
 PDF下载 ( 2613 KB)
PDF下载 ( 2613 KB)

Value of serum autophagy-related protein 7 in diagnosis of HBV-related hepatocellular carcinoma
-
摘要:
目的 通过分析HBV相关肝细胞癌(HBV-HCC)患者血清自噬相关蛋白7(ATG7)的表达水平,探讨其在HBV-HCC诊断中的临床意义。 方法 选取2018年6月—2020年12月在福建医科大学孟超肝胆医院住院的慢性乙型肝炎(CHB)患者50例,HCC患者89例,其中HBV-HCC患者67例,非HBV-HCC(nonHBV-HCC)患者22例,另选取同期20例健康体检者为对照(HC)。采集各组个体人口学及AFP等实验室数据,应用ELISA技术检测各组样本血清ATG7水平,绘制ATG7、AFP及二者联合检测受试者工作特征曲线(ROC曲线)并比较其曲线下面积(AUC)。非正态分布的计量资料多组间比较采用Kruskal-Wallis H检验,2组间比较采用Mann-Whitney U检验;计数资料组间比较采用χ2检验;采用Spearman进行相关性分析。 结果 HBV-HCC组、nonHBV-HCC组、CHB组和HC组的血清ATG7水平分别为22.88(19.79~23.04) ng/mL、17.06(14.45~19.40)ng/mL、19.21(16.65~20.82)ng/mL和13.82(8.70~17.82)ng/mL,差异有统计学意义(χ2=65.144,P<0.001);ATG7诊断HBV-HCC的AUC为0.818(95%CI:0.743~0.879),略高于AFP(AUC=0.777,95%CI:0.698~0.843),差异无统计学意义(Z=0.852,P=0.394);ATG7和AFP联合检测诊断HBV-HCC的AUC为0.859(95%CI:0.790~0.913),显著高于ATG7(Z=2.192,P=0.028)和AFP(Z=2.076,P=0.038)。 结论 ATG7是诊断HBV-HCC的良好标志物,ATG7和AFP联合检测可显著提高HBV-HCC的诊断率。 Abstract:Objective To investigate the clinical significance of autophagy-related protein 7 (ATG7) in the diagnosis of HBV-related hepatocellular carcinoma (HBV-HCC) by measuring the expression level of serum ATG7 in patients with HBV-HCC. Methods A total of 50 patients with chronic hepatitis B (CHB) and 89 patients with HCC who were hospitalized in Mengchao Hepatobiliary Hospital of Fujian Medical University from June 2018 to December 2020 were enrolled, among whom 67 patients had HBV-HCC (HBV-HCC group) and 22 patients had no HBV-HCC (non-HBV-HCC group), and 20 healthy volunteers who underwent physical examination were enrolled as healthy control (HC) group. Demographic data and laboratory data including alpha-fetoprotein (AFP) were collected from each group, and ELISA was used to measure the serum level of ATG7. The receiver operating curve (ROC) was plotted for ATG7 and AFP used alone or in combination, and the area under the ROC curve (AUC) was compared. The Kruskal-Wallis H test was used for comparison of non-normally distributed