
 PDF下载 ( 2595 KB)
PDF下载 ( 2595 KB)

再次肝切除术与射频消融治疗亚洲复发性肝细胞癌患者效果比较的Meta分析
DOI: 10.3969/j.issn.1001-5256.2021.05.025
Clinical effect of re-hepatic resection versus radiofrequency ablation in treatment of recurrent hepatocellular carcinoma in Asia: A Meta-analysis
-
摘要:
目的 使用Meta分析的方法比较再次肝切除术与射频消融治疗亚洲复发性肝癌患者的安全性与疗效。 方法 系统检索PubMed、中国知网和万方数据库,日期自建库截止至2020年6月15日。由两位评价者独立检索并提取数据,采用RevMan 5.4.1软件进行Meta分析。 结果 共2项随机对照试验和18项回顾性队列研究符合纳入标准,均来自亚洲国家,包含2903例复发性肝癌患者。再次肝切除术组和射频消融组患者围手术期病死率分别为2%和0,围手术期并发症发生率分别为22.4%和3.3%。再次肝切除术组和射频消融组患者术后1、3、5年总生存率分别为92.3%、66.3%、51.1%和91.4%、69.2%、39.9%。两组患者术后1、3、5年无瘤生存率分别为67.9%、48.3%、34.4%和57.5%、27.9%、14.0%。Meta分析结果提示,两组患者的总生存率差异无统计学意义(HR=0.89,95%CI:0.77~1.02,P=0.10),但再次肝切除术组患者的无瘤生存率显著高于射频消融组(HR=0.79,95%CI:0.72~0.87,P<0.001)。 结论 目前证据显示,再次肝切除术治疗复发性肝癌有更高的无瘤生存率,但两组患者的总生存率相似。 -
关键词:
- 癌,肝细胞 /
- 肝切除术 /
- 射频消融 /
- Meta分析(主题)
Abstract:Objective To investigate the safety and efficacy of re-hepatic resection (rHR) versus radiofrequency ablation (RFA) in the treatment of recurrent hepatocellular carcinoma (RHCC) in Asia through a meta-analysis. Methods PubMed, CNKI, and Wanfang Data were searched for related studies published up to June 15, 2020. Two reviewers independently searched for the articles and extracted related data, and RevMan 5.4.1 was used to perform the meta-analysis. Results A total of 2 randomized controlled trials and 18 retrospective cohort studies met the inclusion criteria and involved 2903 patients with RHCC from Asian countries. The mortality rate in the perioperative period was 2% in the rHR group and 0 in the RFA group, and the incidence rate of perioperative complications was 22.4% in the rHR group and 3.3% in the RFA group. The 1-, 3-, and 5-year overall survival rates were 92.3%, 66.3%, and 51.1%, respectively, in the rHR group and 91.4%, 69.2%, and 39.9%, respectively, in the RFA group. The 1-, 3-, and 5-year disease-free survival rates were 67.9%, 48.3%, and 34.4%, respectively, in the rHR group and 57.5%, 27.9%, and 14.0%, respectively, in the RFA group. The Meta-analysis showed that there was no significant difference in overall survival rate between the two groups (hazard ratio [HR]=0.89, 95% confidence interval [CI]: 0.77-1.02, P=0.10), while the rHR group had a significantly higher disease-free survival rate than the RFA group (HR=0.79, 95% CI: 0.72-0.87, P < 0.001). Conclusion Current evidence shows that rHR may help to achieve a higher disease-free survival rate than RFA in the treatment of RHCC, while rHR and RFA have a similar overall survival rate. -
肝细胞癌(简称肝癌)术后复发是导致患者死亡的主要原因[1]。对于复发性肝癌,临床上常用的治疗方法包括再次肝切除术、射频消融(radiofrequency ablation,RFA)、肝移植、介入、靶向药物治疗等[2]。然而,目前国内外肝癌诊疗指南均未对复发性肝癌提供具体的诊疗推荐。再次肝切除术和RFA属于根治性治疗方法,临床应用广泛,文献报道较多。但单个研究样本量小,且研究间的结论不统一,临床上对复发性肝癌的根治性治疗方案尚存争议。本文使用Meta分析的方法,客观分析两种治疗措施对复发性肝癌的疗效与安全性。
1. 资料与方法
1.1 文献检索
系统检索PubMed、中国知网和万方数据库,检索日期自建库至2020年6月15日。英文检索词包括:recurrent、recurrence、hepatocellular carcinoma、liver cancer、hepatic resection、hepatectomy、resection、radiofrequency ablation等,中文检索词包括:复发、肝癌、肝细胞癌、手术、再次肝切除术、射频消融等。
1.2 纳入标准
(1) 研究:比较再次肝切除术与RFA治疗复发性肝癌的随机对照试验或队列研究,英文或中文发表。(2)患者:罹患原发性肝癌,接受首次肝切除术治疗后,肝癌复发,复发肿瘤符合米兰标准,且无大血管侵犯及肝外转移。(3)干预措施:肝癌复发后,接受再次肝切除术或RFA治疗。(4)结局指标:报道了总生存期(overall survival,OS)、无瘤生存期(recurrence-free survival,RFS)、围手术期并发症和围手术期病死率中的任何一项。
