均动脉压(mmHg) 90.00(82.20~96.70) 88.67(78.42~95.92) Z=-1.951 0.051  下载: 导出CSV
下载: 导出CSV
表 2 两组实验室指标及影像学资料的比较
Table 2. Comparison of laboratory and imaging data between the two groups
项目 非重症胆管炎组(n=273) 重症胆管炎组(n=108) 统计值 P值 WBC(×109/L) 6.98(5.41~9.42) 11.22(8.17~15.27) Z=-7.936 <0.001 中性粒细胞计数(×109/L) 5.19(3.60~7.95) 10.23(7.19~13.62) Z=-8.934 <0.001 淋巴细胞计数(×109/L) 1.05(0.70~1.50) 0.55(0.32~0.85) Z=-7.824 <0.001 淋巴细胞百分比(%) 16.60(8.75~24.55) 4.80(2.70~7.60) Z=-10.089 <0.001 中性粒细胞百分比(%) 75.50(65.15~86.70) 91.60(86.10~94.98) Z=-10.227 <0.001 中性粒细胞计数/淋巴细胞计数 4.58(2.68~9.86) 18.88(11.60~35.16) Z=-10.091 <0.001 血小板计数/淋巴细胞计数 170.41(122.38~263.74) 216.56(136.92~344.74) Z=-2.318 0.020 TBil(μmol/L) 38.87(23.25~72.48) 87.67(50.73~145.75) Z=-7.689 <0.001 DBil(μmol/L) 23.35(10.75~52.76) 59.57(37.33~108.23) Z=-7.798 <0.001 IBil(μmol/L) 14.30(8.93~21.90) 24.75(14.90~37.18) Z=-5.819 <0.001 ALP(U/L) 194.50(126.50~291.75) 245.00(164.25~440.50) Z=-3.600 <0.001 Alb(g/L) 41.90±5.77 35.83±5.81 t=9.226 <0.001 前白蛋白(mg/L) 201.08±73.25 127.99±70.72 t=8.822 <0.001 胆总管直径≥1.5 cm[例(%)] 73(26.7) 50(46.3) χ2=13.370 <0.001 AST(U/L) 123.00(46.25~256.75) 128.00(69.50~235.75) Z=-0.829 0.407 ALT(U/L) 175.00(75.25~340.50) 145.00(80.00~255.50) Z=-1.228 0.219 多发结石[例(%)] 137(50.2) 62(57.4) χ2=1.536 0.215
下载: 导出CSV
表 3 重症胆管炎患者多因素logistic回归分析结果
Table 3. Results of multivariate logistic regression analysis in patients with severe cholangitis
变量 β值 Wald SE OR(95%CI) P值 年龄 0.051 15.047 0.013 1.053(1.027~1.082) <0.001 TBil 0.014 26.654 0.003 1.014(1.009~1.020) <0.001 Alb -0.139 19.600 0.031 0.871(0.817~0.924) <0.001 中性粒细胞百分比 0.120 38.332 0.019 1.128(1.088~1.175) <0.001 常量 -10.023 17.999 2.363 <0.001(-) <0.001 注:“-”表示无数据。
下载: 导出CSV
表 4 急性重症胆管炎风险预测评分表
Table 4. Table of risk prediction score of acute severe cholangitis
变量 数值 得分 年龄(岁) <30 0 30~<40 1 40~<50 2 50~<60 3 60~<70 4 70~<80 5 ≥80 6 Alb(g/L) <20 0 20~<30 -3 30~<40 -6 40~<50 -8 ≥50 -11 TBil(μmol/L) <20 0 20~<70 1 70~<120 3 120~<170 4 170~<220 6 220~<270 7 ≥270 8 中性粒细胞百分比(%) <50 0 50~<70 5 70~<90 10 ≥90 14
下载: 导出CSV
-
[1] Biliary Surgery Group, Surgery Branch of Chinese Medical Association. Guidelines for diagnosis and treatment of acute biliary tract infections(2021)[J]. Chin J Surg, 2021, 59(6): 422-429. DOI: 10.3760/cma.j.cn112139-20210421-00180.中华医学会外科学分会胆道外科学组. 急性胆道系统感染的诊断和治疗指南(2021版)[J]. 中华外科杂志, 2021, 59(6): 422-429. DOI: 10.3760/cma.j.cn112139-20210421-00180. [2] KIRIYAMA S, KOZAKA K, TAKADA T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholangitis (with videos)[J]. J Hepatobiliary Pancreat Sci, 2018, 25(1): 17-30. DOI: 10.1002/jhbp.512. [3] YANG DX, ZHANG Y, WANG XF, et al. Application of ultrasound-guided real - time percutaneous transhepatic-cholangial or transhepatic-cholecyst drainage in treatment of acute obstructive cholangitis in primary hospitals[J]. J Clin Hepatol, 2020, 36(4): 847-849. DOI: 10.3969/j.issn.1001-5256.2020.04.027.