
 PDF下载 ( 1845 KB)
PDF下载 ( 1845 KB)

aMAP评分评估门诊慢性HBV感染者肝细胞癌风险的价值分析
DOI: 10.3969/j.issn.1001-5256.2022.10.009
伦理学声明:本研究方案于2021年5月26日经由北京清华长庚医院伦理委员会审批,批号:21228-0-01(2021-5-26)。患者均签署知情同意书。
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:王丽旻、张鸿飞负责课题设计,资料分析,撰写论文;甘雨、王静月、谢思参与收集数据,修改论文;黄缘负责拟定写作思路,指导撰写文章并最后定稿。
Value of aMAP score in prediction of hepatocellular carcinoma risk in outpatients with chronic hepatitis B virus infection
-
摘要:
目的 探索肝细胞癌(HCC)风险预测模型aMAP评分对门诊慢性HBV感染者肝细胞癌风险评估的应用价值。 方法 选取2018年1月—2021年12月于北京清华长庚医院门诊就诊的慢性HBV感染者709例,计算aMAP及进行HCC风险评估。符合正态分布的计量资料组间比较采用t检验,等级资料两组间比较采用Mann-Whitney U检验。 结果 709例慢性HBV感染者中,22.4%合并酒精性肝病,11.8%合并糖尿病。18.6%合并脂肪肝,19.0%合并肝硬化,9.7%合并肝癌。71.2%的患者服用口服抗病毒药物,28.8%未用抗病毒药物。aMAP最高为75.2分,HCC低、中和高风险人数分别占70.0%、23.1%和6.9%;合并酒精性肝病、糖尿病、肝硬化患者aMAP高风险的比例高于无酒精性肝病、糖尿病、肝硬化患者(9.4% vs 6.2%,11.9% vs 6.2%,19.3% vs 4.0%),高中低风险组成比较,差异有统计学意义(P值分别为<0.01, 0.01,<0.01)。抗病毒治疗组患者aMAP变化的年均值(-1.15±1.72)分,明显低于未用抗病毒治疗者的(0.93±2.05)分(t=39.36,P<0.01)。HCC患者确诊前3年内高风险的比例分别为38.4%、26.7%、33.3%。aMAP在确诊HCC前3年均>50分,早于AFP的升高。 结论 aMAP评分作为慢性HBV感染者HCC筛查管理的工具,简单快捷,便于门诊的应用。合并酒精性肝病、肝硬化的慢性HBV感染者aMAP评分的HCC高风险比例高于无合并疾病患者的比例,口服抗病毒治疗可降低aMAP。 Abstract:Objective To assess the aMAP risk in prediction of hepatocellular carcinoma (HCC) risk in outpatients with chronic hepatitis B virus (HBV) infection. Methods A total of 709 patients with chronic HBV infection were recruited for calculation of the aMAP scores and then stratified for HCC risk statistically. The t-test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups. Results Among these 709 patients, 22.4% had complicated with alcoholic liver disease, 11.8% with diabetes mellitus. 18.6% with fatty liver, 19.0% with liver cirrhosis, and 9.7% with liver cancer. Among all patients, 71.2% received oral antiviral medicine. Moreover, the highest aMAP score was 75.2 and the low, medium and high HCC risks were 70.0%, 23.1%, and 6.9% respectively in these patients. The proportion of patients with high HCC risk was higher among those with alcohol liver disease, diabetes mellitus, and liver cirrhosis than those without these complications (9.4% vs 6.2%; 11.9% vs 6.2%; and 19.3% vs 4.0%). The mean annual change in aMAP score