
 PDF下载 ( 2160 KB)
PDF下载 ( 2160 KB)

慢性乙型肝炎患者肝纤维化程度与肾损伤的相关性分析
DOI: 10.3969/j.issn.1001-5256.2022.10.008
Correlation analysis of hepatic fibrosis and renal injury in patients with chronic hepatitis B
-
摘要:
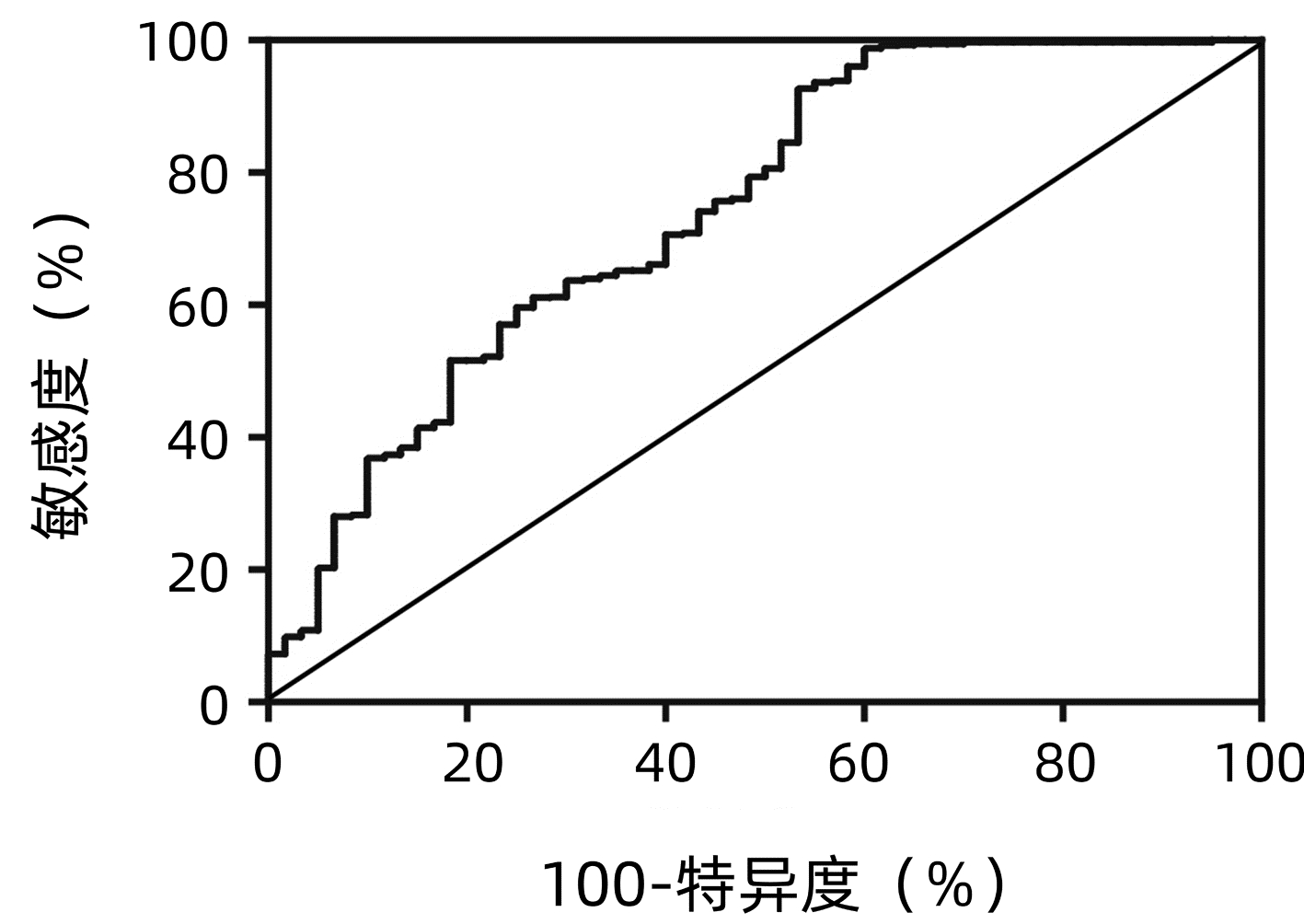
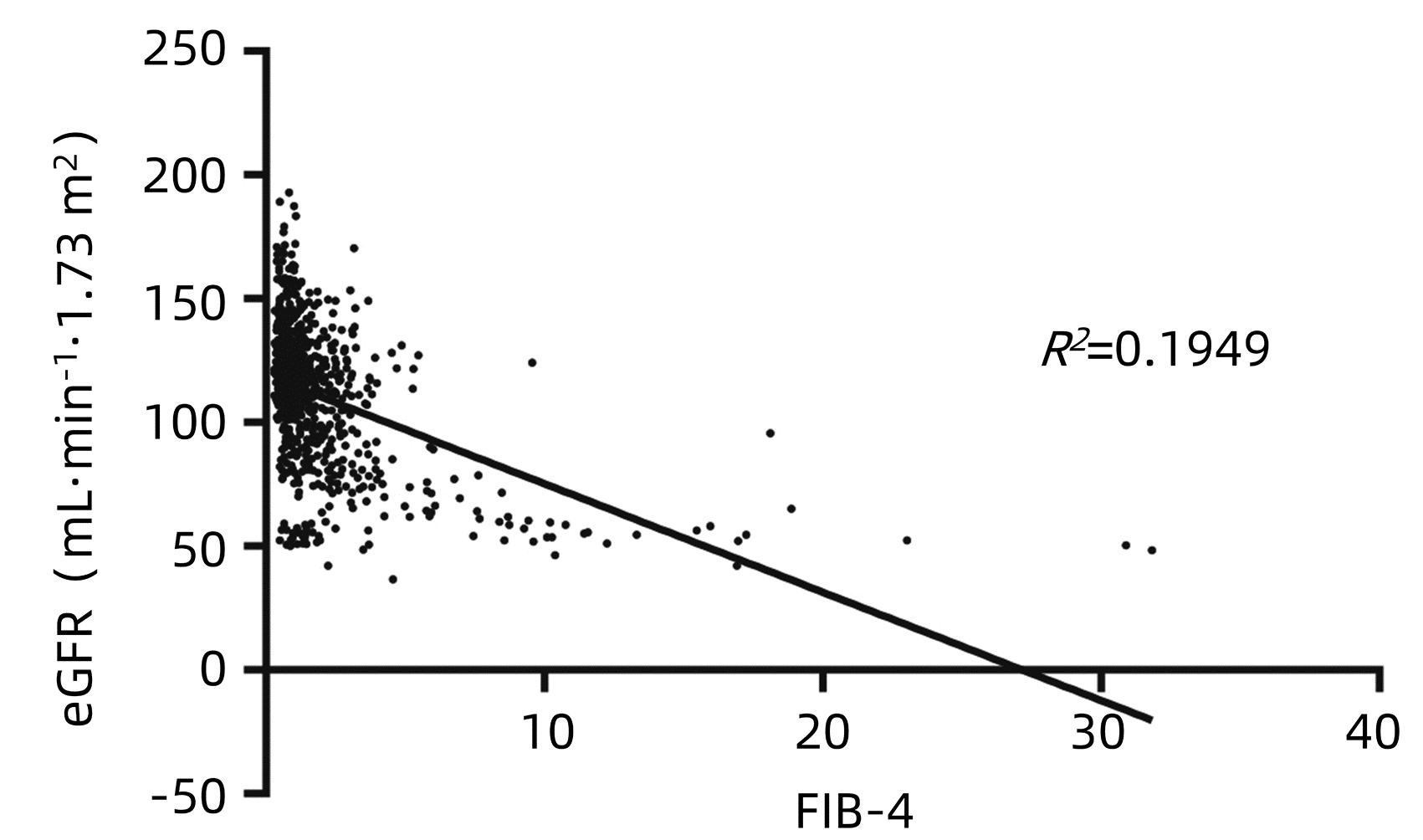
目的 分析慢性乙型肝炎(CHB)患者肝纤维化程度与肾功能损伤的关系。 方法 回顾性分析2010年5月—2019年10月798例CHB患者的肾功能,根据研究对象的肝纤维化4因子指数(FIB-4)水平将患者分为4组,Q1组(FIB-4≤0.74)200例,Q2组(0.74<FIB-4<1.13)199例,Q3组(1.13≤FIB-4<2.0)200例,Q4组(FIB-4≥2.0)199例。非正态分布计量资料多组间比较采用Kruskal-Wallis H检验。计数资料组间比较采用χ2检验。采用一元线性回归分析和Spearman偏相关分析确定FIB-4与估算肾小球滤过率(eGFR)之间的关系。采用多因素Logistic回归模型评估肾损伤的风险因素,计算优势比(OR)和95%CI。采用多分类Logistic回归分析不同分组的FIB-4与肾损伤的关系,计算OR和95%CI。绘制ROC曲线分析FIB-4在肾损伤诊断中的价值。 结果 FIB-4与年龄具有相关性(r值为0.650,P<0.001),因此采用Spearman偏相关分析对年龄、性别进行矫正。结果显示,FIB-4与ALT、AST、ALP、GGT、LDH、TBil、DBil、总蛋白、Alb、球蛋白、TBA、LAP、PLT、HBV DNA、AFP、eGFR仍有明显相关性(r值分别为0.202、0.354、0.292、0.287、0.222、0.377、0.361、-0.085、-0.412、0.168、0.422、0.247、-0.421、0.172、0.318、-0.359,P值均<0.05)。一元线性回归分析显示eGFR与FIB-4呈负相关(R2=0.1949)。多因素Logistic回归分析结果显示,HBV DNA、FIB-4是肾损伤的独立危险因素,(OR值分别为1.227、1.581,95%CI分别为1.038~1.452、1.359~1.839,P值分别为0.017、P<0.001)。多分类Logistic回归分析发现,FIB-4水平与可能的肾损伤发病呈正相关,随着FIB-4四分位数的降低,肾损伤发病率逐渐下降。FIB-4对肾损伤预测的ROC曲线下面积为0.74(95%CI: 0.67~0.82,P<0.001),敏感度为0.47,特异度为0.93,最佳截断值为3.48。 结论 CHB患者肝纤维化程度与肾损伤的风险相关。 Abstract:Objective To analyze the relationship between liver fibrosis and renal injury in patients with chronic hepatitis B (CHB). Methods We retrospectively analyzed the renal function of 798 CHB patients who were enrolled from May 2010 to October 2019. According to the quartile of fibrosis-4 (FIB-4) index, the population was divided into four groups: group Q1 (FIB-4≤0.74), group Q2 (0.74 < FIB-4 < 1.13), Q3 group (1.13≤FIB-4 < 2.0), and Q4 group (FIB-4≥2.0). The Mann-Whitney U test was used for