
 PDF下载 ( 2312 KB)
PDF下载 ( 2312 KB)

超声引导下局部消融治疗危险区域原发性肝癌的效果及安全性分析
DOI: 10.3969/j.issn.1001-5256.2021.07.023
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:王婷负责资料收集,数据分析及文章撰写;陆伟、李嘉、周莉负责课题设计,研究指导,审校并最终定稿;王春妍、刘建勇、周永和负责分析数据,指导文章撰写。
Effectiveness and safety of ultrasound-guided ablation in treatment of primary liver cancer in dangerous areas
-
摘要:
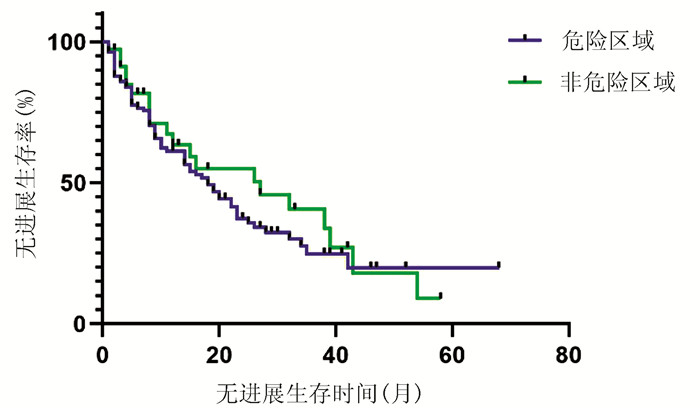
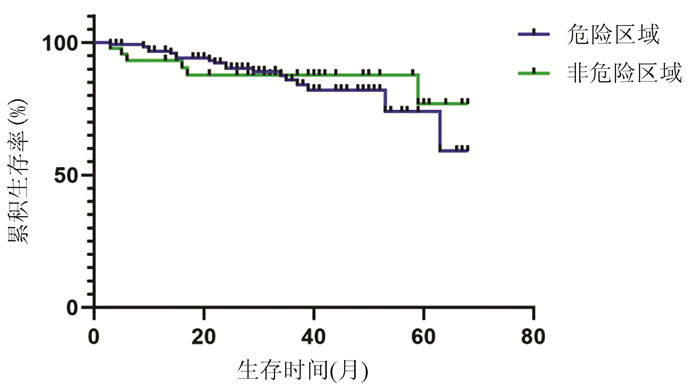
目的 探讨超声引导下经皮局部消融术对危险区域肝癌的治疗效果并评估安全性。 方法 选取2014年1月—2017年9月天津市第二人民医院收治的179例初次行超声引导下消融术治疗的原发性肝癌患者,按肿瘤位置不同分为危险区域组(134例)和非危险区域组(45例),均接受消融治疗。术后对患者肿瘤复发、死亡情况进行随访,无复发或死亡者随访至2019年9月。比较危险区域组和非危险区域组患者消融术后并发症、肿瘤完全缓解情况、肿瘤复发或进展及术后生存情况。符合正态分布的计量资料2组间比较采用两独立样本t检验;非正态分布的计量资料2组间比较采用Mann-Whitney U检验;计数资料2组间比较采用χ2检验。采用Kaplan-Meier法分析肿瘤局部进展率、累积生存率,2组间比较采用log-rank检验。 结果 2组患者基线水平无差异。危险区域组和非危险区域组术后轻度、重度并发症发生率,术后1个月甲胎蛋白(AFP)下降率、复常率差异均无统计学意义(42.5% vs 51.1%、6.0% vs 2.22%、75.0% vs 80.0%和33.9% vs 26.3%,P值均>0.05);术后1个月完全缓解率差异无统计学意义(91.8% vs 93.3%,P=0.990);危险区域组和非危险区域组术后1、2年肿瘤无进展生存率分别为60.7%、63.50%和37.1%、55.0%,中位无进展生存时间分别为18个月和27个月,差异无统计学意义(χ2=0.573,P=0.449);术后1、2年累积生存率分别为96.8%、93.3%和90.3%、87.8%,差异无统计学意义(χ2=0.110,P=0.731)。 结论 超声引导下经皮局部消融术治疗危险区域肝癌可行、安全、有效。 Abstract:Objective To investigate the effectiveness and safety of ultrasound-guided percutaneous local ablation in the treatment of liver cancer in dangerous areas. Methods A total of 179 patients with primary liver cancer who were admitted to Tianjin Second People's Hospital from January 2014 to September 2017 and underwent ultrasound-guided ablation for the first time were enrolled, and according to tumor location, the patients were divided into dangerous area group with 134 patients and non-dangerous area group with 45 patients. All patients received ablation therapy. The patients were followed up to observe tumor recurrence and death, and the patients without recurrence or death were followed up to September 2019. The two groups were compared in terms of complications after ablation, complete tumor response rate, tumor recurrence or progression, and postoperative survival. The two-independent-samples t-test was used for comparison of normally distributed continuous data between two groups; The Mann-Whitney U test was used for comparison of non- normally distributed continuous data between two groups, and the chi-square test was used for comparison of categorical data between two groups; the Kaplan-Meier method was used to analyze local tumor progression rate and cumulative survival rate, and the log-rank test was used for comparison between two groups. Results There were no significant differences in baseline levels between the two groups. There were no significant differences between the