was 0.93±2.05 in patients without antiviral treatment that was higher than -1.15±1.72 in patients with antiviral treatment (t=39.36; P < 0.001). In addition, the proportion of these patients with high HCC risk three years before HCC diagnosis was 38.4%, 26.7%, and 33.3% respectively. The median of aMAP score was more than 50 three years before diagnosis liver cancer, data of which indicated that this change was earlier than that of AFP. Conclusion aMAP is a simple convenient marker for screening early HCC in outpatient with chronic HBV infection and complications, especially in those patients with alcohol liver disease, diabetes, and cirrhosis. Oral antiviral therapy could reduce aMAP in patients with chronic HBV infection. -
Key words:
- Carcinoma, Hepatocellular /
- Hepatitis B Virus /
- aMAP Score
-
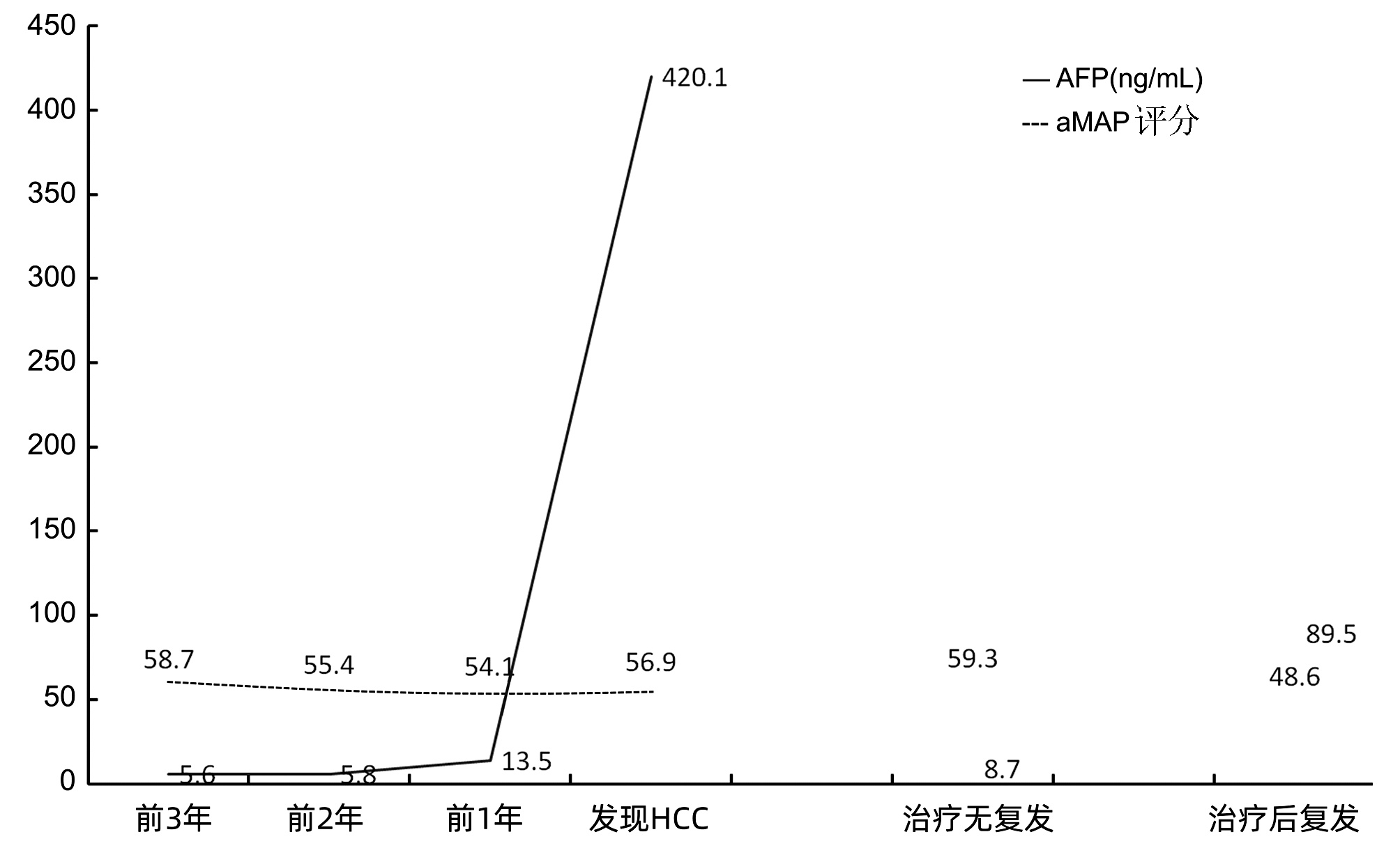
图 1 HCC确诊前3年以及治疗后复发与否的AFP与aMAP变化
Figure 1. AFP and aMAP in HCC patients before diagnosis HCC 3 years and after treatment recurrence or not
表 1 各亚组aMAP评分的高、中、低风险人数分布及比例
Table 1. Distribution and proportion of high, medium and low risk with aMAP score in each subgroup
项目 高风险(n=49) 中风险(n=164) 低风险(n=496) U值 P值 性别[例(%)] -0.42 0.67 男 21(5.0) 105(25.0) 294(75.0) 女 28(9.7) 59(20.4) 202(69.9) 乙型肝炎家族史[例(%)] -0.22 0.83 有 16(5.0) 81(25.2) 224(69.2) 无 33(8.5) 83(21.4) 272(70.1) 肝癌家族史[例(%)] -0.03 0.97 有 11(6.0) 44(19.8) 127(74.0) 无 38(7.2) 120(22.8) 369(70.0) 合并酒精性肝病[例(%)] -4.25 <0.01 有 15(9.4) 55(34.6) 89(56.0) 无 34(6.2) 109(19.8) 407(74.0) 合并糖尿病[例(%)] -2.59 0.01 有 10(11.9) 25(29.8) 49(58.3) 无 39(6.2) 139(22.2) 447(71.5) 合并脂肪肝[例(%)] -0.32 0.74 有 6(4.5) 33(25.0) 93(70.4) 无 43(7.5) 131(22.7) 403(69.8) 合并肝硬化[例(%)] -8.99 <0.01 有 26(19.3) 56(41.5) 53(39.2) 无 23(4.0) 108(18.8) 443(77.2) 合并HCC[例(%)] -4.75 <0.01 有 6(8.7) 33(47.8) 30(43.5) 无 43(6.7) 131(20.5) 466(72.8) 抗病毒治疗[例(%)] -0.33 0.74 有 27(5.4) 124(24.8) 350(69.9) 无 22(10.6) 40(19.2) 146(70.2) ALT[例(%)] -6.02 <0.01 <40 U/L 6(3.0) 22(10.7) 177(86.3) ≥40 U/L 43(8.5) 142(28.2) 319(63.2) HBeAg[例(%)] -5.06 <0.01 阳性 5(3.0) 18(11.0) 141(86.0) 阴性 44(8.1) 146(26.8) 355(65.1) HBV DNA[例(%)] -4.83 <0.01 <30 IU/mL 13(4.2) 52(16.6) 248(79.2) ≥30 IU/mL 36(9.1) 112(28.3) 248(62.6) HBsAg[例(%)] -9.11 <0.01 ≤247 IU/mL 21(3.9) 92(17.3) 420(78.8) >247 IU/mL 28(15.9) 72(40.9) 76(43.2)  下载: 导出CSV