1.3 排除标准
(1) 肝切除和RFA治疗原发性肝癌、胆管细胞癌或转移性肝癌的研究;(2)单组样本量过小(<10例)或单臂研究;(3)未提供病例具体纳入时间段的研究;(4)肝癌复发后,接受再次肝切除术或RFA治疗前,接受其他的治疗方案(如介入、靶向药物等)。再次肝切除术或RFA治疗后,序贯介入或其他治疗措施,不在排除标准范围之内。对于重复性发表的研究,仅纳入样本量最大的一项。
1.4 数据提取
两位评价者独立检索并提取纳入文献的数据,数据提取过程中若有分歧则通过双方讨论或询问第3位评价者解决。提取的数据包括人口统计学资料及临床基线数据、OS、RFS、围手术期并发症发生率及病死率。若原始文献未详细描述生存数据,则从其Kaplan-Meier生存曲线图估算。
1.5 统计学方法
统计分析采用RevMan 5.4.1软件(Cochrane协作组,牛津,英国)。采用从纳入文献提取的风险比(HR)进行OS和RFS的Meta分析。统计学异质性的评估采用I2检验。I2≥50%时采用随机效应模型,I2<50%时采用固定效应模型。P<0.05为差异有统计学意义。采用漏斗图估计发表偏倚。由于纳入文献提供的数据存在一定的局限性,无法根据患者性别、肿瘤大小、肿瘤个数、肿瘤位置等进行亚组分析。
2. 结果
2.1 基线特点
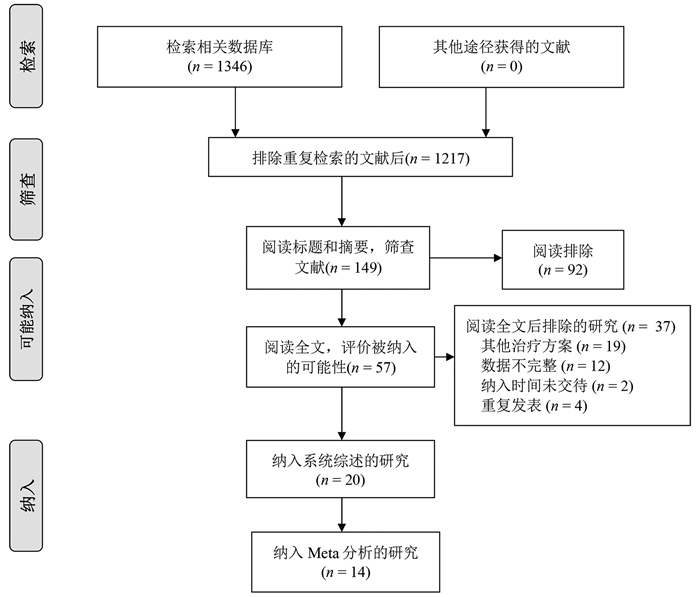
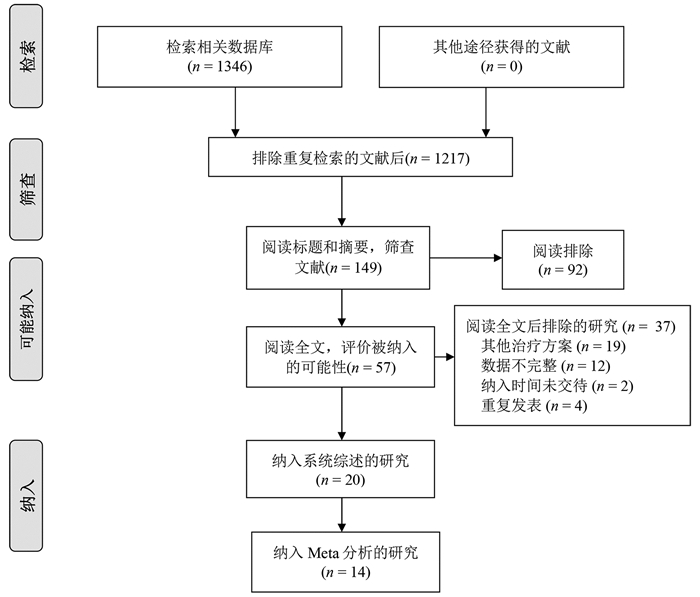
根据纳入和排除标准,18篇回顾性队列研究[3-20]和2篇随机对照试验[21-22]比较了再次肝切除术和RFA治疗复发性肝癌的临床疗效与安全性,共2903例患者(图 1)。全部纳入患者均来自亚洲国家,基线数据详见表 1。
表 1 纳入研究的基线特点第一作者和年份 国家/地区 纳入时间(年) 组别 样本量 男/女(例) 年龄(岁) 单个/多个肿瘤(例) 复发肿瘤直径(cm) 肝硬化[例(%)] CTP分级(A/B/C,例) 随访(月) Wang 2015[3] 中国 2004—2010 肝切除 128 113/15 50.2±10.1 89/39 2.4±0.9 66(51.6) - - RFA 162 148/14 52.7±10.9 107/55 2.3±0.7 - - - Sun 2017[4] 中国台湾 2002—2014 肝切除 43 34/9 60(35~76) - 1.9(0.8~3.0) 36(83.7) 42/1 53 RFA 57 38/19 63(27~81) - 1.8(1.0~3.0) 50(87.7) 57/0 54 Umeda 2011[5] 日本 1998—2007 肝切除 29 - - - 3.20±0.57 - 29/0 48 RFA 58 - - - 2.1±0.3 - 51/7 48 Song 2015[6] 韩国 1994—2012 肝切除 39 31/8 52.5±9.8 32/7 2.2±1.1 23(59) 39/0 36.3(0.8~126.6) RFA 178 145/33 55.4±10.6 156/22 1.7±0.6 130(73.0) 172/6 44.7(5.6~139.8) Liang 2008[7] 中国 1999—2007 肝切除 44 39/5 48.8±12.0 34/10 ≤3 (26) - 44/0 33.5±24.1 RFA 66 54/12 54.6±10.8 48/18 ≤3 (44) - 64/2 21.1±19.1 Ho 2012[8] 中国台湾 2001—2007 肝切除 54 40/14 56.3±12.3 - 2.9±1.8 26(48.1) 51/2/1 32(0~79) RFA 50 39/11 61.0±11.1 - 2.3±1.9 28(56.0) 50/0 27(0~96) Chan 2012[9] 中国香港 2001—2008 肝切除 29 - 52(38~79) 21/8 2.1(0.8~5.5) 25(86.2) 29/0 44.9 RFA 45 - 59(36~80) 29/16 2.2(0.8~6.0) 40(88.9) 40/5 44.9 Chen 2018[10] 中国 2009—2015 肝切除 48 41/7 73.5±3.5 28/20 2.6±1.1 41(85.4) 39/9 36.9(2~78) RFA 57 51/6 73.7±2.9 30/27 2.5±1.2 49(86.0) 45/12 37.3(2~78) 岑峰2016[11] 中国 2011—2015 肝切除 28 22/6 53.6 12/16 - 23(82.1) 18/10 - RFA 24 19/5 55.7 10/14 - 19(79.2) - - 陈康2019[12] 中国 2005—2014 肝切除 77 65/12 - - - 57(74) 76/1 57(2~168) RFA 82 72/10 - - - 50(61) 77/5 51(4~111) 黄新辉2013[13] 中国 2007—2011 肝切除 66 51/15 50.5±10.1 66/0 2.9±1.1 57(86.3) 66/0 - RFA 46 36/10 54.1±12.1 46/0 2.6±0.9 39(84.8) 46/0 - 梁惠宏2011[14] 中国 1999—2009 肝切除 72 65/7 49±12 72/0 2.1±0.1 - 70/2 36±25 RFA 79 69/10 55±11 79/0 2.5±0.1 - 73/6 32±21 任正刚2008[15] 中国 2000—2005 肝切除 145 127/18 51 127/18 2.0 - 145/0 23(3~88) RFA 68 64/4 52 52/16 2.0 - 68/0 23(3~88) 田正灵2016[16] 中国 2012—2015 肝切除 30 28/2 48.8±9.6 24/6 - 24(80) - 17(6.0~42.5) RFA 27 26/1 50.9±10.1 19/8 - 23(85.2) - 17(6.0~42.5) 张辉2013[17] 中国 2003—2011 肝切除 69 - - - 3.5 61(88.4) 54/15 - RFA 99 - - 2.1 76(76.8) 71/28 - 张婷婷2014[18] 中国 1998—2010 肝切除 27 25/2 47±13 25/2 3.2±1.1 - 27/0 32(9~118) RFA 39 37/2 52±13 37/2 2.7±1.1 - 37/2 28(2~79) Peng 2018[19] 中国 2006—2015 肝切除 79 67/2 55 59/20 ≤3(48) - - 53.2(4~96) RFA 107 95/12 57 75/32 ≤3(73) - - 52.3(3~96) Lu 2020[20] 中国 2004—2015 肝切除 138 124/16 50.1±10.9 112/26 2.8±1.9 96(70) 138/0 37.6 RFA 194 172/22 52.9±11.8 162/32 1.9±0.9 134(69) 194/0 41.6 Xia 2019[21] 中国 2010—2013 肝切除 120 107/13 52.4(25.7~60.5) 96/24 2.9(1.0~5.0) 50(41.7) 120/0 44.3(4.3~90.6) RFA 120 109/11 53.5(28.0~59.9) 94/26 2.7(1.0~4.8) 55(45.8) 120/0 44.3(4.3~90.6) 刘嘉龙2019[22] 中国 2016—2017 肝切除 39 38/1 50.0±10.0 37/2 2.1±0.7 37(94.9) 38/1 24 RFA 41 37/4 48.9±11.3 39/2 1.8±0.8 39(95.1) 39/2 24 注:-,未报道。 2.2 围术期并发症及病死率