dangerous area group and the non-dangerous area group in the incidence rates of mild complications (42.5% vs 51.1%, χ2=1.002, P=0.317) and severe complications (6.0% vs 2.22%, χ2=0.453, P=0.290) and the reduction rate and normalization rate of alpha-fetoprotein within 1 month after ablation (reduction rate: 75.0% vs 80.0%, χ2=0.464, P=0.496; normalization rate: 33.9% vs 26.3%, χ2=0.381, P=0.537), and there was also no significant difference in complete tumor response rate between the two groups (91.8% vs 93.3%, P=0.990). The dangerous area group had 1- and 2-year progression-free survival rates of 60.7% and 37.1%, respectively, and the non-dangerous area group had 1- and 2-year progression-free survival rates of 63.5% and 55.0%, respectively, with a median progression-free survival time of 18 months and 27 months, respectively, and there was no significant difference between the two groups (χ2=0.573, P=0.449). The dangerous area group had 1- and 2-year cumulative survival rates of 96.8% and 90.3%, respectively, and the non-dangerous area group had 1- and 2-year cumulative survival rates of 93.3% and 87.8%, respectively, with no significant difference between the two groups (χ2=0.110, P=0.731). Conclusion Ultrasound-guided percutaneous local ablation is a feasible, safe, and effective method for the treatment of liver cancer in dangerous areas. -
Key words:
- Carcinoma, Hepatocellular /
- Catheter Ablation /
- Treatment Outcome
-
表 1 2组患者一般资料
项目 危险区域组(n=134) 非危险区域组(n=45) 统计值 P值 男性(例) 95 37 χ2=2.232 0.135 年龄(岁) 58.3±10.0 58.3±8.7 t=-0.008 0.994 肿瘤最大直径(cm) 2.3±0.9 2.5±1.0 t=-1.612 0.109 CNLC期(例) χ2=1.000 0.597 Ⅰa期 127 43 Ⅱb期 7 2 Child-Pugh A级(例) χ2=0.208 0.649 A级 114 37 B级 20 8 术前AFP(例) χ2=0.305 0.581 升高 62 19 正常 70 26 ALT(U/L) 24(17~36) 23(18~37) Z=-0.003 0.997 AST(U/L) 27(20~38) 32(22~47) Z=-1.688 0.091 Alb(g/L) 40.6±6.8 41.2±6.9 t=-0.562 0.575 TBil(μmol/L) 16.6(11.8~23.2) 18.7(13.4~25.8) Z=-1.535 0.125 INR 1.10±0.18 1.12±0.19 t=-0.769 0.443  下载: 导出CSV
下载: 导出CSV
表 2 2组患者术后并发症情况比较
并发症 危险区域组(n=134) 非危险区域组(n=45) χ2值 P值 轻度并发症[(例)%] 57(42.5) 23(51.1) 1.002 0.317 肝区疼痛 17(12.7) 12(26.7) 非感染性发热 19(14.2) 5(11.1) 恶心、呕吐 21(15.7) 6(13.3) 重度并发症[(例)%] 8(6.0) 1(2.2) 0.453 0.290 消化道出血 3(2.2) 1(2.2) 术后感染 5(3.7) -
下载: 导出CSV
-
[1] Bureau of Medical AdministrationNational Health Commission of the People's Republic of China. Guidelines for diagnosis and treatment of primary liver cancer in China (2019 edition)[J]. J Clin Hepatol, 2020, 36(2): 277-292. DOI: 10.3969/j.issn.1001-5256.2020.02.007.中华人民共和国国家卫生健康委员会医政医管局. 原发性肝癌诊疗规范(2019年版)[J]. 