下载: 导出CSV
表 2 HCC患者确诊前1、2、3年的aMAP评分
Table 2. aMAP of HCC patients before diagnosised 1-3 years
组别 例数 高风险[例(%)] 中风险[例(%)] 低风险[例(%)] 诊断HCC前3年 13 5(38.5) 3(23.0) 5(38.5) 诊断HCC前2年 15 4(26.7) 4(26.7) 7(46.7) 诊断HCC前1年 15 5(33.3) 6(40.0) 4(26.7) 诊断HCC时 69 6(8.7) 33(47.8) 30(43.5)
下载: 导出CSV
-
[1] General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer (2022 edition)[J]. J Clin Hepatol, 2022, 38(2): 288-303. DOI: 10.3969/j.issn.1001-5256.2022.02.009.国家卫生健康委办公厅. 原发性肝癌诊疗指南(2022年版)[J]. 临床肝胆病杂志, 2022, 38(2): 288-303. DOI: 10.3969/j.issn.1001-5256.2022.02.009. [2] WANG M, WANG Y, FENG X, et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: Experience of the Chinese National Cancer Center[J]. Int J Infect Dis, 2017, 65: 15-21. DOI: 10.1016/j.ijid.2017.09.003. [3] FAN R, PAPATHEODORIDIS G, SUN J, et al. aMAP risk score predicts hepatocellular carcinoma development in patients with chronic hepatitis[J]. J Hepatol, 2020, 73(6): 1368-1378. DOI: 10.1016/j.jhep.2020.07.025. [4] YANG HI, YUEN MF, CHAN HL, et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and validation of a predictive score[J]. Lancet Oncol, 2011, 12(6): 568-574. DOI: 10.1016/S1470-2045(11)70077-8. [5] WONG VW, CHAN SL, MO F, et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers[J]. J Clin Oncol, 2010, 28(10): 1660-1665. DOI: 10.1200/JCO.2009.26.2675. [6] WONG GL, CHAN HL, WONG CK, et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B[J]. J Hepatol, 2014, 60(2): 339-345. DOI: 10.1016/j.jhep.2013.09.029. [7] PAPATHEODORIDIS G, DALEKOS G, SYPSA V, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy[J]. J Hepatol, 2016, 64(4): 800-806. DOI: 10.1016/j.jhep.2015.11.035. [8] IOANNOU GN, GREEN PK, BESTE LA, et al. Development of models estimating the risk of hepatocellular carcinoma after antiviral treatment for hepatitis C[J]. J Hepatol, 2018, 69(5): 1088-1098. DOI: 10.1016/j.jhep.2018.07.024. [9] IOANNOU GN, GREEN P, KERR KF, et al. Models estimating risk of hepatocellular carcinoma in patients with alcohol or NAFLD-related cirrhosis for risk stratification[J]. J Hepatol, 2019, 71(3): 523-533. DOI: 10.1016/j.jhep.2019.05.008. [10] SHARMA SA, KOWGIER M, HANSEN BE, et al. Toronto HCC risk index: A validated scoring system to predict 10-year risk of HCC in patients with cirrhosis[J]. J Hepatol, 2017. DOI: 10.1016/j.jhep.2017.07.033.