continuous data between multiple groups, and the Mann-Whitney U test was used for comparison between two groups; the chi-square test was used for comparison of categorical data between groups; a Spearman correlation analysis was used to investigate correlation. Results The serum level of ATG7 was 22.88(19.79-23.04) ng/mL in the HBV-HCC group, 17.06(14.45-19.40) ng/mL in the non-HBV-HCC group, 19.21(16.65-20.82) ng/mL in the CHB group, and 13.82(8.70-17.82) ng/mL in the HC group, with a significant difference between groups (χ2=65.144, P < 0.001). ATG7 had an AUC of 0.818 (95% confidence interval [CI]: 0.743-0.879) and AFP had an AUC of 0.777 (95% CI: 0.698-0.843) in the diagnosis of HBV-HCC, suggesting that ATG7 had a slightly higher AUC than AFP (Z=0.852, P=0.394). ATG7 combined with AFP had an AUC of 0.859 (95% CI: 0.790-0.913) in the diagnosis of HBV-HCC, which was significantly higher than the AUC of ATG7 alone (Z=2.192, P=0.028) and AFP alone (Z=2.076, P=0.038). Conclusion ATG7 is a good marker for the diagnosis of HBV-HCC, and combined measurement of ATG7 and AFP can significantly improve the diagnostic rate for HBV-HCC. -
肝细胞癌(HCC)是我国最常见的恶性肿瘤之一。国家癌症中心最新数据显示,我国每年新发肝癌约37万人,约32.6万人死于肝癌,其中94.7%与慢性HBV感染有关[1-2]。早期发现、早期诊断和早期治疗是改善原发性肝癌预后的关键。然而目前尚缺乏原发性肝癌高敏感度和高特异度的诊断指标。自噬是细胞自我吞噬胞内长寿蛋白或受损细胞器并通过溶酶体途径进行的分解代谢过程,从而维持细胞稳态[3]。近年研究[4-7]显示自噬在HBV感染和HCC的发生发展起重要作用。但目前关于自噬相关蛋白在HBV相关HCC(HBV-HCC)患者血清中的表达及意义鲜有报道。本研究通过分析HBV-HCC、非HBV相关HCC(nonHBV-HCC)、慢性乙型肝炎(CHB)和健康对照者血清自噬相关蛋白7(ATG7)的表达水平,探讨ATG7对HBV-HCC的诊断价值。
1. 资料与方法
1.1 研究对象
选取2018年6月—2020年12月于本院住院的HCC患者89例。HCC的诊断标准符合《原发性肝癌诊疗规范(2017年版)》[8]并经病理确认。排除标准如下:病理类型为肝内胆管癌或HCC-肝内胆管癌混合型者;已接受过肝移植术、局部消融、肝动脉化疗栓塞术、放化疗等抗肿瘤治疗者;继发性HCC患者;同时伴有其他肿瘤患者。CHB诊断符合《慢性乙型肝炎防治指南(2019年版)》[9]。根据血清是否检出HBsAg和/或HBV DNA分为HBV-HCC组及nonHBV-HCC组。选取同期50例CHB患者(CHB组)和20例健康体检者作为对照组(HC组)。
1.2 资料收集
收集研究对象性别和年龄,总蛋白(TP)、白蛋白(Alb)、TBil、DBil、ALT、AST、GGT和ALP等实验室指标。另收集HBV-HCC组患者的BCLC分期和肿瘤直径等病理资料。
1.3 血清ATG7检测