comparison of non-normally distributed continuous data between multiple groups. The chi-square test was used for comparison of categorical data between groups. Spearman partial correlation analysis was used to determine the relationship between FIB-4 and estimated glomerular filtration rate (eGFR). Multivariate Logistic regression model was used to assess the risk factors of renal injury using odds ratio (OR) and 95% confidence intervals (CI). Multiple Logistic regression was used to analyze the relationship between FIB-4 and renal injury in different groups. Results Because FIB-4 was correlated with age (r=0.650, P < 0.001), Spearman partial correlation analysis was used to adjust for age and gender. We found FIB-4 index was significantly associated with ALT, AST, ALP, GGT, LDH, TBil, DBil, TP, Alb, Glo, TBA, LAP, PLT, HBV DNA, AFP and eGFR (r values were 0.202, 0.354, 0.292, 0.287, 0.222, 0.377, 0.361, -0.085, -0.412, 0.168, 0.422, 0.427, 0.247, -0.421, 0.172, 0.318, -0.359, respectively, all P < 0.001). eGFR was negatively correlated with FIB-4 (R2=0.192 9). Multivariate logistic regression analysis found that HBV DNA(OR=1.227, 95%CI: 1.038-1.452, P=0.017), FIB-4(OR=1.581, 95%CI: 1.359-1.839, P < 0.001) were independent risk factors for renal injury. The AUC value of FIB-4 in predicting renal injury was 0.74 (95%CI: 0.67-0.82, P < 0.001), with a sensitivity of 0.47, a specificity of 0.93, and an optimal cutoff value of 3.48. Conclusions The degree of liver fibrosis in CHB patients is associated with the risk of renal injury. -
Key words:
- Hepatitis B, Chronic /
- Liver Cirrhosis /
- Glomerular Filtration Rate /
- Renal Injury
-
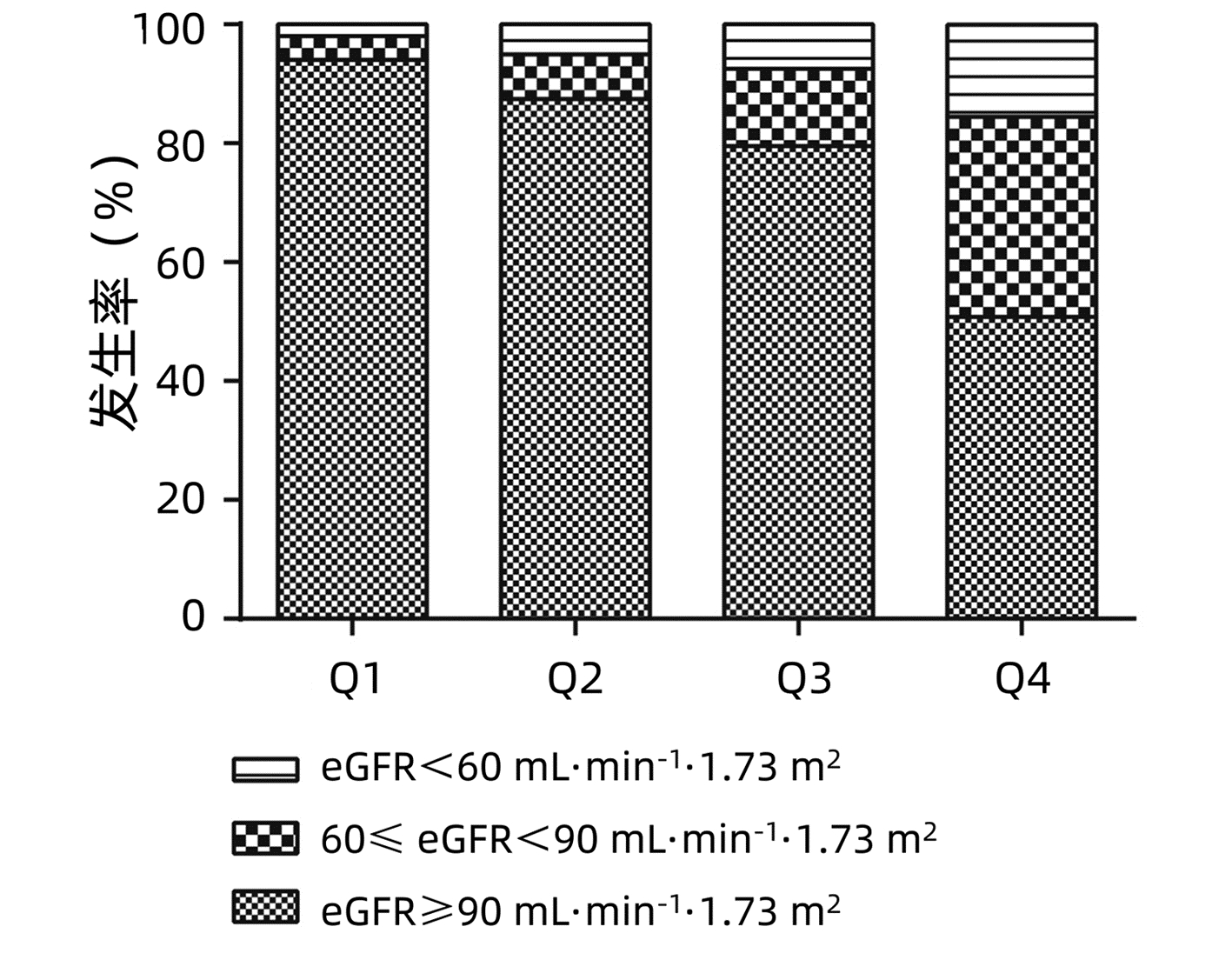
图 2 不同FIB-4组的肾损伤发生率
Figure 2. Incidence of renal function injury in different FIB-4 groups