临床肝胆病杂志, 2020, 36(2): 277-292. DOI: 10.3969/j.issn.1001-5256.2020.02.007. [2] LEE WC, JENG LB, CHEN MF. Estimation of prognosis after hepatectomy for hepatocellular carcinoma[J]. Br J Surg, 2002, 89(3): 311-316. DOI: 10.1046/j.0007-1323.2001.02034.x. [3] Bureau of Medical Administration National Health Commission of the People's Republic of China. Guidelines for diagnosis and treatment of primary liver cancer in China (2019 edition)[J]. J Clin Hepatol, 2020, 36(2): 277-292. DOI: 10.3969/j.issn.1001-5256.2020.02.007.中华人民共和国国家卫生健康委员会医政医管局. 原发性肝癌诊疗规范(2019年版)[J]. 临床肝胆病杂志, 2020, 36(2): 277-292. DOI: 10.3969/j.issn.1001-5256.2020.02.007. [4] TOSHIMORI J, NOUSO K, NAKAMURA S, et al. Local recurrence and complications after percutaneous radiofrequency ablation of hepatocellular carcinoma: A retrospective cohort study focused on tumor location[J]. Acta Med Okayama, 2015, 69(4): 219-226. DOI: 10.18926/AMO/53558. [5] LEE CH, CHEN WT, LIN CC, et al. Radiofrequency ablation assisted by real-time virtual sonography for hepatocellular carcinoma inconspicuous under sonography and high-risk locations[J]. Kaohsiung J Med Sci, 2015, 31(8): 413-419. DOI: 10.1016/j.kjms.2015.06.002. [6] NAKAZAWA T, KOKUBU S, SHIBUYA A, et al. Radiofrequency ablation of hepatocellular carcinoma: Correlation between local tumor progression after ablation and ablative margin[J]. AJR Am J Roentgenol, 2007, 188(2): 480-488. DOI: 10.2214/AJR.05.2079. [7] JIANG C, LIU B, CHEN S, et al. Safety margin after radiofrequency ablation of hepatocellular carcinoma: Precise assessment with a three-dimensional reconstruction technique using CT imaging[J]. Int J Hyperthermia, 2018, 34(8): 1135-1141. DOI: 10.1080/02656736.2017.1411981. [8] Chinese Society of Liver Cancer, Chinese Anti-Cancer Association; Chinese Society of Clinical Oncology, Chinese Anti-Cancer Association; Liver Cancer Study Group, Chinese Society of Hepatology, Chinese Medical Association. Expert consensus on the norms of local ablation therapy for hepatocellular carcinoma[J]. J Clin Hepatol, 2011, 27(3): 236-238, 244. http://lcgdbzz.org/article/id/LCGD201103004中国抗癌协会肝癌专业委员会, 中国抗癌协会临床肿瘤学协作专业委员会, 中华医学会肝病学分会肝癌学组. 肝癌局部消融治疗规范的专家共识[J]. 临床肝胆病杂志, 2011, 27(3): 236-238, 244. http://lcgdbzz.org/article/id/LCGD201103004 [9] LENCIONI R, LLOVET JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma[J]. Semin Liver Dis, 2010, 30(1): 52-60. DOI: 10.1055/s-0030-1247132. [10] BENSON AB 3rd, D'ANGELICA MI, ABBOTT DE, et al. NCCN guidelines insights: Hepatobiliary cancers, version 1.2017[J]. J Natl Compr Canc Netw, 2017, 15(5): 563-573. DOI: 10.6004/jnccn.2017.0059. [11] ZHU P, WANG YM. Updated key points and clinical pathway for NCCN clinical practice guidelines in oncology: Hepatobiliary cancers (Version2. 2016)[J]. J Clin Hepatol, 2016, 32(9): 1644-1652. DOI: 10.3969/j.issn.1001-5256.2016.09.003.