15篇文献[4, 6-7, 9-17, 19, 21-22]报道了再次肝切除术围手术期并发症发生率为5.5%~68.2%,中位值为22.4%,常见并发症包括肝功能不全、胸腔积液、腹水、胆瘘等。14篇文献[4, 6-7, 9-10, 12-17, 19, 21-22]报道了RFA的围手术期并发症发生率为0~13%,中位值为3.3%,常见并发症包括胆漏、腹腔出血等。16篇文献[4, 6-7, 9-19, 21-22]报道了再次肝切除术和RFA围手术期病死率,其中6篇文献[4, 6, 10, 12, 17, 19]报道再次肝切除术组围手术期病死率为1.3%~2.6%,中位值为2%,其余文献报道发生率为0;仅1篇文献[9]报道RFA围手术期病死率为2.2%,其余文献报道发生率为0(表 2)。
表 2 纳入患者的治疗结局第一作者和年份 组别 并发症发生率(%) 围手术期病死率(%) 复发[例(%)] RFS OS 1年 3年 5年 P值1) 1年 3年 5年 P值1) Wang 2015[3] 肝切除 - - - - - - - 97.7 84.1 64.5 <0.001 RFA - - - - - - 96.9 73.4 37.0 Sun 2017[4] 肝切除 16 2 30(69.8) 57.0 32.1 28.6 0.89 97.6 82.7 56.4 0.69 RFA 7 0 41(71.9) 60.8 26.6 16.6 98.2 77.2 52.6 Umeda 2011[5] 肝切除 - - - - - - - 93.1 66.8 58.1 0.899 RFA - - - - - - 94.7 75.1 48.3 Song 2015[6] 肝切除 64 2.6 18(46.2) 66.1 48.5 43.1 0.834 88.8 88.8 83.9 0.686 RFA 2.2 0 117(65.7) 70.1 40.8 30.0 98.9 82.5 71.0 Liang 2008[7] 肝切除 68.2 0 86.4 - - - - 78.6 44.5 27.6 0.79 RFA 3.0 0 78.8 - - - 76.6 48.6 39.9 Ho 2012[8] 肝切除 - - - - - - - - - 72.0 - RFA - - - - - - - - 83.0 Chan 2012[9] 肝切除 24.1 0 21(72.4) 41.1 24.2 24.2 0.14 89.7 56.5 35.2 0.51 RFA 2.2 2.2 38(84.4) 32.2 12.4 9.3 83.7 43.1 29.1 Chen 2018[10] 肝切除 25 2.1 26(54.2) 73.1 49.7 40.7 0.465 76.3 52.5 42.6 0.413 RFA 0 0 27(47.4) 69.5 37.8 33.1 78.2 40.8 36.7 岑峰2016[11] 肝切除 50 0 - 46.4 0 0 - - - - - RFA - 0 - 20.8 0 0 - - - 陈康2019[12] 肝切除 17.1 1.3 - - - - - 88.8 68.8 51.1 0.258 RFA 9.8 0 - - - - 91.4 73.4 61.1 黄新辉2013[13] 肝切除 18.1 0 - 43.9 14.4 8.2 0.548 89.5 54.3 28.8 0.780 RFA 0 0 - 56.9 12.4 5.0 82.6 50.8 20.5 梁惠宏2011[14] 肝切除 36 0 ≤1年: 39>1年: 33 - - - - 95.3 65.7 54.5 >0.05 RFA 13 0 ≤1年: 37>1年: 42 - - - - 100 79.4 62.1 任正刚2008[15] 肝切除 5.5 0 ≤2年: 71>2年: 74 79.4 48.1 34.4 0.001 88.1 62.6 41.0 0.693 RFA 1.5 0 ≤2年: 37>2年: 31 58.0 27.8 12.4 94.7 65.1 37.3 田正灵2016[16] 肝切除 6.7 0 10(33.3) 73.3 64.3 - 0.002 96.7 93.3 - 0.54 RFA 3.7 0 24(88.9) 46.7 26.7 - 96.3 84.0 - 张辉2013[17] 肝切除 15.9 1.45 - - - - - 68.2 45.4 - >0.05 RFA 0 0 - - - - 73.7 53.6 - 张婷婷2014[18] 肝切除 - 0 22(56.4) 66.7 50.7 43.4 0.323 96.2 76.9 61.2 0.471 RFA - 0 14(52.9) 65.8 28.0 14.0 86.2 73.3 62.2 Peng 2018[19] 肝切除 17.7 1.3 - 64.8 41.6 38.3 0.258 84.8 60.2 51.9 0.871 RFA 4.7 0 - 58.2 35.2 29.6 84.6 66.9 49.1 Lu 2020[20] 肝切除 - - - 91.8 82.0 72.9 0.38 - - - - RFA - - - 94.4 75.4 61.7 - - - Xia 2019[21] 肝切除 22.4 0 60.8 85.0 52.4 36.2 0.09 92.5 65.8 43.6 0.17 RFA 7.3 0 64.2 74.2 41.7 30.2 87.5 52.5 38.5 刘嘉龙2019[22] 肝切除 35.9 0 19(48.7) 69.2 - - <0.001 92.3 - - 0.292 RFA 4.9 0 32(78.0) 26.8 - - 85.4 - - 注:-,未报道;1) P值来源于原文报道。 2.3 RFA与肝切除术OS的比较
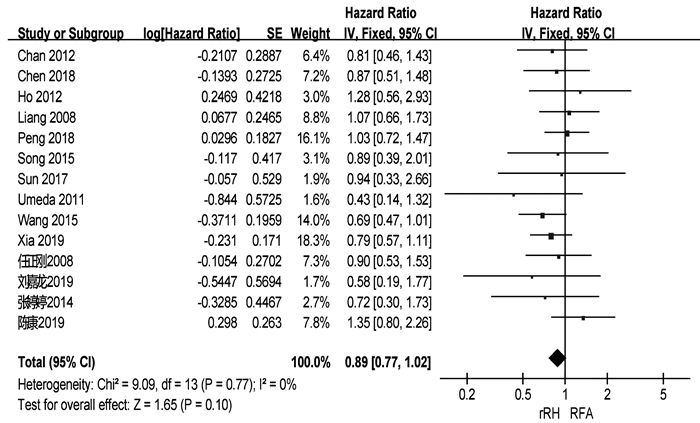
共有18篇研究[3-10, 12-18, 21-22]报道了OS(表 2)。两组患者术后1、3、5年中位OS分别为92.3%、66.3%、51.1%与91.4%、69.2%、39.9%。共有14篇研究[3-10, 12, 15, 18-19, 21-22]可提取数据统计HR,各组间不存在异质性(I2=0,P=0.77),采用固定效应模型进行分析。结果显示,两组患者的OS差异无统计学意义(HR= 0.89,95%CI:0.77~1.02,P=0.10)(图 2)。
2.4 RFA与肝切除术RFS的比较
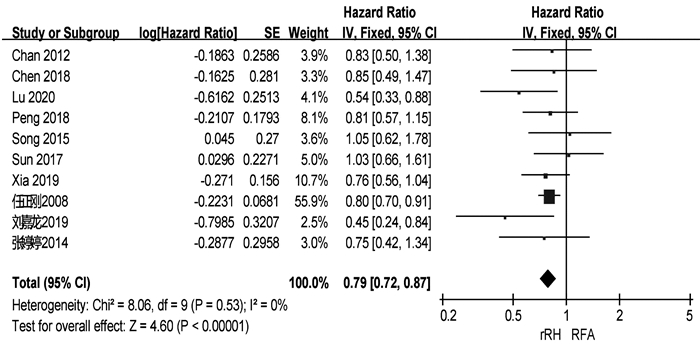
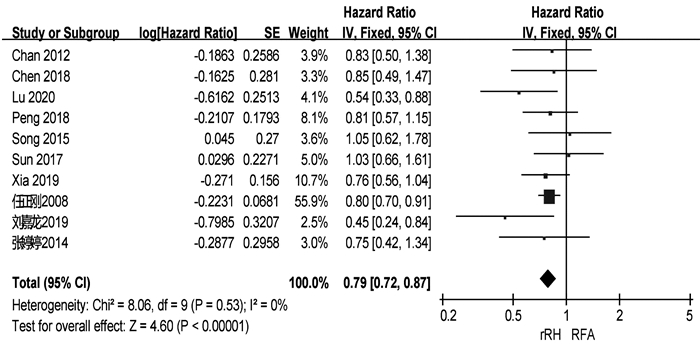
共有13篇研究[4, 6, 9-11, 13, 15-16, 18-19, 20-22]报道了RFS(表 2)。两组患者术后1、3、5年中位RFS分别为67.9%、48.3%、34.4%和57.5%、27.9%、14.0%。共有10篇研究[4, 6, 9-10, 15, 18-22]可提取数据统计HR,各组间不存在异质性(I2=0,P=0.53),采用固定效应模型进行分析。结果显示,再次肝切除术组患者的RFS显著高于RFA组(HR=0.79,95%CI:0.72~0.87,P<0.001)(图 3)。