表 1 按FIB-4分层的研究人群特征
Table 1. Characteristics of the study population stratified by the FIB-4 quartiles
指标 FIB-4 统计值 P值 Q1组(n=200) Q2组(n=199) Q3组(n=200) Q4组(n=199) 男性[例(%)] 111(55.5) 122(61.3) 110(55) 131(65.8) χ2=6.587 0.087 年龄(岁) 29(26~33) 35(31~43) 46.5(37~54) 41(52~60) H=329.27 0.001 ALT(U/L) 27.4(21.1~42.7) 25.3(18.4~42.7) 24.6(16.6~40.5) 38.2(21.7~76.7) H=38.37 0.001 AST(U/L) 22.7(20.1~27.4) 23.9(20.0~31.3) 24.2(19.9~32.3) 35.7(25.4~67.2) H=117.32 0.001 ALP(U/L) 61.1(51.0~72.3) 61.2(50.6~74.5) 64.8(53.6~79.3) 76.0(62.6~97.8) H=67.46 0.001 GGT(U/L) 18.2(14.2~25.4) 18.2(13.9~29.5) 18.3(13.4~28.3) 29.5(16.9~58.8) H=55.76 0.001 LDH(U/L) 186(167~209) 193(173~212) 189(171~210) 209(179~238) H=43.20 0.001 TBiL(mmol/L) 10.7(8.4~13.5) 11.7(9.0~15.8) 11.6(9.5~15.0) 14.9(11.3~19.6) H=62.83 0.001 DBiL(mmol/L) 2.7(1.7~3.7) 2.9(2.1~4.3) 2.9(2.3~3.9) 4.4(2.9~6.4) H=81.14 0.001 总蛋白(g/L) 74.6(71.9~77.5) 74.8(71.7~77.7) 74.2(71.3~77.2) 73.3(69.5~77.2) H=11.08 0.011 Alb(g/L) 45.3(44.3~46.9) 45.4(44.3~46.9) 44.7(43.6~46.2) 43.7(41.1~45.7) H=60.64 0.001 球蛋白(g/L) 29.2(26.9~31.7) 29.5(27.3~32.2) 29.7(26.4~32.3) 29.7(26.5~34.3) H=2.79 0.425 TBA(μmol/L) 2.0(1.4~3.0) 1.9(1.2~2.8) 2.3(1.3~4.1) 4.8(2.3~13.0) H=109.26 0.001 LAP(U/L) 51.6(46.5~58.9) 51.5(47.1~58.0) 51.1(46.1~58.1) 55.9(47.2~68.3) H=23.71 0.001 PLT(×109/L) 226.5(203.3~258.8) 190.0(169.0~221.0) 169.0(149.0~197.8) 119.0(86.0~158.0) H=342.03 0.001 BUN(mmol/L) 4.5(3.7~5.4) 4.7(3.9~5.4) 4.9(4.2~5.8) 4.9(4.2~5.8) H=12.65 0.005 甘油三酯(mmol/L) 0.8(0.7~1.1) 0.9(0.6~1.1) 0.9(0.7~1.1) 0.8(0.6~1.1) H=1.93 0.587 TC(mmol/L) 4.1(3.7~4.7) 4.1(3.6~4.7) 4.1(3.6~4.7) 4.1(3.7~4.8) H=0.28 0.963 高密度脂蛋白(mmol/L) 1.3(1.1~1.6) 1.3(1.1~1.5) 1.3(1.1~1.6) 1.4(1.1~1.7) H=2.41 0.493 低密度脂蛋白(mmol/L) 2.3(1.9~2.8) 2.3(1.9~2.9) 2.3(1.9~2.8) 2.3(1.9~2.7) H=1.57 0.667 