
 PDF下载 ( 2738 KB)
PDF下载 ( 2738 KB)

经皮冷冻消融联合无水酒精注射治疗70岁以上老年肝细胞癌患者的效果及安全性分析
DOI: 10.3969/j.issn.1001-5256.2022.02.021
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:罗婧和吕采红参与了研究数据的获取分析过程;杨永平参与了研究的思路设计。
Clinical efficacy and safety of percutaneous cryoablation combined with percutaneous ethanol injection in elderly patients with hepatocellular carcinoma aged 70 years or older
-
摘要:
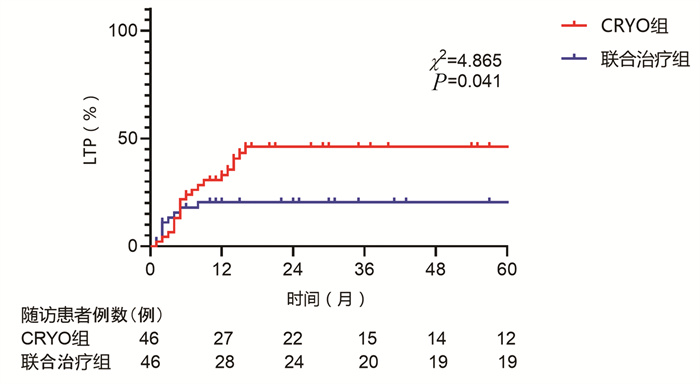
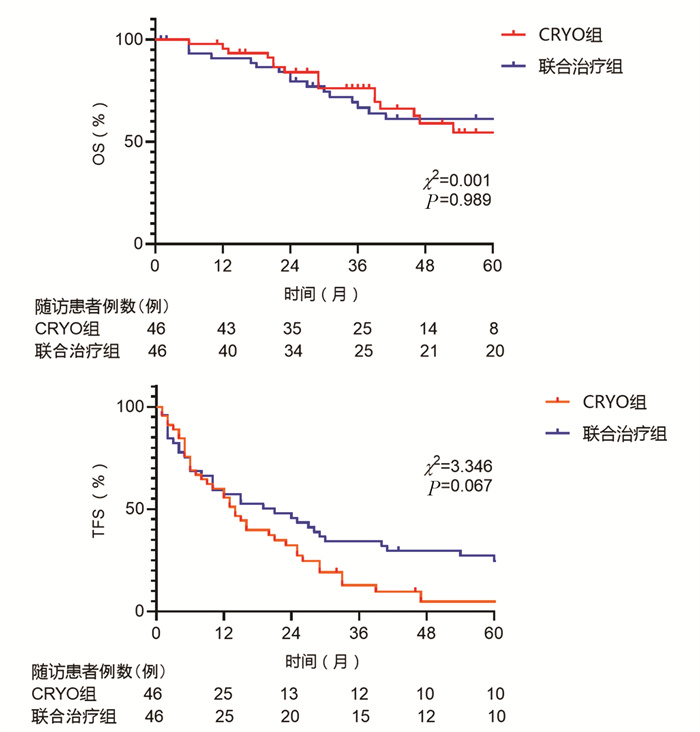
目的 探讨经皮冷冻消融(CRYO)联合无水酒精注射(PEI)对早期老年肝细胞癌患者的疗效和安全性。 方法 回顾性纳入解放军总医院第五医学中心2014年1月—2018年1月收治的92例老年肝细胞癌患者,其中单一CRYO治疗组46例,CRYO联合PEI(联合治疗)组46例。比较两种治疗方式的效果,不良反应及治疗前后肝功能相关指标的变化,并随访患者肿瘤的复发及生存预后情况。正态分布的计量资料两组间比较用t检验;非正态分布的计量资料两组间比较采用Mann-Whitney U秩和检验。计数资料两组间比较采用χ2检验。两组的生存时间采用Kaplan-Meier方法进行生存分析,并用log-rank检验生存曲线的差异;通过Cox回归法确定影响生存预后的独立危险因素。 结果 联合治疗组和CRYO组初次消融的有效率分别为89.1%和73.9%,组间差异无统计学意义(P>0.05)。CRYO组和联合治疗组患者术后总生存率和无瘤生存率间的差异均无统计学意义(P值均>0.05),但联合治疗组患者术后第1、2和3年局部肿瘤进展率分别为20%、21%和21%,明显低于CRYO组的30%、46%、46%(χ2=4.187,P<0.05)。多因素Cox回归分析提示行单一CRYO治疗可能是局部肿瘤进展率的独立危险因素(HR=2.206,95%CI: 1.003~4.850, P=0.049)。在不良反应的发生率上两组间差异没有统计学意义(P>0.05),但CRYO组有3例严重不良反应,联合治疗组未出现严重不良反应。 结论 对于早期老年肝细胞癌患者,CRYO联合PEI治疗较单纯CRYO治疗安全有效,能明显降低局部肿瘤进展率。 Abstract:Objective To investigate the clinical efficacy and safety of percutaneous cryoablation combined with percutaneous ethanol injection (PEI) in elderly patients with early-stage hepatocellular carcinoma aged 70 years or older. Methods A retrospective analysis was performed for the clinical data of 92 elderly patients with hepatocellular carcinoma who were admitted to The Fifth Medical Center of Chinese PLA General Hospital from January 2014 to January 2018, among whom 46 underwent cryoablation alone (CRYO group) and 46 underwent cryoablation combined with PEI (combination therapy group). The two groups were compared in terms of clinical outcome, adverse reactions, and changes in liver function parameters after treatment, and the patients were followed up to observe tumor recurrence and survival. The t-test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups. The Kaplan-Meier method was used for survival analysis, and the log-rank test was used for comparison of survival curves. The Cox regression analysis was used to identify the independent risk factors for survival and prognosis. Results There was no significant difference in the response rate of initial ablation between the combination therapy group and the CRYO group (89.1% vs 73.9%, P > 0.05). There were no significant differences between the CRYO group and