所有研究对象清晨空腹肘静脉采血,采血后1 h内送实验室,3000 r/min离心10 min分离血清,-80 ℃冰箱保存。ATG7检测前4 h室温下复溶。使用上海江莱生物技术有限公司人ATG7酶联免疫吸附测定试剂盒(批号:Aug 2020)进行检测,严格按试剂盒说明书操作,在加入终止液15 min内用PHOMO酶标仪(安图生物,合肥)在450 nm波长测定各孔光密度(OD值),用WPS表格以标准品的浓度为纵坐标,OD值为横坐标绘制标准曲线并取得多项式公式,根据多项式公式计算每个样本的ATG7浓度。
1.4 伦理学审查
本研究方案经由福建医科大学孟超肝胆医院伦理委员会审批,批号:科审2020-029-01。
1.5 统计学方法
采用SPSS 22.0进行统计分析。非正态分布的计量资料以M(P25~P75)表示,多组间比较采用Kruskal-Wallis H检验,2组间比较采用Mann-Whitney U检验;计数资料组间比较采用χ2检验;采用Spearman进行相关性分析。运用GraphPad Prism7.0绘制散点图,采用Medcalc18.11.3绘制受试者工作特征曲线(ROC曲线)并比较不同指标曲线下面积(AUC)。P<0.05为差异有统计学意义。
2. 结果
2.1 一般资料
HCC、CHB及HC 3组比较,男女比例差异无统计学意义,其余指标差异均有统计学意义(P值均<0.01)(表 1)。89例HCC患者中,67例(75.28%)血清HBsAg和/或HBV DNA阳性,纳入HBV-HCC组;剩余22例(24.72%)纳入nonHBV-HCC组,包括5例酒精性肝硬化,8例非酒精性脂肪肝,1例慢性丙型肝炎,2例肝硬化(病因未明),6例慢性肝炎(病因未明)。HBV-HCC组血清TBil水平及具有肝硬化背景病例数高于nonHBV-HCC组,而nonHBV-HCC组的血清AST水平和最大肿瘤直径高于HBV-HCC组,差异均有统计学意义(P值均<0.05),其余参数差异均无统计学意义(P值均>0.05)(表 2)。
表 1 3组人口学和实验室特征比较参数 HCC组(n=89) CHB组(n=50) HC组(n=20) χ2值 P值 年龄(岁) 56.0(48.0~66.5) 42.0(32.8~52.5) 37.5(30.0~48.8) 38.807 <0.001 男性[例(%)] 77(86.52) 38(76.00) 13(65.00) 5.480 0.076 TBil(μmol/L) 19.30(12.65~26.10) 19.55(12.78~29.28) 12.15(9.48~18.63) 10.478 0.005 DBil(μmol/L) 7.60(4.70~10.85) 4.45(2.20~7.05) 5.30(4.15~6.35) 17.168 <0.001 TP(g/L) 61.0(54.5~67.5) 66.5(60.8~73.3) 72.0(70.0~77.0) 34.168 <0.001 Alb(g/L) 34.0(31.0~38.5) 37.5(34.0~41.0) 44.0(41.0~47.0) 42.516 <0.001 ALT(U/L) 115.0(62.0~218.5) 87.5(26.5~206.8) 19.0(12.3~26.5) 37.212 <0.001 AST(U/L) 149.0(54.0~286.0) 57.0(31.5~110.5) 17.0(14.3~20.0) 54.345 <0.001 GGT(U/L) 52.0(34.0~110.5) 68.5(29.3~112.0) 17.0(14.3~24.5) 31.527 <0.001 ALP(U/L) 81.0(60.5~103.0) 102.0(82.5~117.0) 66.5(52.8~88.3) 21.160 <0.001 AFP(ng/mL) 37.90(5.00~712.32) 7.20(3.05~241.27) 2.85(2.18~4.48) 33.048 <0.001 ATG7(ng/mL) 21.11(17.76~22.73) 19.21(16.65~20.82) 13.82(8.70~17.82) 33.134 <0.001 表 2 HBV-HCC组与nonHBV-HCC组生化和病理特征比较参数 HBV-HCC组(n=67) nonHBV-HCC组(n=22) 统计值 P值 年龄(岁) 55.0(46.0~ 65.0) 63.5(50.8~71.8) U=535.000 0.055 男/女(例) 58/9 19/3 χ2=0.001 0.981 TBil(μmol/L) 20.60(13.30~27.40) 16.00(11.15~21.48) U=524.500 0.043 DBil(μmol/L) 7.70(4.80~10.90) 