apoA(g/L) 1.2(1.0~1.3) 1.2(1.0~1.3) 1.2(1.0~1.4) 1.2(0.9~1.4) H=7.65 0.054 apoB(g/L) 0.7(0.6~0.8) 0.7(0.6~0.9) 0.7(0.6~0.8) 0.7(0.6~0.9) H=0.72 0.868 eGFR(mL·min-1·1.73 m-2) 121.4(111.8~138.8) 121.0(108.3~134.5) 116.1(103.0~127.0) 95.6(71.3~118.7) H=117.03 0.001 HBV DNA(拷贝/mL) 3.2(2.7~7.5) 2.8(2.7~4.6) 2.7(2.7~3.9) 3.4(2.7~5.8) H=22.11 0.001 AFP(g/L) 2.0(1.3~3.3) 2.5(1.4~3.8) 2.2(1.3~3.7) 3.5(1.6~8.5) H=45.80 0.001  下载: 导出CSV
下载: 导出CSV
表 2 年龄和性别矫正后的FIB-4与临床特征的相关性
Table 2. Age-and gender-adjusted correlations between FIB-4 index and clinical characteristics
指标 r值 P值 ALT(U/L) 0.202 0.001 AST(U/L) 0.354 0.001 ALP(U/L) 0.292 0.001 GGT(U/L) 0.287 0.001 LDH(U/L) 0.222 0.001 TBiL(mmol/L) 0.377 0.001 DBiL(mmol/L) 0.361 0.001 总蛋白(g/L) -0.085 0.016 Alb(g/L) -0.412 0.001 球蛋白(g/L) 0.168 0.001 TBA(μmol/L) 0.422 0.001 LAP(U/L) 0.247 0.001 PLT(×109/L) -0.421 0.001 BUN(mmol/L) -0.046 0.192 甘油三酯(mmol/L) -0.060 0.090 TC(mmol/L) -0.056 0.113 高密度脂蛋白(mmol/L) 0.004 0.905 低密度脂蛋白(mmol/L) -0.068 0.054 apoA(g/L) -0.028 0.438 apoB(g/L) -0.035 0.328 eGFR(mL·min-1·1.73 m-2) -0.359 0.001 HBV DNA(拷贝/mL) 0.172 0.001 AFP(g/L) 0.318 0.001
下载: 导出CSV
表 3 肾损伤危险因素的Logistic回归分析
Table 3. Logistic regression analysis of risk factors of renal injury
指标 单变量 多变量 OR (95%CI) P值 OR (95%CI) P值 男性[例(%)] 0.714(0.409~1.245) 0.235 - - 年龄(岁) 1.032(1.011~1.053) 0.002 - - ALT(U/L) 1.001(1.000~1.002) 0.024 - - AST(U/L) 1.004(1.002~1.007) 0.001 - - ALP(U/L) 1.020(1.011~1.029) 0.001 - - GGT(U/L) 1.006(1.002~1.010) 0.004 - - LDH(U/L) 1.007(1.002~1.012) 0.003 - - TBiL(mmol/L) 1.027(1.011~1.043) 0.001 - - DBiL(mmol/L) 1.038(1.013~1.063) 0.003 - - 总蛋白(g/L) 0.976(0.926~1.028) 0.355 - - Alb(g/L) 0.826(0.774~0.881) 0.000 - - 球蛋白(g/L) 1.085(1.032~1.142) 0.002 - - TBA(μmol/L) 1.024(1.012~1.036) 0.001 - - LAP(U/L) 1.022(1.008~1.036) 