the combination therapy group in overall survival time and tumor-free survival rate after surgery (P > 0.05), and compared with the CRYO group, the combination therapy group had significantly lower 1-, 2-, and 3-year local tumor progression rates (20%/21%/21% vs 30%/46%/46%, χ2=4.187, P < 0.05). The multivariate Cox regression analysis showed that cryoablation alone might be an independent risk factor for local tumor progression(HR=2.206, 95%CI: 1.003-4.850, P=0.049). There was no significant difference in the incidence rate of adverse reactions between the two groups (P > 0.05), but 3 patients in the CRYO group experienced serious adverse reactions, while no patients in the combination therapy group experienced such reactions. Conclusion For elderly patients with early-stage hepatocellular carcinoma, cryoablation combined with PEI is safer and more effective than cryoablation alone and can significantly reduce local tumor progression rate. -
Key words:
- Carcinoma, Hepatocellalar /
- Catheter Ablation /
- Ethanol /
- Injections Intralesional
-
表 1 2组早期老年HCC患者临床特征比较
项目 CRYO组(n=46) 联合治疗组(n=46) 统计值 P值 年龄(岁) 73(70~83) 72(70~81) U=833.500 0.107 男/女(例) 34/12 34/12 χ2=0.000 1.000 BMI(kg/m2) 22.28±0.51 23.52±0.43 t=1.859 0.066 ECOG PS评分(例) χ2=2.841 0.092 0 8 15 1 38 31 病因学(例) χ2=0.066 0.797 HBV 37 36 HCV 9 10 Child-Pugh分级(例) χ2=0.123 0.726 A级 42 41 B级 4 5 AFP(μg/L) 15.39(5.25~39.90) 17.00(4.63~85.75) U=1 014.000 0.731 Alb(g/L) 37.00(35.00~40.00) 37.00(33.00~41.00) U=1 054.500 0.978 TBil(μmol/L) 13.20(9.70~17.30) 13.20(10.50~16.95) U=1 113.500 0.665 ALT(U/L) 18.00(14.50~44.50) 24.00(16.50~40.00) U=1 166.500 0.397 AST(U/L) 27.00(22.00~44.00) 35.00(25.00~51.50) U=1 210.500 0.233 PLT(×109/L) 123.00(79.00~156.50) 114.00(77.50~168.00) U=1 076.000 0.888 ALP(U/L) 92.00(77.00~105.50) 89.00(75.00~109.50) U=1 051.000 0.956 GGT(U/L) 38.00(23.50~80.50) 29.00(20.00~49.50) U=867.500 0.137 肿瘤最大直径(cm) 2.07±0.15 2.20±0.17 t=0.445 0.658 肿瘤数目(例) χ2=0.522 0.470 单发 33 36 多发 13 10 高危部位肿瘤(例) 36 34 χ2=0.239 0.625 合并基础疾病(例) 肝硬化 21 18 χ2=0.401 0.527 糖尿病 9 9 χ2=0.000 1.000 高血压 21 15 χ2=1.643 0.200 心血管疾病 7 3 χ2=1.795 0.180 既往抗病毒治疗(例) 19 23 χ2=0.701 0.402  下载: 导出CSV
下载: 导出CSV
表 2 2组患者的生存预后情况
项目 CRYO组(n=46) 联合治疗组(n=46) 统计值 P值 中位随访期(月) 57(44~60) 67(46~72) χ2=3.247 0.072 完全消融[例(%)] 34(73.9) 41(89.1) χ2=3.536 0.060 LTP[例(%)] χ2=4.187 0.041 1年 14(30) 9(20) 2年 21(46) 10(21) 3年 21(46) 10(21) TFS[例(%)] χ2=3.346 0.067 1年 26(58) 27(59) 3年 6(13) 16(34) 5年 2(5) 11(25) OS[例(%)] χ2=0.000 0.989 1年 45(97) 42(91) 3年 35(76) 26(68) 5年 25(55) 28(61)