7.15(3.80~9.65) U=602.500 0.201 TP(g/L) 61.0(50.0~67.0) 58.5(51.3~68.3) U=638.500 0.348 Alb(g/L) 34.0(31.0~38.0) 33.0(30.3~39.0) U=709.500 0.793 ALT(U/L) 95.0(54.0~198.0) 152.0(89.8~268.0) U=557.000 0.087 AST(U/L) 136.0(37.0~240.0) 236.5(93.8~348.8) U=523.000 0.042 GGT(U/L) 51.0(30.0~111.0) 58.0(35.0~113.3) U=658.000 0.452 ALP(U/L) 76.0(60.0~99.0) 92.0(62.8~127.8) U=575.500 0.124 AFP(ng/mL) 58.00(7.10~945.80) 18.28(2.48~405.33) U=536.500 0.057 BCLC(A/B/C/D,例) 51/4/12/0 12/5/5/0 χ2=5.229 0.073 最大肿瘤直径(cm) 3.95(2.50~7.70) 8.00(3.70~11.00) U=520.000 0.047 肝硬化[例(%)] 55(82.09) 9(40.91) χ2=13.904 <0.001 2.2 HBV-HCC血清ATG7表达水平升高
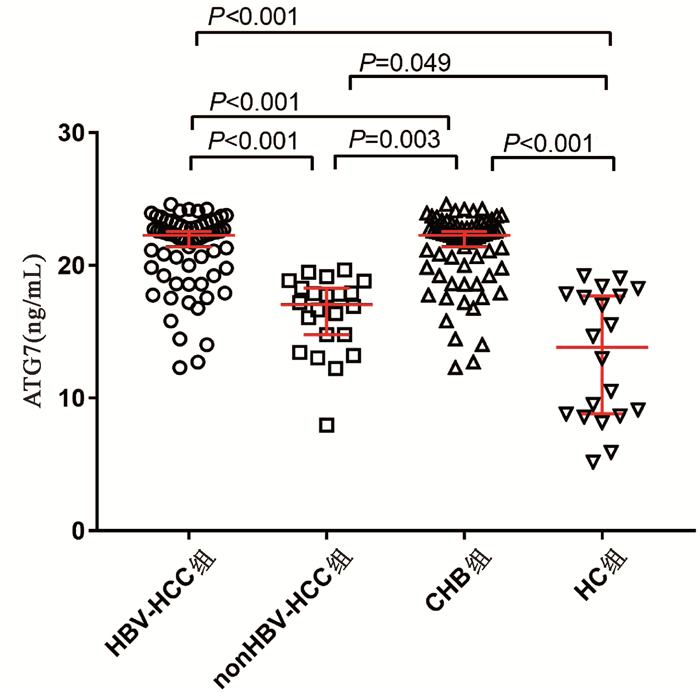
HBV- HCC组、nonHBV-HCC组、CHB组和HC组血清ATG7水平分别为22.88(19.79~23.04)ng/mL、17.06(14.45~19.40)ng/mL、19.21(16.65~20.82)ng/mL和13.82(8.70~17.82)ng/mL,差异有统计学意义(χ2=65.144,P<0.001)。两两比较显示HBV-HCC组血清ATG7不仅高于CHB组(U=758.5,P<0.001)和HC组(U=94.0,P<0.001),也高于nonHBV-HCC组(U=142.0,P<0.001);而nonHBV-HCC组血清ATG7水平不仅低于HBV-HCC组,也低于CHB组(U=311.0,P=0.003),仅稍高于HC组(U=142.0,P=0.049)(图 1)。此外,在67例HBV-HCC患者中,有肝硬化背景和无肝硬化背景患者的血清ATG7水平分别为22.32 (19.79~22.99)ng/mL和20.89(19.40~23.37)ng/mL,差异无统计学意义(P>0.05)。
2.3 血清ATG7表达水平和血清AFP水平的相关性
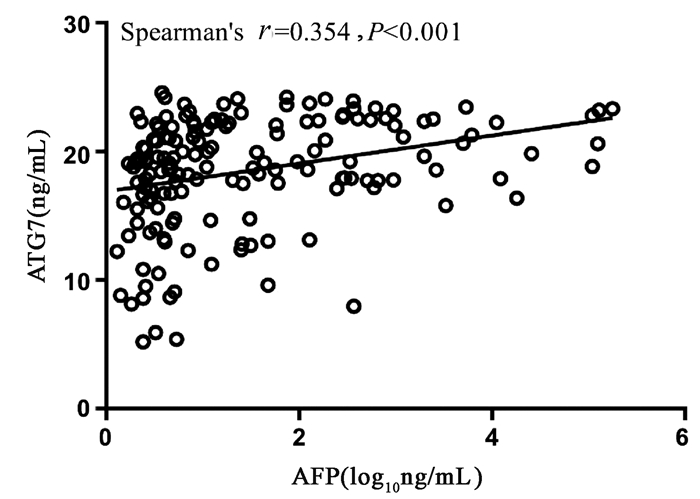
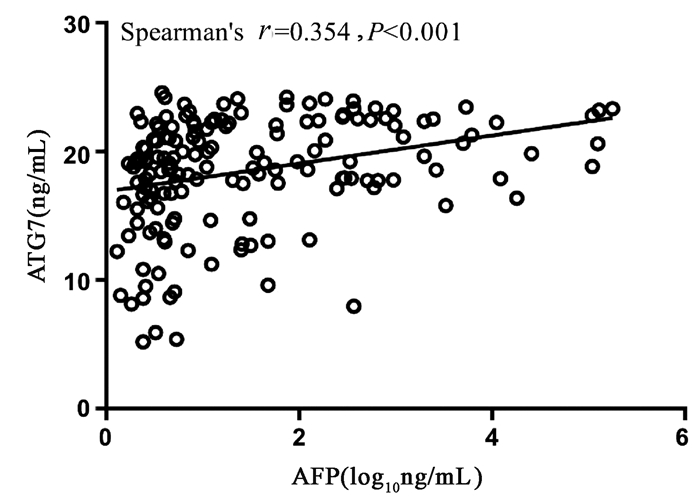
Spearman相关性分析显示,血清ATG7表达水平和血清AFP水平呈正相关,但相关性较弱(r=0.354,95%CI:0.205~0.486,P<0.001)(图 2)。
2.4 ATG7在HBV-HCC中的诊断性能
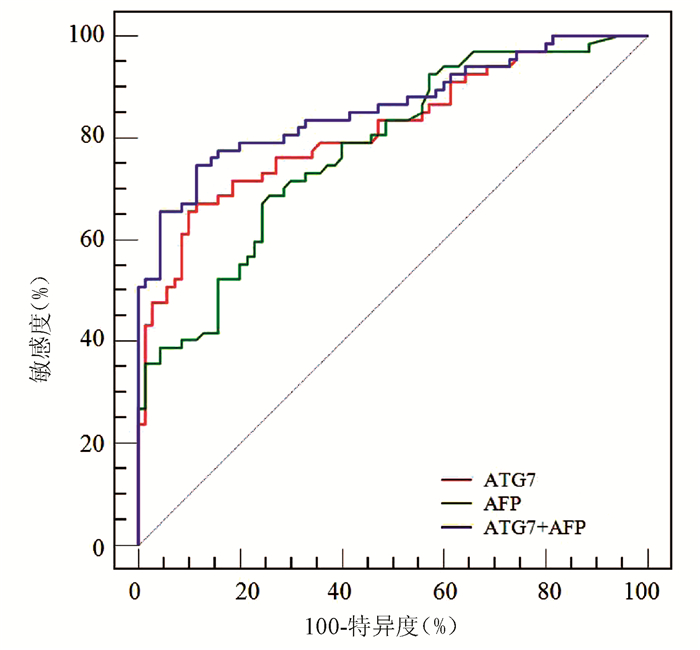
ROC曲线分析显示,ATG7诊断HBV-HCC的AUC为0.818(95% CI:0.743~0.879),稍高于AFP(AUC=0.777,95%CI:0.698~0.843),但二者差异无统计学意义(Z=0.852,P=0.394)(图 3);ATG7诊断HBV-HCC的cut-off值为20.08 ng/mL,敏感度和特异度分别为71.64%和77.14%,均略高于AFP(68.66%和74.29%)。ATG7联合AFP的二元logistic回归预测概率的AUC为0.859 (95%CI:0.790~0.913),显著高于ATG7(Z=2.192,P=0.028)和AFP(Z=2.076,P=0.038)(图 3, 表 3)。
表 3 ATG7、AFP及其联合检测诊断HBV-HCC的性能项目 AUC cut-off值 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) AFP 0.777 12.20 ng/mL 68.66 74.29 71.9 71.2 ATG7 0.818 20.08 ng/mL 71.64 77.14 75.0 74.0 ATG7+AFP 0.859 0.56 74.63 88.57 86.2 78.5 3. 讨论
本研究通过ELISA技术检测HCC患者血清ATG7表达水平,结果显示HBV-HCC患者血清ATG7显著升高,血清ATG7是诊断HBV-HCC的良好标志物,ATG7与AFP联合诊断可显著提高HBV-HCC的诊断效率。