2.5 发表偏倚
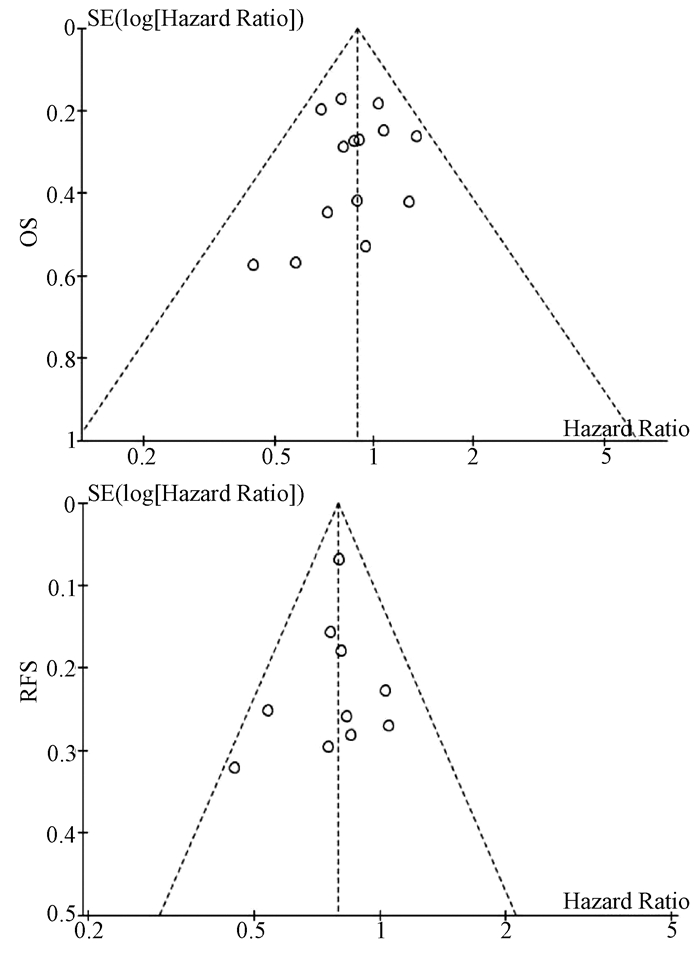
基于OS和RFS HR的漏斗图提示,发表偏倚不明显(图 4)。
3. 讨论
肝癌术后复发是影响患者术后长期生存的主要危险因素。对于复发性肝癌,目前临床上以多学科综合治疗为主。肝移植能显著提高复发性肝癌患者的RFS和远期生存率[23],但肝移植适应证严格、肝源匮乏和费用昂贵等问题仍限制其广泛的临床应用。此外,既往研究[24-25]表明再次肝切除术和RFA对复发性肝癌的疗效均优于介入。因此,针对肝内复发性肝癌患者,再次肝切除术和RFA是目前较为理想的治疗方案。有研究[3]认为再次肝切除术是治疗复发性肝癌的首选治疗方案,即使患者的原发癌更具侵袭性,肝功能水平更差,肝癌复发后行再次肝切除术仍可以获得与RFA相似的疗效。梁惠宏等[14]的研究则发现,RFA治疗复发性小肝癌的长期疗效优于再次肝切除术。因此,关于再次肝切除术和RFA治疗复发性肝癌的选择仍存在较大争议。本研究通过Meta分析的方法,综合评估再次肝切除术和RFA治疗复发性肝癌的疗效和安全性。
本研究结果显示,两组患者的OS无显著性差异,但再次肝切除术组患者的RFS显著高于RFA组。这一结论与肝切除术和RFA治疗原发性肝癌的结果一致[26-27]。RFA组患者RFS偏低的原因可能是:(1)再次肝切除术能将复发肿瘤以及潜在的瘤周子灶及血管癌栓同时切除,减少肿瘤再次局部复发和转移的可能性;(2)RFA后部分患者的肿瘤消融不完全而需进行二次消融或其他治疗;(3)术前影像学检查未能发现主瘤旁的微小卫星灶,导致消融不完全而引起肝癌再次复发。虽然RFA可用于治疗直径≤5 cm的肝癌,但目前认为其最佳适应证为直径≤3 cm的小肝癌[28]。有研究[29]发现,肝癌的直径和数目是导致RFA消融不完全的主要因素,随着肝癌直径的增加,RFA的疗效逐步下降。Livraghi等[30]的研究也表明RFA治疗直径3~5 cm的肝癌时完全消融率显著降低,导致RFA治疗复发性肝癌后局部复发和早期复发的比例明显升高。无论是原发性还是复发性肝癌,肿瘤直径在3~5 cm时经RFA治疗后其RFS和远期生存率均低于再次肝切除术[21, 31]。因此,在选择复发性肝癌治疗方案时,肿瘤直径应作为重要的参考指标。
本研究中,在围手术期并发症方面,再次肝切除术组和RFA组患者的中位发生率分别为22.4%和3.3%,与原发性肝癌接受肝切除术或RFA治疗后的并发症发生率相似[32-33]。此外,本研究还发现RFA治疗复发性肝癌的安全性明显优于再次肝切除术。RFA组患者术后并发症发生率及严重程度更低。虽然再次肝切除术能改善患者的远期生存率及RFS,但再次肝切除术的实施仍受诸多因素的限制,例如复发肿瘤的位置、数量以及肝硬化严重程度等。手术造成较大的创伤导致患者术后更容易发生严重并发症。此外,肝癌患者常伴有不同程度的肝硬化,无疑增加了手术的风险,部分患者最终死于肝衰竭而非肝癌本身带来的肿瘤负担[32]。相比于再次肝切除术,RFA在超声等影像学技术引导下精准地对复发肿瘤进行消融,从而最大限度地避免正常肝组织的破坏。对于手术无法切除、无法耐受手术的患者亦可选择RFA治疗。此外,RFA还可联合介入或无水酒精注射提高患者的OS和RFS[10, 19]。RFA本身具有微创和可重复的优点,肝癌再次复发后相当一部分患者仍可及时接受RFA或其他治疗[12],从而获得与再次肝切除相似的短期OS。
值得注意的是,本研究纳入文献中多数为回顾性研究,仅有2篇随机对照试验,因此本研究结论仍需更多的随机对照试验进行验证。其次,再次肝切除术和RFA治疗复发性肝癌的适应证存在一定的区别。然而,本Meta分析纳入的多数文献均仅纳入符合米兰标准的复发性肝癌,这些患者同时符合再次肝切除术和RFA的适应证。最后,肝癌术后复发(甚至多次)比较常见,对于复发肿瘤的治疗,多采取综合治疗方案(如介入、靶向、免疫治疗等),而非再次肝切除术或RFA等“单一”治疗模式。因此,联合治疗方案可能影响本荟萃分析对患者OS的判断。
总而言之,对于复发性肝癌的治疗,再次肝切除术能提高患者RFS,RFA则具有安全性高的优点。因此,在复发性肝癌患者的治疗中应遵循个体化和多学科治疗原则,合理选择治疗方案。
-
表 1 纳入研究的基线特点
第一作者和年份 国家/地区 纳入时间(年) 组别 样本量 男/女(例) 年龄(岁) 单个/多个肿瘤(例) 复发肿瘤直径(cm) 肝硬化[例(%)] CTP分级(A/B/C,例) 随访(月) Wang 2015[3] 中国 2004—2010 肝切除 128 113/15 50.2±10.1 89/39 2.4±0.9 66(51.6) - - RFA 162 148/14 52.7±10.9 107/55 2.3±0.7 - - - Sun 2017[4] 中国台湾 2002—2014 肝切除 43 34/9 60(35~76) - 1.9(0.8~3.0) 36(83.7) 42/1 53 RFA 57 38/19 63(27~81) - 1.8(1.0~3.0) 50(87.7) 57/0 54 Umeda 2011[5] 日本 1998—2007 肝切除 29 - - - 3.20±0.57 - 29/0 48 RFA 58 - - - 2.1±0.3 - 51/7 48 Song 2015[6] 韩国 1994—2012 肝切除 39 31/8 52.5±9.8 32/7 2.2±1.1 23(59) 39/0 36.3(0.8~126.6) RFA 178 145/33 55.4±10.6 156/22 1.7±0.6 130(73.0) 172/6 44.7(5.6~139.8) Liang 2008[7] 中国 1999—2007 肝切除 44 39/5 48.8±12.0 34/10 ≤3 (26) - 44/0 33.5±24.1 RFA 66 54/12 54.6±10.8 48/18 ≤3 (44) - 64/2 21.1±19.1 Ho 2012[8] 中国台湾 2001—2007 肝切除 54 40/14 56.3±12.3 - 2.9±1.8 26(48.1) 51/2/1 32(0~79) RFA 50 39/11 61.0±11.1 - 2.3±1.9 28(56.0) 50/0 27(0~96) Chan 2012[9] 中国香港 2001—2008 肝切除 29 - 52(38~79) 21/8 2.1(0.8~5.5) 25(86.2) 29/0 44.9 RFA 45 - 59(36~80) 29/16 2.2(0.8~6.0) 40(88.9) 40/5 44.9 Chen 2018[10] 中国 2009—2015 肝切除 48 41/7 73.5±3.5 28/20 2.6±1.1 41(85.4) 39/9 36.9(2~78) RFA 57 51/6 73.7±2.9 30/27 2.5±1.2 49(86.0) 45/12 37.3(2~78) 岑峰2016[11] 中国 2011—2015 肝切除 28 22/6 53.6 12/16 - 23(82.1) 18/10 - RFA 24 19/5 55.7 10/14 - 19(79.2) - - 陈康2019[12] 中国 2005—2014 肝切除 77 65/12 - - - 57(74) 76/1 57(2~168) RFA 82 72/10 - - - 