下载: 导出CSV
表 3 影响患者LTP的Cox单因素回归分析
变量 HR(95%CI) P值 单一治疗方式 2.206(1.003~4.850) 0.049 Child-Pugh B级 0.629(0.149~2.645) 0.399 ECOG PS =1分 1.438(0.654~3.159) 0.245 男性 1.168(0.517~2.640) 0.739 年龄>75岁 1.052(0.466~2.375) 0.406 BMI>24 kg/m2 1.081(0.479~2.441) 0.831 HBsAg阳性 1.559(0.634~3.832) 0.282 抗-HCV阳性 1.678(0.584~4.822) 0.980 伴随合并症 1.014(0.489~2.101) 0.778 有门静脉高压 0.835(0.402~1.737) 0.251 规律抗病毒治疗 0.682(0.322~1.445) 0.522 高危部位肿瘤 0.600(0.229~1.574) 0.457 肿瘤直径>3 cm 0.918(0.350~2.409) 0.906 肿瘤数量>1个 1.031(0.456~2.329) 0.641 Alb>35 g/L 0.669(0.304~1.469) 0.863 TBil>17.1 μmol/L 1.383(0.629~3.038) 0.475 ALT>40 U/L 1.148(0.508~2.592) 0.441 ALP>150 U/L 1.314(0.397~4.345) 0.322 AFP>20 ng/mL 1.237(0.597~2.566) 0.315
下载: 导出CSV
表 4 影响患者TFS和OS的Cox单因素回归分析
变量 TFS OS HR(95%CI) P值 HR(95%CI) P值 单一治疗方式 1.529(0.958~2.441) 0.067 0.995(0.512~1.934) 0.989 Child-Pugh B级 1.289(0.639~2.603) 0.468 2.603(1.133~5.981) 0.019 ECOG PS =1分 0.617(0.371~1.024) 0.055 0.945(0.461~1.939) 0.878 男性 1.060(0.623~1.802) 0.827 1.082(0.509~2.302) 0.837 年龄>75岁 1.009(0.618~1.648) 0.970 1.075(0.528~2.189) 0.841 BMI>24 kg/m2 0.669(0.396~1.130) 0.123 1.767(0.896~3.482) 0.094 HBsAg阳性 1.804(0.986~3.300) 0.056 1.433(0.505~4.063) 0.494 抗-HCV阳性 0.661(0.370~1.182) 0.152 0.653(0.271~1.570) 0.335 伴随合并症 0.846(0.538~1.331) 0.461 0.791(0.407~1.538) 0.486 有门静脉高压 1.376(0.863~2.193) 0.170 1.397(0.722~2.703) 0.316 规律抗病毒治疗 0.920(0.584~1.449) 0.713 1.358(0.703~2.625) 0.358 高危部位肿瘤 0.773(0.450~1.329) 0.341 0.596(0.247~1.437) 0.242 肿瘤直径>3 cm 1.367(0.785~2.380) 0.258 2.041(0.978~4.260) 0.049 8 肿瘤数量>1个 1.501(0.904~2.493) 0.107 1.450(0.725~2.904) 0.289 Alb>35 g/L 1.191(0.754~1.881) 0.445 0.475(0.245~0.921) 0.024 TBil>17.1 μmol/L 1.405(0.839~2.352) 0.186 1.033(0.497~2.146) 0.931 ALT>40 U/L 0.855(0.507~1.443) 0.551 0.910(0.427~1.937) 0.805 ALP>150 U/L 0.900(0.411~1.972) 0.789 1.930(0.733~5.082) 0.173 AFP>20 ng/mL 1.183(0.750~1.867) 0.462 1.804(0.929~3.504) 0.076
下载: 导出CSV
-
[1] LI X, LIANG P. Current status and advances in ultrasound-guided thermal ablation for hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(3): 510-514. DOI: 10.3969/j.issn.1001-5256.2021.03.004.李鑫, 梁萍. 超声引导下肝癌热消融治疗的现状与进展[J]. 临床肝胆病杂志, 2021, 37(3): 510-514. DOI: 10.3969/j.issn.1001-5256.2021.03.004. [2] TOKUSHIGE K, HASHIMOTO E, HORIE Y, et al. Hepatocellular carcinoma based on cryptogenic liver disease: The most common non-viral hepatocellular carcinoma in patients aged over 80 years[J]. Hepatol Res, 2015, 45(4): 441-447. DOI: 10.1111/hepr.12372. [3] MIRICI-CAPPA F, GRAMENZI A, SANTI V, et al. Treatments for hepatocellular carcinoma in elderly patients are as effective as in younger patients: A 20-year multicentre experience[J]. Gut, 2010, 59(3): 387-396. DOI: 10.1136/gut.2009.194217. [4] ZHANG YX, ZHANG XH, YU XL, et al. Prognosis of microwave ablation for hepatocellular carcinoma: Does age make a difference?