ATG7作为一种泛素样修饰物激活酶,通过激活ATG8和ATG12调节自噬体的延伸,是自噬体形成过程的关键蛋白之一[10]。近年研究[11-12]提示ATG7及自噬在HBV-HCC发生发展中发挥重要作用。首先,HBV感染或HBV病毒蛋白的表达可诱导ATG7表达及自噬反应。本研究中CHB组血清ATG7显著高于健康对照组,印证了自噬与HBV感染有关。其次,多项研究[13-14]显示包括ATG7在内的多种自噬相关蛋白在HCC组织表达显著提高。近年的分子细胞学试验进一步揭示多种分子可通过ATG7调节自噬促进HCC发生发展[15-17]。研究[15]显示长链非编码RNA HOX转录反义RNA(HOTAIR)可通过上调ATG7表达激活自噬促进HCC细胞系增殖。癌性锚蛋白重复序列可直接与胞质中的ATG7蛋白相互作用诱导自噬从而促进HCC细胞进展[16]。肿瘤坏死因子α诱导蛋白8(TNFAIP8)则通过与ATG3-ATG7复合物相互作用调节自噬促进HCC细胞增殖[17]。相反,靶向敲减ATG7可抑制自噬,从而促进细胞凋亡、延缓细胞周期及抑制HCC细胞增殖[13]。上述研究结果表明ATG7与HBV-HCC密切相关。本研究数据显示HBV-HCC患者血清ATG7显著高于CHB和健康对照组,进一步证实了自噬与HBV-HCC的相关性,提示血清ATG7是一种潜在HBV-HCC标志物。而且HBV-HCC患者血清ATG7也显著高于nonHBV-HCC,提示不同病因的HCC发病机制不同,其血清标志物也可不同。
虽然AFP已在临床应用数十年,但诊断敏感度不高。最近的一项系统综述[18]显示,AFP诊断HCC的合并敏感度仅为63.9%。与此相符,本研究中AFP诊断HBV-HCC的敏感度、特异度和AUC分别为68.66%、74.29%和0.777。虽然ATG7的敏感度与AFP相仿,但其特异度较高,总体诊断性能较好。此外,ATG7和AFP相关性较弱,提示二者联合检测可有效提高诊断性能。早前有学者[19]提出应用logistic回归分析有助于提高多指标联合诊断效率。本研究结果显示ATG7联合AFP的二元logistic回归预测模型对HBV-HCC的整体诊断性能较好,AUC及诊断敏感度和特异度均显著高于ATG7及AFP。
总之,本研究显示ATG7是HBV-HCC的良好标志物,与AFP有较好的互补性,二者联合检测可显著提高HBV-HCC的诊断效率。然而本研究为单中心横断面研究,纳入研究病例有限,因此其诊断性能仍有待进一步扩大样本的多中心临床验证。
-
表 1 3组人口学和实验室特征比较
参数 HCC组(n=89) CHB组(n=50) HC组(n=20) χ2值 P值 年龄(岁) 56.0(48.0~66.5) 42.0(32.8~52.5) 37.5(30.0~48.8) 38.807 <0.001 男性[例(%)] 77(86.52) 38(76.00) 13(65.00) 5.480 0.076 TBil(μmol/L) 19.30(12.65~26.10) 19.55(12.78~29.28) 12.15(9.48~18.63) 10.478 0.005 DBil(μmol/L) 7.60(4.70~10.85) 4.45(2.20~7.05) 5.30(4.15~6.35) 17.168 <0.001 TP(g/L) 61.0(54.5~67.5) 66.5(60.8~73.3) 72.0(70.0~77.0) 34.168 <0.001 Alb(g/L) 34.0(31.0~38.5) 37.5(34.0~41.0) 44.0(41.0~47.0) 42.516 <0.001 ALT(U/L) 115.0(62.0~218.5) 87.5(26.5~206.8) 19.0(12.3~26.5) 37.212 <0.001 AST(U/L) 149.0(54.0~286.0) 57.0(31.5~110.5) 17.0(14.3~20.0) 54.345 <0.001 GGT(U/L) 52.0(34.0~110.5) 68.5(29.3~112.0) 17.0(14.3~24.5) 31.527 <0.001 ALP(U/L) 81.0(60.5~103.0) 102.0(82.5~117.0) 66.5(52.8~88.3) 21.160 <0.001 AFP(ng/mL) 37.90(5.00~712.32) 7.20(3.05~241.27) 2.85(2.18~4.48) 33.048 <0.001 ATG7(ng/mL) 21.11(17.76~22.73) 19.21(16.65~20.82) 13.82(8.70~17.82) 33.134 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 HBV-HCC组与nonHBV-HCC组生化和病理特征比较