50(61) 77/5 51(4~111) 黄新辉2013[13] 中国 2007—2011 肝切除 66 51/15 50.5±10.1 66/0 2.9±1.1 57(86.3) 66/0 - RFA 46 36/10 54.1±12.1 46/0 2.6±0.9 39(84.8) 46/0 - 梁惠宏2011[14] 中国 1999—2009 肝切除 72 65/7 49±12 72/0 2.1±0.1 - 70/2 36±25 RFA 79 69/10 55±11 79/0 2.5±0.1 - 73/6 32±21 任正刚2008[15] 中国 2000—2005 肝切除 145 127/18 51 127/18 2.0 - 145/0 23(3~88) RFA 68 64/4 52 52/16 2.0 - 68/0 23(3~88) 田正灵2016[16] 中国 2012—2015 肝切除 30 28/2 48.8±9.6 24/6 - 24(80) - 17(6.0~42.5) RFA 27 26/1 50.9±10.1 19/8 - 23(85.2) - 17(6.0~42.5) 张辉2013[17] 中国 2003—2011 肝切除 69 - - - 3.5 61(88.4) 54/15 - RFA 99 - - 2.1 76(76.8) 71/28 - 张婷婷2014[18] 中国 1998—2010 肝切除 27 25/2 47±13 25/2 3.2±1.1 - 27/0 32(9~118) RFA 39 37/2 52±13 37/2 2.7±1.1 - 37/2 28(2~79) Peng 2018[19] 中国 2006—2015 肝切除 79 67/2 55 59/20 ≤3(48) - - 53.2(4~96) RFA 107 95/12 57 75/32 ≤3(73) - - 52.3(3~96) Lu 2020[20] 中国 2004—2015 肝切除 138 124/16 50.1±10.9 112/26 2.8±1.9 96(70) 138/0 37.6 RFA 194 172/22 52.9±11.8 162/32 1.9±0.9 134(69) 194/0 41.6 Xia 2019[21] 中国 2010—2013 肝切除 120 107/13 52.4(25.7~60.5) 96/24 2.9(1.0~5.0) 50(41.7) 120/0 44.3(4.3~90.6) RFA 120 109/11 53.5(28.0~59.9) 94/26 2.7(1.0~4.8) 55(45.8) 120/0 44.3(4.3~90.6) 刘嘉龙2019[22] 中国 2016—2017 肝切除 39 38/1 50.0±10.0 37/2 2.1±0.7 37(94.9) 38/1 24 RFA 41 37/4 48.9±11.3 39/2 1.8±0.8 39(95.1) 39/2 24 注:-,未报道。  下载: 导出CSV
下载: 导出CSV
表 2 纳入患者的治疗结局
第一作者和年份 组别 并发症发生率(%) 围手术期病死率(%) 复发[例(%)] RFS OS 1年 3年 5年 P值1) 1年 3年 5年 P值1) Wang 2015[3] 肝切除 - - - - - - - 97.7 84.1 64.5 <0.001 RFA - - - - - - 96.9 73.4 37.0 Sun 2017[4] 肝切除 16 2 30(69.8) 57.0 32.1 28.6 0.89 97.6 82.7 56.4 0.69 RFA 7 0 41(71.9) 60.8 26.6 16.6 98.2 77.2 52.6 Umeda 2011[5] 肝切除 - - - - - - - 93.1 66.8 58.1 0.899 RFA - - - - - - 94.7 75.1 48.3 Song 2015[6] 肝切除 64 2.6 18(46.2) 66.1 48.5 43.1 0.834 88.8 88.8 83.9 0.686 RFA 2.2 0 117(65.7) 70.1 40.8 30.0 98.9 82.5 71.0 Liang 2008[7] 肝切除 68.2 0 86.4 - - - - 78.6 44.5 27.6 0.79 RFA 3.0 0 78.8 - - - 76.6 48.6 39.9 Ho 2012[8] 肝切除 - - - - - - - - - 72.0 - RFA - - - - - - - - 83.0 Chan 2012[9] 肝切除 24.1 0 21(72.4) 41.1 24.2 24.2 0.14 89.7 56.5 35.2 0.51 RFA 2.2 2.2 38(84.4) 32.2 12.4 9.3 83.7 43.1 29.1 Chen 2018[10] 肝切除 25 2.1 26(54.2) 73.1 49.7 40.7 0.465 76.3 52.5 42.6 0.413 RFA 0 0 27(47.4) 69.5 37.8 33.1 78.2 40.8 36.7 岑峰2016[11] 肝切除 50 0 - 46.4 0 0 - - - - - RFA - 0 - 20.8 0 0 - - - 陈康2019[12] 肝切除 17.1 1.3 - - - - - 88.8 68.8 51.1 0.258 RFA 9.8 0 - - - - 91.4 73.4 61.1 黄新辉2013[13] 肝切除 18.1 0 - 43.9 14.4 8.2 0.548 89.5 54.3 28.8 0.780 RFA 0 0 - 56.9 12.4 5.0 82.6 50.8 20.5 梁惠宏2011[14] 肝切除 36 0 ≤1年: 39>1年: 33 - - - - 95.3 65.7 54.5 >0.05 RFA 13 0 ≤1年: 37>1年: 42 - - - - 100 79.4 62.1 任正刚2008[15] 肝切除 5.5 0 ≤2年: 71>2年: 74 79.4 48.1 34.4 0.001 88.1 62.6 41.0 0.693 RFA 1.5 0 ≤2年: 37>2年: 31 58.0 27.8 12.4 94.7 65.1 37.3 田正灵2016[16] 肝切除 6.7 0 10(33.3) 73.3 64.3 - 0.002 96.7 93.3 - 0.54 RFA 3.7 0 24(88.9) 46.7 26.7 - 96.3 84.0 - 张辉2013[17] 肝切除 15.9 1.45 - - - - - 68.2 45.4 - >0.05 RFA 0 0 - - - - 73.7 53.6 - 张婷婷2014[18] 肝切除 - 0 22(56.4) 66.7 50.7 43.4 0.323 96.2 76.9 61.2 0.471 RFA - 0 14(52.9) 65.8 28.0 14.0 86.2 73.3 62.2 Peng 2018[19] 肝切除 17.7 1.3 - 64.8 41.6 38.3 0.258 84.8 60.2 51.9 0.871 RFA 4.7 0 - 58.2 35.2 29.6 84.6 66.9 49.1 Lu 2020[20] 肝切除 - - - 91.8 82.0 72.9 0.38 - - - - RFA - - - 94.4 75.4 61.7 - - - Xia 2019[21] 肝切除 22.4 0 60.8 85.0 52.4 36.2 0.09 92.5 65.8 43.6 0.17 RFA 7.3 0 64.2 74.2 41.7 30.2 87.5 52.5 38.5 刘嘉龙2019[22] 肝切除 35.9 0 19(48.7) 69.2 - - <0.001 92.3 - - 0.292 RFA 4.9 0 32(78.0) 26.8 - - 85.4 - - 注:-,未报道;1) P值来源于原文报道。