[J]. Int J Hyperthermia, 2020, 37(1): 688-695. DOI: 10.1080/02656736.2020.1778198. [5] ZHUO ET, ZHENG YC, FU GH, et al. Clinical effect of transcatheter arterial chemoembolization combined with percutaneous ethanol injection in elderly patients with primary liver cancer[J]. Chin J Gerontol, 2021, 41(14): 2956-2958. DOI: 10.3969/j.issn.1005-9202.2021.14.013.卓恩挺, 郑扬慈, 符国宏, 等. 肝动脉化疗栓塞术联合无水酒精消融术在老年原发性肝癌中的临床效果[J]. 中国老年学杂志, 2021, 41(14): 2956-2958. DOI: 10.3969/j.issn.1005-9202.2021.14.013. [6] LI Z, ZHANG K, LIN SM, et al. Radiofrequency ablation combined with percutaneous ethanol injection for hepatocellular carcinoma: a systematic review and meta-analysis[J]. Int J Hyperthermia, 2017, 33(3): 237-246. DOI: 10.1080/02656736.2016.1237681. [7] HUANG H, LIANG P, YU XL, et al. Safety assessment and therapeutic efficacy of percutaneous microwave ablation therapy combined with percutaneous ethanol injection for hepatocellular carcinoma adjacent to the gallbladder[J]. Int J Hyperthermia, 2015, 31(1): 40-47. DOI: 10.3109/02656736.2014.999017. [8] WANG XZ, WANG ZX, YANG YP. The value of cryoablation combined with percutaneous ethanol injection in the treatment of liver cancer[J]. Hebei Med J, 2012, 34(15): 2274-2276. DOI: 10.3969/j.issn.1002-7386.2012.15.014.王新真, 王忠新, 杨永平, 等. 氩氦刀冷冻消融联合无水乙醇注射在肝癌治疗中的价值[J]. 河北医药, 2012, 34(15): 2274-2276. DOI: 10.3969/j.issn.1002-7386.2012.15.014. [9] WANG C, WANG H, YANG W, et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma[J]. Hepatology, 2015, 61(5): 1579-1590. DOI: 10.1002/hep.27548. [10] WANG H, LITTRUP PJ, DUAN Y, et al. Thoracic masses treated with percutaneous cryotherapy: Initial experience with more than 200 procedures[J]. Radiology, 2005, 235(1): 289-298. DOI: 10.1148/radiol.2351030747. [11] DINDO D, DEMARTINES N, CLAVIEN PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey[J]. Ann Surg, 2004, 240(2): 205-213. DOI: 10.1097/01.sla.0000133083.54934.ae. [12] AHMED M, SOLBIATI L, BRACE CL, et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria--a 10-year update[J]. Radiology, 2014, 273(1): 241-260. DOI: 10.1148/radiol.14132958. [13] KUDO M. Recent advances in systemic therapy for hepatocellular carcinoma in