参数 HBV-HCC组(n=67) nonHBV-HCC组(n=22) 统计值 P值 年龄(岁) 55.0(46.0~ 65.0) 63.5(50.8~71.8) U=535.000 0.055 男/女(例) 58/9 19/3 χ2=0.001 0.981 TBil(μmol/L) 20.60(13.30~27.40) 16.00(11.15~21.48) U=524.500 0.043 DBil(μmol/L) 7.70(4.80~10.90) 7.15(3.80~9.65) U=602.500 0.201 TP(g/L) 61.0(50.0~67.0) 58.5(51.3~68.3) U=638.500 0.348 Alb(g/L) 34.0(31.0~38.0) 33.0(30.3~39.0) U=709.500 0.793 ALT(U/L) 95.0(54.0~198.0) 152.0(89.8~268.0) U=557.000 0.087 AST(U/L) 136.0(37.0~240.0) 236.5(93.8~348.8) U=523.000 0.042 GGT(U/L) 51.0(30.0~111.0) 58.0(35.0~113.3) U=658.000 0.452 ALP(U/L) 76.0(60.0~99.0) 92.0(62.8~127.8) U=575.500 0.124 AFP(ng/mL) 58.00(7.10~945.80) 18.28(2.48~405.33) U=536.500 0.057 BCLC(A/B/C/D,例) 51/4/12/0 12/5/5/0 χ2=5.229 0.073 最大肿瘤直径(cm) 3.95(2.50~7.70) 8.00(3.70~11.00) U=520.000 0.047 肝硬化[例(%)] 55(82.09) 9(40.91) χ2=13.904 <0.001
下载: 导出CSV
表 3 ATG7、AFP及其联合检测诊断HBV-HCC的性能
项目 AUC cut-off值 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) AFP 0.777 12.20 ng/mL 68.66 74.29 71.9 71.2 ATG7 0.818 20.08 ng/mL 71.64 77.14 75.0 74.0 ATG7+AFP 0.859 0.56 74.63 88.57 86.2 78.5
下载: 导出CSV
-
[1] ZHENG RS, SUN KX, ZHANG SW, et al. Report of cancer epidemiology in China, 2015[J]. Chin J Oncol, 2019, 41(1): 19-28. DOI: 10.3760/cma.j.issn.0253-3766.2019.01.005.郑荣寿, 孙可欣, 张四维, 等. 2015年中国恶性肿瘤流行情况分析[J]. 中华肿瘤杂志, 2019, 41(1): 19-28. DOI: 10.3760/cma.j.issn.0253-3766.2019.01.005. [2] WANG M, WANG Y, FENG X, et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: Experience of the Chinese National Cancer Center[J]. Int J Infect Dis, 2017, 65: 15-21. DOI: 10.1016/j.ijid.2017.09.003. [3] SHIN GC, KANG HS, LEE AR, et al. Hepatitis B virus-triggered autophagy targets TNFRSF10B/death receptor 5 for degradation to limit TNFSF10/TRAIL response[J]. Autophagy, 2016, 12(12): 2451-2466. DOI: 10.1080/15548627.2016.1239002. [4] TIAN Y, SIR D, KUO CF, et al. Autophagy required for