下载: 导出CSV
-
[1] WANG YY, LIU JM, WANG LJ, et al. Prognostic value of tumor burden score in patients with hepatocellular carcinoma[J]. Chin J Oncol Prev Treat, 2019, 11(5): 393-397. DOI: 10.3969/j.issn.1674-5671.2019.05.06.王言焱, 刘佳明, 王立军, 等. 肿瘤负荷评分在肝细胞癌患者预后预测中的价值[J]. 中国癌症防治杂志, 2019, 11(5): 393-397. DOI: 10.3969/j.issn.1674-5671.2019.05.06. [2] European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma[J]. J Hepatol, 2018, 69(1): 182-236. DOI: 10.1016/j.jhep.2018.03.019. [3] WANG K, LIU G, LI J, et al. Early intrahepatic recurrence of hepatocellular carcinoma after hepatectomy treated with re-hepatectomy, ablation or chemoembolization: A prospective cohort study[J]. Eur J Surg Oncol, 2015, 41(2): 236-242. DOI: 10.1016/j.ejso.2014.11.002. [4] SUN WC, CHEN IS, LIANG HL, et al. Comparison of repeated surgical resection and radiofrequency ablation for small recurrent hepatocellular carcinoma after primary resection[J]. Oncotarget, 2017, 8(61): 104571-104581. DOI: 10.18632/oncotarget.21604. [5] UMEDA Y, MATSUDA H, SADAMORI H, et al. A prognostic model and treatment strategy for intrahepatic recurrence of hepatocellular carcinoma after curative resection[J]. World J Surg, 2011, 35(1): 170-177. DOI: 10.1007/s00268-010-0794-8. [6] SONG KD, LIM HK, RHIM H, et al. Repeated hepatic resection versus radiofrequency ablation for recurrent hepatocellular carcinoma after hepatic resection: A propensity score matching study[J]. Radiology, 2015, 275(2): 599-608. DOI: 10.1148/radiol.14141568. [7] LIANG HH, CHEN MS, PENG ZW, et al. Percutaneous radiofrequency ablation versus repeat hepatectomy for recurrent hepatocellular carcinoma: A retrospective study[J]. Ann Surg Oncol, 2008, 15(12): 3484-3493. DOI: 10.1245/s10434-008-0076-y. [8] HO CM, LEE PH, SHAU WY, et al. Survival in patients with recurrent hepatocellular carcinoma after primary hepatectomy: Comparative effectiveness of treatment modalities[J]. Surgery, 2012, 151(5): 700-709. DOI: 10.1016/j.surg.2011.12.015. [9] CHAN AC, POON RT, CHEUNG TT, et al. Survival analysis of re-resection versus radiofrequency ablation for intrahepatic recurrence after hepatectomy for hepatocellular carcinoma[J]. World J Surg, 2012, 36(1): 151-156. DOI: 10.1007/s00268-011-1323-0. [10] CHEN S, PENG Z, XIAO H, et al. Combined radiofrequency ablation and ethanol injection versus repeat hepatectomy for elderly patients with recurrent hepatocellular carcinoma after initial hepatic surgery[J]. Int J Hyperthermia, 2018, 34(7): 1029-1037. DOI: 10.1080/02656736.2017.1387941. [11] CEN F. Analysis of curative effect of repeated hepatectomy for recurrent HCC[D]. Hangzhou: Zhejiang University School of Medicine, 2016.岑峰. 复发性肝癌行再次肝切除术治疗的疗效分析研究[D]. 杭州: 浙江大学, 2016. [12] CHEN K, LIU XY, TENG YX, et al. Rehepatectomyand radiofrequency ablation for patients with recurrent hepatocellular carcinoma[J]. Chin J Practic Surg, 2019, 39(10): 1060-1064. DOI: 10.19538/j.cjps.issn1005-2208.2019.10.16.陈康, 刘新宇, 滕煜宪, 等. 再次肝切除与射频消融治疗复发性肝癌疗效对比研究[J]. 