an aging society: 2020 update[J]. Liver Cancer, 2020, 9(6): 640-662. DOI: 10.1159/000511001. [14] European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma[J]. J Hepatol, 2018, 69(1): 182-236. DOI: 10.1016/j.jhep.2018.03.019. [15] RHO SY, LEE HW, KIM DY, et al. Current status of therapeutic choice and feasibility for patients with hepatocellular carcinoma aged ≥ 70 years: A nationwide cancer registry analysis[J]. J Hepatocell Carcinoma, 2021, 8: 321-332. DOI: 10.2147/JHC.S306507. [16] GALUN D, BOGDANOVIC A, ZIVANOVIC M, et al. Short- and long-term outcomes after hepatectomy in elderly patients with hepatocellular carcinoma: An analysis of 229 cases from a developing country[J]. J Hepatocell Carcinoma, 2021, 8: 155-165. DOI: 10.2147/JHC.S297296. [17] KIM JM, CHO BI, KWON CH, et al. Hepatectomy is a reasonable option for older patients with hepatocellular carcinoma[J]. Am J Surg, 2015, 209(2): 391-397. DOI: 10.1016/j.amjsurg.2013.06.010. [18] YU B, DING Y, LIAO X, et al. Radiofrequency ablation versus surgical resection in elderly patients with early-stage hepatocellular carcinoma in the era of organ shortage[J]. Saudi J Gastroenterol, 2018, 24(6): 317-325. DOI: 10.4103/sjg.SJG_261_18. [19] EI S, HIBI T, TANABE M, et al. Cryoablation provides superior local control of primary hepatocellular carcinomas of > 2 cm compared with radiofrequency ablation and microwave coagulation therapy: An underestimated tool in the toolbox[J]. Ann Surg Oncol, 2015, 22(4): 1294-1300. DOI: 10.1245/s10434-014-4114-7. [20] DUNNE RM, SHYN PB, SUNG JC, et al. Percutaneous treatment of hepatocellular carcinoma in patients with cirrhosis: A comparison of the safety of cryoablation and radiofrequency ablation[J]. Eur J Radiol, 2014, 83(4): 632-638. DOI: 10.1016/j.ejrad.2014.01.007. [21] SATO M, TATEISHI R, YASUNAGA H, et al. Mortality and morbidity of hepatectomy, radiofrequency ablation, and embolization for hepatocellular carcinoma: A national survey of 54, 145 patients[J]. J Gastroenterol, 2012, 47(10): 1125-1133. DOI: 10.1007/s00535-012-0569-0. [22] SHⅡNA S, TATEISHI R, ARANO T, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors[J]. Am J Gastroenterol, 2012, 107(4): 569-577; quiz 578. DOI: 10.1038/ajg.2011.425. [23] LI Z, ZHANG C, LOU C, et al. Comparison of percutaneous cryosurgery and surgical resection for the treatment of small hepatocellular carcinoma[J]. Oncol Lett, 2013, 6(1): 239-245. DOI: 10.3892/ol.2013.1314. [24] ORLACCHIO A, BAZZOCCHI G, PASTORELLI D, et al. Percutaneous cryoablation