0.002 - - PLT(×109/L) 0.987(0.982~0.991) 0.001 - - BUN(mmol/L) 0.539(0.887~1.258) 0.539 - - 甘油三酯(mmol/L) 0.951(0.553~1.637) 0.857 - - TC(mmol/L) 0.561(0.668~1.244) 0.561 - - 高密度脂蛋白(mmol/L) 0.774(0.379~1.580) 0.482 - - 低密度脂蛋白(mmol/L) 0.904(0.615~1.328) 0.606 - - apoA(g/L) 0.791(0.308~2.030) 0.626 - - apoB(g/L) 1.018(0.288~3.594) 0.978 - - HBV DNA(拷贝/mL) 1.217(1.078~1.374) 0.001 1.227(1.038~1.452) 0.017 AFP(g/L) 1.003(1.001~1.004) 0.004 - - FIB-4 1.428(1.303~1.565) 0.001 1.581(1.359~1.839) 0.001
下载: 导出CSV
表 4 FIB-4与肾损伤风险的相关性
Table 4. Association of FIB-4 with the risk of renal function injury
项目 FIB-4 P值 自变量每增加1个标准差 Q1 Q2 Q3 Q4 模型1 0.111(0.038~0.320) 0.287(0.136~0.632) 0.439(0.229~0.842) 1 0.001 2.720(2.104~3.517) 模型2 0.113(0.039~0.328) 0.289(0.138~0.608) 0.450(0.234~0.866) 1 0.001 2.713(2.094~3.514) 模型3 0.162(0.054~0.488) 0.417(0.189~0.918) 0.621(0.310~1.243) 1 0.006 2.847(2.081~3.894) 注:模型1,未进行协变量矫正;模型2,进行性别矫正后;模型3,进行性别、ALP、GGT、TBil、DBil、TBA、LAP及AFP矫正后。由于在FIB-4的计算中包含了年龄、ALT、AST和PLT等因素,因此模型未进行调整。
下载: 导出CSV
-
[1] HE P, FENG GH. Current research on the mechanism of direct damage of kidney tissue by virus in hepatitis B virus-associatednephritis[J]. Chin J Infect Dis, 2012, 30(2): 123-125. DOI: 10.3760/cma.j.issn.1000-6680.2012.02.016.何平, 冯国和. 乙型肝炎病毒相关性肾炎中病毒直接损伤肾组织作用机制研究现状[J]. 中华传染病杂志, 2012, 30(2): 123-125. DOI: 10.3760/cma.j.issn.1000-6680.2012.02.016. [2] ZHOU Y, YUAN WJ. Status of virus directdamage in the pathogenesis of hepatitis B virus-associated nephritis[J]. Chin J Neahrol, 2010, 26(8): 646-648. DOI: 10.3760/cma.j.issn.1001-7097.2010.08.021.周益, 袁伟杰. 病毒直接损伤作用在乙肝相关性肾炎发病机制中的地位[J]. 