中国实用外科杂志, 2019, 39(10): 1060-1064. DOI: 10.19538/j.cjps.issn1005-2208.2019.10.16. [13] HUANG XH, HUANG Y, LIN KC, et al. The curative efficacy comparison of percntaneons radiofrequency ablation versus surgical re-resection for recurrent small hepatocellular carcinoma[J]. J Abdominal Surg, 2013, 26(2): 93-95. DOI: 10.3969/j.issn.1003-5591.2013. 02.008.黄新辉, 黄尧, 林科灿, 等. 复发性小肝细胞癌射频消融与再手术切除疗效的分析[J]. 腹部外科, 2013, 26(2): 93-95. DOI: 10.3969/j.issn.1003-5591.2013. 02.008. [14] LIANG HH, PENG ZW, CHEN MS, et al. Effects of percutaneous radiofrequency ablation and repeat hepatectomy for the treatment of solitary recurrent hepatocelluar carcinoma with the diameter no more than 3 cm[J]. Chin J Dig Surg, 2011, 10(1): 36-39. DOI: 10.3760/cma.j.issn. 1673-9752. 2011.01.010.梁惠宏, 彭振维, 陈敏山, 等. 经皮射频消融与再手术治疗单个直径≤3 cm的复发性肝癌的疗效比较[J]. 中华消化外科杂志, 2011, 10(1): 36-39. DOI: 10.3760/cma.j.issn.1673-9752. 2011.01.010. [15] REN ZG, GAN YH, FAN J, et al. Treatment of postoperative recurrence of hepatocellular carcinoma with radiofrequency ablation comparing with repeated surgical resection[J]. Chin J Surg, 2008, 46(21): 1614-1616. DOI: 10.3321/j.issn:0529-5815.2008.21.005.任正刚, 干育红, 樊嘉, 等. 射频毁损术与再手术切除治疗复发性小肝癌对照研究[J]. 中华外科杂志, 2008, 46(21): 1614-1616. DOI: 10.3321/j.issn:0529-5815.2008.21.005. [16] TIAN ZL. Investigate the efficacy between radiofrequency ablation and surgical resection in the treatment of small recurrent hepatocellular carcinoma: An retrospective analysis of 57 cases[D]. Nanning: Guangxi Medical University, 2016.田正灵. 射频消融与手术切除治疗复发性小肝细胞性肝癌的疗效比较分析(附57例病例分析)[D]. 南宁: 广西医科大学, 2016. [17] ZHANG H, XU XB, HE XJ, et al. Compare of the efficacy between re-operative and radiofrequency ablation on postoperative recurrent carcinoma[J]. Med J West China, 2013, 25(12): 1816-1818. DOI: 10.3969/j.issn.1672-3511.2013.12.019.张辉, 徐新保, 何晓军, 等. 原发性肝癌术后复发再手术切除与射频消融治疗的疗效比较[J]. 西部医学, 2013, 25(12): 1816-1818. DOI: 10.3969/j.issn.1672-3511.2013.12.019. [18] ZHANG TT, LI KY, LUO HC, et al. Long-term outcomes of percutaneous microwave ablation versus repeat hepatectomy for treatment of late recurrent small hepatocellular carcinoma: A retrospective study[J]. Natl Med J China, 2014, 94(33): 2570-2572. DOI: 10.3760/cma. j.issn.0376-2491.2014.33.004.张婷婷, 李开艳, 罗鸿昌, 等. 经皮微波消融和二次手术治疗晚期复发型小肝癌的长期疗效观察[J]. 中华医学杂志, 2014, 94(33): 2570-2572. DOI: 10.3760/cma.j.issn.0376-2491. 2014.33.004. [19] PENG Z, WEI M, CHEN S, et al. Combined transcatheter arterial chemoembolization and radiofrequency ablation versus hepatectomy for recurrent hepatocellular carcinoma after initial surgery: A propensity score matching study[J]. Eur Radiol, 2018, 28(8): 3522-3531. DOI: 10.1007/s00330-017-5166-4. [20] LU LH, MEI J, KAN A, et al. Treatment optimization for recurrent hepatocellular carcinoma: Repeat hepatic resection versus radiofrequency ablation[J]. Cancer Med, 2020, 9(9): 2997-3005. DOI: 10.1002/cam4.2951. [21] XIA Y, LI J, LIU G, et al. Long-term effects of repeat hepatectomy vs percutaneous radiofrequency ablation among patients with recurrent hepatocellular carcinoma: A randomized clinical trial[J]. JAMA Oncol, 2020, 6(2): 255-263. DOI: 10.1001/jamaoncol.2019.4477. [22] LIU JL, HUANG D, CAO L, et al. Laparoscopic hepatectomy versus radiofrequency ablation in treatment of recurrent hepatocellular carcinoma: A prospective randomized control study based on interim follow-up analysis[J]. J Third Milit Med Univ, 2019, 41(5): 467-472. DOI: 10.16016/j.1000-5404.201811005.