朱鹏, 王宇明. 《2016年美国国立综合癌症网络肝胆肿瘤临床实践指南(V2版)》更新要点及临床路径[J]. 临床肝胆病杂志, 2016, 32(9): 1644-1652. DOI: 10.3969/j.issn.1001-5256.2016.09.003. [12] YANG BS, YUAN M, HOU YB, et al. TACE combined with precision radiofrequency ablation by using multiple imaging guidance technology for HCC located at exceptionalsites[J]. J Intervent Radiol, 2018, 27(12): 1193-1198. DOI: 10.3969/j.issn.1008-794X.2018.12.018.杨柏帅, 袁敏, 侯毅斌, 等. TACE联合多影像引导技术精准消融特殊部位肝细胞癌29例[J]. 介入放射学杂志, 2018, 27(12): 1193-1198. DOI: 10.3969/j.issn.1008-794X.2018.12.018. [13] HAN HY, JING X, DING JM, et al. Safety and efficacy of microwave ablation for hepatocellular carcinoma at dangerous locations[J]. Chin J Interv Imaging Ther, 2017, 14(4): 205-209. DOI: 10.13929/j.1672-8475.201611009.韩海云, 经翔, 丁建民, 等. 经皮微波消融治疗危险部位肝癌的安全性和疗效分析[J]. 中国介入影像与治疗学, 2017, 14(4): 205-209. DOI: 10.13929/j.1672-8475.201611009. [14] TERATANI T, YOSHIDA H, SHⅡNA S, et al. Radiofrequency ablation for hepatocellular carcinoma in so-called high-risk locations[J]. Hepatology, 2006, 43(5): 1101-1108. DOI: 10.1002/hep.21164. [15] HUANG H, LIANG P, YU XL, et al. Safety assessment and therapeutic efficacy of percutaneous microwave ablation therapy combined with percutaneous ethanol injection for hepatocellular carcinoma adjacent to the gallbladder[J]. Int J Hyperthermia, 2015, 31(1): 40-47. DOI: 10.3109/02656736.2014.999017. [16] ZHANG M, LIANG P, CHENG ZG, et al. Efficacy and safety of artificial ascites in assisting percutaneous microwave ablation of hepatic tumours adjacent to the gastrointestinal tract[J]. Int J Hyperthermia, 2014, 30(2): 134-141. DOI: 10.3109/02656736.2014.891765. [17] WONG SN, LIN CJ, LIN CC, et al. Combined percutaneous radiofrequency ablation and ethanol injection for hepatocellular carcinoma in high-risk locations[J]. AJR Am J Roentgenol, 2008, 190(3): w187-w195. DOI: 10.2214/AJR.07.2537. [18] LIU A, XU W, XU H, et al. Effects of ultrasound-guided low-power microwave ablation for the treatment of liver cancer in special sites[J]. J Pract Radiol, 2018, 34(12): 1925-1928. DOI: 10.3969/j.issn.1002-1671.2018.12.028.柳昂, 许伟, 徐浩, 等. 超声引导下小功率微波消融术治疗特殊部位肝癌疗效分析[J]. 实用放射学杂志, 2018, 34(12): 1925-1928. DOI: 10.3969/j.issn.1002-1671.2018.12.028. [19] ZHANG NN, CHENG XJ, LIU JY, et al. High-powered microwave ablation in treating patients with hepatocellular carcinoma and the risk fac-tors of recurrence[J]. J Prac Hepatol, 2015, 18(3): 249-253. DOI: 10.3969/j.issn.1672-5069.2015.02.008.张宁宁, 程晓静, 刘建勇, 等. 大功率微波消融治疗肝癌临床疗效及其复发危险因素分析[J]. 实用肝脏病杂志, 2015, 18(3): 249-253. DOI: 10.3969/j.issn.1672-5069.2015.02.008. -

 本文二维码
本文二维码
图(2) / 表(2)
计量
- 文章访问数: 397
- HTML全文浏览量: 119
- PDF下载量: 52
- 被引次数: 0