中华肾脏病杂志, 2010, 26(8): 646-648. DOI: 10.3760/cma.j.issn.1001-7097.2010.08.021. [3] TAKEKOSHI Y, TANAKA M, MIYAKAWA Y, et al. Free "small" and IgG-associated "large" hepatitis B e antigen in the serum and glomerular capillary walls of two patients with membranous glomerulonephritis[J]. N Engl J Med, 1979, 300(15): 814-819. DOI: 10.1056/NEJM197904123001502. [4] ADLER S, SALANT DJ, DITTMER JE, et al. Mediation of proteinuria in membranous nephropathy due to a planted glomerular antigen[J]. Kidney Int, 1983, 23(6): 807-815. DOI: 10.1038/ki.1983.99. [5] CHENG WR, SUN LJ, DONG HR, et al. Clinical and pathological characteristics of hepatitis B virus-associated glomerulonephritis in adults[J]. Int J Virol, 2021, 28(3): 231-235. DOI: 10.3760/cma.j.issn.1673-4092.2021.03.013.程文荣, 孙丽君, 董鸿瑞, 等. 成人乙型肝炎病毒相关性肾小球肾炎的临床及病理特点分析[J]. 国际病毒学杂志, 2021, 28(3): 231-235. DOI: 10.3760/cma.j.issn.1673-4092.2021.03.013. [6] GUPTA A, QUIGG RJ. Glomerular diseases associated with hepatitis B and C[J]. Adv Chronic Kidney Dis, 2015, 22(5): 343-351. DOI: 10.1053/j.ackd.2015.06.003. [7] AN ML, HE P. Research progress on mechanism of podocyte injury and its relationship with glomerular diseases[J]. Chin J Clin Res, 2018, 31(10): 1427-1431. DOI: 10.13429/j.cnki.cjcr.2018.10.033.安梦丽, 何平. 足细胞损伤的机制及与肾小球疾病的关系研究进展[J]. 中国临床研究, 2018, 31(10): 1427-1431. DOI: 10.13429/j.cnki.cjcr.2018.10.033. [8] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [9] REVILL PA, CHISARI FV, BLOCK JM, et al. A global scientific strategy to cure hepatitis B[J]. Lancet Gastroenterol Hepatol, 2019, 4(7): 545-558. DOI: 10.1016/S2468-1253(19)30119-0. [10] HONG YS, RYU S, CHANG Y, et al. Hepatitis B virus infection and development of chronic kidney disease: a cohort study[J]. BMC Nephrol, 2018, 19(1): 353. DOI: 10.1186/s12882-018-1154-4. [11] FABRIZI F, CERUTTI R, RIDRUEJO E. Hepatitis B virus infection as a risk factor for chronic kidney disease[J]. Expert Rev Clin Pharmacol, 2019, 12(9): 867-874. DOI: 