hepatitis B virus replication in transgenic mice[J]. J Virol, 2011, 85(24): 13453-13456. DOI: 10.1128/JVI.06064-11. [5] AKKOÇ Y, GÖZVAÇ1K D. Autophagy and liver cancer[J]. Turk J Gastroenterol, 2018, 29(3): 270-282. DOI: 10.5152/tjg.2018.150318. [6] XIE M, YANG Z, LIU Y, et al. The role of HBV-induced autophagy in HBV replication and HBV related-HCC[J]. Life Sci, 2018, 205: 107-112. DOI: 10.1016/j.lfs.2018.04.051. [7] WANG YL, XU XY, YU XH, et al. Role of oxidative stress and autophagy in the development an progression of hepatocellular carcinoma[J]. J Clin Hepatol, 2020, 36(2): 426-429. DOI: 10.3969/j.issn.1001-5256.2020.02.042.王雨露, 许笑阳, 俞晓菡, 等. 氧化应激与自噬在肝细胞癌发生发展中的作用[J]. 临床肝胆病杂志, 2020, 36(2): 426-429. DOI: 10.3969/j.issn.1001-5256.2020.02.042. [8] National Health and Family Planning Commission of the People's Republic of China. Diagnosis, management, and treatment of hepatocellular carcinoma (V2017)[J]. J Clin Hepatol, 2017, 33(8): 1419-1431. DOI: 10.3969/j.issn.1001-5256.2017.08.003.中华人民共和国国家卫生和计划生育委员会. 原发性肝癌诊疗规范(2017版)[J]. 临床肝胆病杂志, 2017, 33(8): 1419-1431. DOI: 10.3969/j.issn.1001-5256.2017.08.003. [9] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [10] MIZUSHIMA N, YOSHIMORI T, OHSUMI Y. The role of Atg proteins in autophagosome formation[J]. Annu Rev Cell Dev Biol, 2011, 27: 107-132. DOI: 10.1146/annurev-cellbio-092910-154005. [11] SIR D, TIAN Y, CHEN WL, et al. The early autophagic pathway is activated by hepatitis B virus and required for viral DNA replication[J]. Proc Natl Acad Sci U S A, 2010, 107(9): 4383-4388. DOI: 10.1073/pnas.0911373107. [12] WANG Y, CHE Y, GAO YX, et al. Effect of expression of autophagy related gene Atg7 on replication of hepatitis B virus[J]. China Medical Herald, 2020, 17(2): 4-8. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202002002.htm王阳, 车阳, 高玉雪, 等. 自噬相关蛋白基因Atg7的表达对乙型肝炎病毒复制的影响[J]. 