杨东晓, 张勇, 王雪峰, 等. 超声实时引导下经皮经肝胆管或胆囊穿刺置管引流术治疗急性梗阻性胆管炎在基层医院的应用[J]. 临床肝胆病杂志, 2020, 36(4): 847-849. DOI: 10.3969/j.issn.1001-5256.2020.04.027. [4] ZHANG Z, ZHAO BM. Successful emergency treatment of esophageal and gastric varices bleeding complicated with acute obstructive suppurative cholangitis: A case report[J/CD]. Chin J Gastrointestinal Endosc (Electronic Edition), 2020, 7(4): 211-212. DOI: 10.3877/cma.j.issn.2095-7157.2020.04.009.张哲, 赵保民. 食管胃静脉曲张破裂出血合并急性梗阻性化脓性胆管炎急诊救治成功1例[J/CD]. 中华胃肠内镜电子杂志, 2020, 7(4): 211-212. DOI: 10.3877/cma.j.issn.2095-7157.2020.04.009. [5] LU W, SUN DX, GAO JH, et al. Overview of big data analysis of precision medicine and modeling key technologies[J]. Chin Hosp Manage, 2021, 41(5): 19-25. https://www.cnki.com.cn/Article/CJFDTOTAL-YYGL202105009.htm路薇, 孙东旭, 高景宏, 等. 面向精准医疗的大数据分析与建模关键技术综述[J]. 中国医院管理, 2021, 41(5): 19-25. https://www.cnki.com.cn/Article/CJFDTOTAL-YYGL202105009.htm [6] KÖNIG IR, FUCHS O, HANSEN G, et al. What is precision medicine?[J]. Eur Respir J, 2017, 50(4): 1700391. DOI: 10.1183/13993003.00391-2017. [7] KIRIYAMA S, TAKADA T, HWANG TL, et al. Clinical application and verification of the TG13 diagnostic and severity grading criteria for acute cholangitis: an international multicenter observational study[J]. J Hepatobiliary Pancreat Sci, 2017, 24(6): 329-337. DOI: 10.1002/jhbp.458. [8] TRAUNER M, FICKERT P, STAUBER RE. Inflammation-induced cholestasis[J]. J Gastroenterol Hepatol, 1999, 14(10): 946-959. DOI: 10.1046/j.1440-1746.1999.01982.x. [9] STRNAD P, TACKE F, KOCH A, et al. Liver - guardian, modifier and target of sepsis[J]. Nat Rev Gastroenterol Hepatol, 2017, 14(1): 55-66. DOI: 10.1038/nrgastro.2016.168. [10] Y1LD1Z BD, ÖZDEN S, SAYLAM B, et al. Simplified scoring system for prediction of mortality in acute suppurative cholangitis[J]. Kaohsiung J Med Sci, 2018, 34(7): 415-419. DOI: 10.1016/j.kjms.2017.12.016. [11] SCHWED AC, BOGGS MM, PHAM XD, et al. Association of admission laboratory values and the timing of endoscopic retrograde cholangiopancreatography with clinical outcomes in acute cholangitis[J]. JAMA Surg, 2016, 151(11): 1039-1045. DOI: 10.1001/jamasurg.2016.2329. [12] ZHANG F, LIU AL, GAO S, et al. Neutrophil dysfunction in sepsis[J]. Chin Med J (Engl), 2016, 129(22): 2741-2744. DOI: 10.4103/0366-6999.193447. [13] DU HW, QIN MF, WANG Q, et al. Analysis of mortality risk factors for acute cholangitis of severse type[J]. Shandong Med J, 2013, 53(7): 29-31. DOI: 10.3969/j.issn.1002-266X.2013.07.010.