10.1080/17512433.2019.1657828. [12] LIU Y, FAN R, CHEN J, et al. Assessment of renal function and risk factors for renal impairment in patients with hepatitis B virus-related liver cirrhosis[J]. J South Med Univ, 2014, 34(4): 472-476. DOI: 10.3969/j.issn.1673-4254.2014.04.07.刘颖, 樊蓉, 陈简, 等. 慢性乙型肝炎病毒感染相关肝硬化患者的肾功能及危险因素分析[J]. 南方医科大学学报, 2014, 34(4): 472-476. DOI: 10.3969/j.issn.1673-4254.2014.04.07. [13] DUAN Y, WANG XM, ZHAO YY, et al. Prevalence and influencing factors of chronic hepatitis B virus infection complicated with chronic kidney disease[J/CD]. Chin J Exp Clin Infect Dis(Electronic Edition), 2018, 12(5): 422-426. DOI: 10.3877/cma.j.issn.1674-1358.2018.05.002.段英, 王笑梅, 赵莹莹, 等. 慢性乙型肝炎病毒感染者合并慢性肾脏病患病率及影响因素[J/CD]. 中华实验和临床感染病杂志(电子版), 2018, 12(5): 422-426. DOI: 10.3877/cma.j.issn.1674-1358.2018.05.002. [14] ZHOU JT, LI JB. Evaluation of renal function and risk factors in patients with chronic hepatitis B[J]. Anhui Med J, 2017, 38(6): 681-684. DOI: 10.3969/j.issn.1000-0399.2017.06.002.周静婷, 李家斌. 不同程度慢性乙型肝炎患者肾功能评估及危险因素分析[J]. 安徽医学, 2017, 38(6): 681-684. DOI: 10.3969/j.issn.1000-0399.2017.06.002. [15] TARGHER G, BERTOLINI L, RODELLA S, et al. Relationship between kidney function and liver histology in subjects with nonalcoholic steatohepatitis[J]. Clin J Am Soc Nephrol, 2010, 5(12): 2166-2171. DOI: 10.2215/CJN.05050610. [16] XU HW, HSU YC, CHANG CH, et al. High FIB-4 index as an independent risk factor of prevalent chronic kidney disease in patients with nonalcoholic fatty liver disease[J]. Hepatol Int, 2016, 10(2): 340-346. DOI: 10.1007/s12072-015-9690-5. [17] SONNEVELD MJ, BROUWER WP, CHAN HL, et al. Optimisation of the use of APRI and FIB-4 to rule out cirrhosis in patients with chronic hepatitis B: results from the SONIC-B study[J]. Lancet Gastroenterol Hepatol, 2019, 