中国医药导报, 2020, 17(2): 4-8. https://www.cnki.com.cn/Article/CJFDTOTAL-YYCY202002002.htm [13] OU Y, HE J, LIU Y. MiR-490-3p inhibits autophagy via targeting ATG7 in hepatocellular carcinoma[J]. IUBMB Life, 2018, 70(6): 468-478. DOI: 10.1002/iub.1715. [14] YU H, LIU QH, XIAO PL, et al. Expression and clinical significance of Beclin1, LC3 and mTOR in hepatic carcinioma[J]. Anhui Med Pharmaceut J, 2018, 22(2): 246-249. DOI: 10.3969/j.issn.1009-6469.2018.02.014.于海, 刘清华, 肖培伦, 等. Beclin1、LC3和mTOR在肝癌中的表达及临床意义[J]. 安徽医药, 2018, 22(2): 246-249. DOI: 10.3969/j.issn.1009-6469.2018.02.014. [15] YANG L, ZHANG X, LI H, et al. The long noncoding RNA HOTAIR activates autophagy by upregulating ATG3 and ATG7 in hepatocellular carcinoma[J]. Mol Biosyst, 2016, 12(8): 2605-2612. DOI: 10.1039/c6mb00114a. [16] LUO T, FU J, XU A, et al. PSMD10/gankyrin induces autophagy to promote tumor progression through cytoplasmic interaction with ATG7 and nuclear transactivation of ATG7 expression[J]. Autophagy, 2016, 12(8): 1355-1371. DOI: 10.1080/15548627.2015.1034405. [17] NITURE S, GYAMFI MA, LIN M, et al. TNFAIP8 regulates autophagy, cell steatosis, and promotes hepatocellular carcinoma cell proliferation[J]. Cell Death Dis, 2020, 113(3): 178. DOI: 1038/s41419-020-2369-4. [18] SUN T, TANG Y, SUN D, et al. Osteopontin versus alpha-fetoprotein as a diagnostic marker for hepatocellular carcinoma: A meta-analysis[J]. Onco Targets Ther, 2018, 11: 8925-8935. DOI: 10.2147/OTT.S186230. [19] QUN ZJ, SHEN Y, CUI XL, et al. Application of logistic regression in multi-index combined diagnosis of diseases[J]. Chin J Health Statistics, 2014, 31(1): 116-118. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT201401036.htm秦正积, 沈毅, 崔晓莉, 等. logistic回归在疾病多指标联合诊断中的应用[J]. 中国卫生统计, 2014, 31(1): 116-118. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT201401036.htm 期刊类型引用(2)
1. 郭佳佳,张文果,王文秀,张晓丽,马徜徉. 血清Nox2、ATG7水平对新生儿窒息心肌损伤的评估价值. 安徽医药. 2024(09): 1791-1795 .  百度学术
百度学术2. 蔡卓玮,胡刚峰,章波. miR-203在乙型肝炎病毒相关肝细胞癌诊断及预后中的意义. 广西医科大学学报. 2022(11): 1773-1780 . 百度学术其他类型引用(0)
-

 下载:
下载:

 百度学术
百度学术 本文二维码
本文二维码

计量
- 文章访问数: 649
- HTML全文浏览量: 130
- PDF下载量: 42
- 被引次数: 2