杜海伟, 秦鸣放, 王庆, 等. 重症急性胆管炎患者的死亡风险因素分析[J]. 山东医药, 2013, 53(7): 29-31. DOI: 10.3969/j.issn.1002-266X.2013.07.010. [14] GONG JP, WU CX, LIU CA, et al. Liver sinusoidal endothelial cell injury by neutrophils in rats with acute obstructive cholangitis[J]. World J Gastroenterol, 2002, 8(2): 342-345. DOI: 10.3748/wjg.v8.i2.342. [15] WANG RF, LYU Y, ZHANG XG. Advances in the diagnosis and treatment of severe acute cholangitis[J]. J Clin Hepatol, 2019, 35(12): 2622-2626. DOI: 10.3969/j.issn.1001-5256.2019.12.002.王荣峰, 吕毅, 张晓刚. 重症胆管炎的诊断与治疗[J]. 临床肝胆病杂志, 2019, 35(12): 2622-2626. DOI: 10.3969/j.issn.1001-5256.2019.12.002. [16] CHENG XY, NIU Q, WANG J, et al. Clinical value of emergency endoscopic retrograde cholangiopancreatography in the treatment of acute severe cholangitis secondary to common bile duct stones in the elderly[J]. Chin J Gerontol, 2022, 42(6): 1381-1384. DOI: 10.3969/j.issn.1005-9202.2022.06.031.程宪永, 牛琼, 王健, 等. 急诊ERCP治疗老年人胆总管结石继发急性重症胆管炎的临床价值[J]. 中国老年学杂志, 2022, 42(6): 1381-1384. DOI: 10.3969/j.issn.1005-9202.2022.06.031. [17] QIN YS, LI QY, YANG FC, et al. Risk factors and incidence of acute pyogenic cholangitis[J]. Hepatobiliary Pancreat Dis Int, 2012, 11(6): 650-654. DOI: 10.1016/s1499-3872(12)60240-9. [18] LIU Q, ZHOU Q, SONG M, et al. A nomogram for predicting the risk of sepsis in patients with acute cholangitis[J]. J Int Med Res, 2020, 48(1): 300060519866100. DOI: 10.1177/0300060519866100. [19] YIN M, SI L, QIN W, et al. Predictive value of serum albumin level for the prognosis of severe sepsis without exogenous human albumin administration: a prospective cohort study[J]. J Intensive Care Med, 2018, 33(12): 687-694. DOI: 10.1177/0885066616685300. [20] KENDALL H, ABREU E, CHENG AL. Serum albumin trend is a predictor of mortality in ICU patients with sepsis[J]. Biol Res Nurs, 2019, 21(3): 237-244. DOI: 10.1177/1099800419827600. [21] ARNAU-BARRÉS I, GVERRI-FERNÁNDEZ R, LUQUE S, et al. Serum albumin is a strong predictor of sepsis outcome in elderly patients[J]. Eur J Clin Microbiol Infect Dis, 2019, 38(4): 743-746. DOI: 10.1007/s10096-019-03478-2. [22] SCHNEIDER J, HAPFELMEIER A, THÖRES S, et al. Mortality risk for acute cholangitis (MAC): a risk prediction model for in-hospital mortality in patients with acute cholangitis[J]. BMC Gastroenterol, 2016, 16: 15. DOI: 10.1186/s12876-016-0428-1. [23] GRAVITO-SOARES E, GRAVITO-SOARES M, GOMES D, et al. Clinical applicability of Tokyo guidelines 2018/2013 in diagnosis and severity evaluation of acute cholangitis and determination of a new severity model[J]. Scand J Gastroenterol, 2018, 53(3): 329-334. DOI: 10.1080/00365521.2018.1430255. -

 本文二维码
本文二维码
计量
- 文章访问数: 472
- HTML全文浏览量: 84
- PDF下载量: 58
- 被引次数: 0