4(7): 538-544. DOI: 10.1016/S2468-1253(19)30087-1. [18] LI X, ZHANG ZH, CAI Q, et al. Judgement of liver fibrosis by gama-glutamyltransferase to qHBsAg ratio in patients with chronic hepatitis B[J]. J Pract Hepatol, 2015, 18(2): 141-144. DOI: 10.3969/j.issn.1672-5069.2015.02.009.李旭, 张振华, 蔡群, 等. 谷氨酰转肽酶/HBsAg比值评估慢性乙型肝炎患者肝纤维化的价值探讨[J]. 实用肝脏病杂志, 2015, 18(2): 141-144. DOI: 10.3969/j.issn.1672-5069.2015.02.009. [19] LI Q, HUANG YX, CHEN L. The diagnostic value of γ-GT/plateletmodel for liver fibrosis and cirrhosis in patients with chronic hepatitis B[J]. Chin J Infect Dis, 2016, 34(6): 360-361. DOI: 10.3760/cma.j.issn.1000-66802016.06.009.李强, 黄玉仙, 陈良. γ-谷氨酰转肽酶/血小板计数模型对慢性乙型肝炎患者明显肝纤维化和肝硬化的诊断价值[J]. 中华传染病杂志, 2016, 34(6): 360-361. DOI: 10.3760/cma.j.issn.1000-66802016.06.009. [20] KIM WR, BERG T, ASSELAH T, et al. Evaluation of APRI and FIB-4 scoring systems for non-invasive assessment of hepatic fibrosis in chronic hepatitis B patients[J]. J Hepatol, 2016, 64(4): 773-780. DOI: 10.1016/j.jhep.2015.11.012. [21] SU XN, CAO JY, JIN Z, et al. Study on semi-quantitative analysis of liver cirrhosis by ultrasound elastography Q analysis technique[J]. Chin J Med Offic, 2021, 49(12): 1319-1322. DOI: 10.16680/j.1671-3826.2021.12.09.苏晓妮, 曹军英, 金壮, 等. 超声弹性成像Q分析技术对肝硬化半定量分析研究[J]. 临床军医杂志, 2021, 49(12): 1319-1322. DOI: 10.16680/j.1671-3826.2021.12.09. [22] FU F, WANG MY, SHI DP, et al. Evaluation of hepatic fibrosis in chronic hepatitis B with parameters obtained from multi-models of diffusion-weighted MRI[J]. Chin J Radiol, 2018, 52(2): 113-118. DOI: 10.3760/cma.j.issn.1005-1201.2018.02.007.付芳芳, 王梅云, 史大鹏, 等. 多种模型MRI扩散加权成像评估慢性乙型病毒性肝炎肝纤维化程度的价值[J]. 中华放射学杂志, 2018, 52(2): 113-118. DOI: 10.3760/cma.j.issn.1005-1201.2018.02.007. -

 本文二维码
本文二维码
计量
- 文章访问数: 376
- HTML全文浏览量: 82
- PDF下载量: 74
- 被引次数: 0