[Onlineaheadofprint] [11] Chinese Society of Infectious Diseases, Chinese Medical Association, Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [12] SUK KT, BAIK SK, YOON JH, et al. Revision and update on clinical practice guideline for liver cirrhosis[J]. Korean J Hepatol, 2012, 18(1): 1-21. DOI: 10.3350/kjhep.2012.18.1.1. [13] Fatty Liver Expert Committee, Chinese Medical Doctor Association, National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association. Guidelines of prevention and treatment for alcoholic liver disease: a 2018 update[J]. J Clin Hepatol, 2018, 34(5): 939-946. DOI: 10.3969/j.issn.1001-5256.2018.05.006.中国医师协会脂肪性肝病专家委员会, 中华医学会肝病学分会脂肪肝和酒精性肝病学组. 酒精性肝病防治指南(2018年更新版)[J]. 临床肝胆病杂志, 2018, 34(5): 939-946. DOI: 10.3969/j.issn.1001-5256.2018.05.006. [14] National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association, Fatty Liver Expert Committee, Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease: A 2018 update[J]. J Clin Hepatol, 2018, 34(5): 947-957. DOI: 10.3969/j.issn.1001-5256.2018.05.007.中华医学会肝病学分会脂肪肝和酒精性肝病学组, 中国医师协会脂肪性肝病专家委员会. 非酒精性脂肪性肝病防治指南(2018年更新版)[J]. 临床肝胆病杂志, 2018, 34(5): 947-957. DOI: 10.3969/j.issn.1001-5256.2018.05.007. [15] TSENG TC, LIU CJ, YANG HC, et al. High levels of hepatitis B surface antigen increase risk of hepatocellular carcinoma in patients with low HBV load[J]. Gastroenterology, 2012, 142(5): 1140-1149. e3; quiz e13-e14. DOI: 10.1053/j.gastro.2012.02.007. [16] LI XH, HAO X, DENG YH, et al. Application of aMAP score to assess the risk of hepatocarciongenesis in population of chronic liver disease in primary hospitals[J]. Chin J Hepatol, 2021, 29(4): 332-337. DOI: 10.3760/cma.j.cn501113-20210329-00144.李秀华, 郝新, 邓永红, 等. 应用aMAP评分评估基层医院慢性肝病人群的肝癌发生风险[J]. 中华肝脏病杂志, 2021, 29(4): 332-337. DOI: 10.3760/cma.j.cn501113-20210329-00144. -

 本文二维码
本文二维码
图(1) / 表(2)
计量
- 文章访问数: 527
- HTML全文浏览量: 296
- PDF下载量: 53
- 被引次数: 0