刘嘉龙, 黄登, 曹利, 等. 腹腔镜肝切除术和射频消融术治疗复发性肝癌的前瞻性随机对照研究(中期随访分析)[J]. 第三军医大学学报, 2019, 41(5): 467-472. DOI: 10.16016/j.1000-5404.201811005. [23] CHAN AC, CHAN SC, CHOK KS, et al. Treatment strategy for recurrent hepatocellular carcinoma: Salvage transplantation, repeated resection, or radiofrequency ablation?[J]. Liver Transpl, 2013, 19(4): 411-419. DOI: 10.1002/lt.23605. [24] CHEN R, GAN Y, GE N, et al. Transarterial chemoembolization versus radiofrequency ablation for recurrent hepatocellular carcinoma after resection within barcelona clinic liver cancer stage 0/A: A retrospective comparative study[J]. J Vasc Interv Radiol, 2016, 27(12): 1829-1836. DOI: 10.1016/j.jvir.2016.06.010. [25] HIROKAWA F, HAYASHI M, MIYAMOTO Y, et al. Appropriate treatment strategy for intrahepatic recurrence after curative hepatectomy for hepatocellular carcinoma[J]. J Gastrointest Surg, 2011, 15(7): 1182-1187. DOI: 10.1007/s11605-011-1484-z. [26] WANG N, ZHENG JL, JIANG L. Clinical effect of surgical resection versus radiofrequency ablation in treatment of multiple liver cancer in different liver segments meeting the Milan criteria[J]. J Clin Hepatol, 2020, 36(4): 792-797. DOI: 10.3969/j.issn.1001-5256.2020.04.017.王宁, 郑金利, 蒋利. 手术切除与射频消融治疗符合米兰标准的不同肝段多发肝癌的效果分析[J]. 临床肝胆病杂志, 2020, 36(4): 792-797. DOI: 10.3969/j.issn.1001-5256.2020.04.017. [27] DUAN C, LIU M, ZHANG Z, et al. Radiofrequency ablation versus hepatic resection for the treatment of early-stage hepatocellular carcinoma meeting Milan criteria: A systematic review and meta-analysis[J]. World J Surg Oncol, 2013, 11(1): 190. DOI: 10.1186/1477-7819-11-190. [28] LIN SM, LIN CJ, LIN CC, et al. Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3 cm or less[J]. Gut, 2005, 54(8): 1151-1156. DOI: 10.1136/gut.2004.045203. [29] PENG ZW, ZHANG YJ, CHEN MS, et al. Risk factors of survival after percutaneous radiofrequency ablation of hepatocellular carcinoma[J]. Surg Oncol, 2008, 17(1): 23-31. DOI: 10.1016/j.suronc.2007.08.002. [30] LIVRAGHI T, LAZZARONI S, MELONI F. Radiofrequency thermal ablation of hepatocellular carcinoma[J]. Eur J Ultrasound, 2001, 13(2): 159-166. DOI: 10.1016/s0929- 8266(01)00128-8. [31] HUANG J, YAN L, CHENG Z, et al. A randomized trial comparing radiofrequency ablation and surgical resection for HCC conforming to the Milan criteria[J]. Ann Surg, 2010, 252(6): 903-912. DOI: 10.1097/SLA.0b013e3181efc656. [32] ZHONG JH, KE Y, GONG WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma[J]. Ann Surg, 2014, 260(2): 329-340. DOI: 10.1097/SLA.0000000000000236. [33] LEE S, KANG TW, SONG KD, et al. Effect of microvascular invasion risk on early recurrence of hepatocellular carcinoma after surgery and radiofrequency ablation[J]. Ann Surg, 2019, 273(3): 564-571. DOI: 10.1097/SLA.0000000000003268. 期刊类型引用(4)
1. 卢冰. 再次肝切除术和射频消融术在治疗肝切除术后早期复发性小肝癌中的疗效比较. 医药论坛杂志. 2024(06): 620-623+628 .  百度学术
百度学术2. 刘明强. 射频消融与肝动脉化疗栓塞术治疗复发性肝癌的效果对比. 中外医疗. 2024(12): 21-24 . 百度学术3. 周亚丹. 围术期预见性护理对肝癌射频消融术患者的影响. 国际医药卫生导报. 2023(05): 708-713 . 百度学术4. 姚加堤. 射频消融术在原发性肝癌术后复发患者中的应用价值. 中外医学研究. 2023(29): 49-52 . 百度学术其他类型引用(0)
-

 下载:
下载:


 百度学术
百度学术