of small hepatocellular carcinoma with US guidance and CT monitoring: initial experience[J]. Cardiovasc Intervent Radiol, 2008, 31(3): 587-594. DOI: 10.1007/s00270-008-9293-9. [25] TAKAHASHI H, MIZUTA T, KAWAZOE S, et al. Efficacy and safety of radiofrequency ablation for elderly hepatocellular carcinoma patients[J]. Hepatol Res, 2010, 40(10): 997-1005. DOI: 10.1111/j.1872-034X.2010.00713.x. [26] KAIBORI M, YOSHⅡ K, HASEGAWA K, et al. Treatment optimization for hepatocellular carcinoma in elderly patients in a Japanese Nationwide Cohort[J]. Ann Surg, 2019, 270(1): 121-130. DOI: 10.1097/SLA.0000000000002751. [27] HINSHAW JL, LEE FT Jr. Cryoablation for liver cancer[J]. Tech Vasc Interv Radiol, 2007, 10(1): 47-57. DOI: 10.1053/j.tvir.2007.08.005. [28] VANDENBROUCKE F, VANDEMEULEBROUCKE J, BULS N, et al. Can tumor coverage evaluated 24 h post-radiofrequency ablation predict local tumor progression of liver metastases?[J]. Int J Comput Assist Radiol Surg, 2018, 13(12): 1981-1989. DOI: 10.1007/s11548-018-1765-z. 期刊类型引用(16)
1. 余文君,余婷婷,李丽华,王红英,普冬,杨永锐. 血清生物标志物在慢性HBV感染自然史诊断中应用的研究进展. 医学理论与实践. 2025(03): 395-398 .  百度学术
百度学术2. 余文君,余婷婷,李丽华,王红英,普冬. 血清标志物在慢性HBV感染自然史中的诊断价值研究. 大理大学学报. 2025(02): 67-74 . 百度学术3. 牛梦铱,杜建新,刘桂玲. 肝纤维化指标、外周血常规指标和GPR对重度慢性乙型肝炎的诊断价值及其相关性分析. 检验医学与临床. 2024(02): 178-182 . 百度学术4. 陈媛,徐晶,谌翠容,孙振江,周婧玮. 乙型病毒性肝炎肝硬化患者血清cTNT、LPS水平、FIB-4指数与幽门螺杆菌感染的关系. 中华医院感染学杂志. 2024(07): 998-1001 . 百度学术5. 吴旭光,马立华,占国祥,黄志刚. 无创炎症诊断模型在非酒精性脂肪性肝病合并乙型肝炎病毒感染患者肝纤维化诊断中的应用. 中国医师杂志. 2024(02): 245-249 . 百度学术6. 赖长祥,唐情容,张秀连,唐奇远,李知玉,周旋,冼文杰,陈瑞坤,吴晓娟,王方. 年龄≤30岁慢性HBV感染者启动抗病毒治疗无创预测模型的构建及分析. 临床肝胆病杂志. 2024(07): 1328-1333 .  本站查看
本站查看7. 姚建锋,陈正雷,张煜华. 实时二维超声剪切波弹性成像在慢性乙型肝炎肝纤维化分期中的临床应用. 罕少疾病杂志. 2024(10): 54-56 . 百度学术8. 李晓宇,黄秀香,叶迎宾. 血清壳多糖酶3样蛋白1和PLT的比值与FIB-4指数在慢性乙型肝炎轻、中度诊断效价的比较. 标记免疫分析与临床. 2024(09): 1693-1697 . 百度学术9. 刘雅茹,胡义扬,赵瑜. 基于证候积分的慢性乙型肝炎湿热证的中西医临床特征. 世界中医药. 2024(22): 3523-3530 . 百度学术10. 曾伟梅,董常峰,黄琨,郑保奇,李志艳,冯程,陈昕,刘忠. 声触诊弹性成像线性结合超声评分细分慢性乙肝患者肝纤维化程度. 中华超声影像学杂志. 2023(02): 129-135 . 百度学术11. 王娟霞,陈馨悦,魏世博,孙新策,朱浩宇,连唐悠悠,杜雨峰. 慢性乙型肝炎患者肝脏炎症程度预测模型的研究. 中国实用内科杂志. 2023(05): 390-395 . 百度学术12. 梁紫茵,周伟泽,黄秀明,邓振雄,利旭辉. 分析基于4项因素的肝纤维化指数值动态变化对恩替卡韦治疗慢性乙型肝炎肝硬化病人患肝癌风险的预测价值. 安徽医药. 2023(06): 1211-1216 . 百度学术13. 宋艺佳,刘素彤,张丽慧,赵文霞,刘鸣昊. 无创诊断与代偿期乙型肝炎肝硬化患者中医证型的相关性分析. 中西医结合肝病杂志. 2023(11): 981-985 . 百度学术14. 贾梦山,刘加敏,杨艳霞. 血清Galectin-9和PD-L1对慢性乙型肝炎肝脏炎症程度的诊断价值. 分子诊断与治疗杂志. 2022(08): 1354-1357+1362 . 百度学术15. 宣佳利. 维生素D对妊娠期高血压大鼠肝脏的保护作用及机制. 牡丹江医学院学报. 2022(05): 10-13 . 百度学术16. 黄亮,郑世燕. LSM值、APRI、FIB-4、肝脏病理对肝病诊断运用价值. 中国当代医药. 2022(32): 46-48+57 . 百度学术其他类型引用(8)
-





 百度学术
百度学术

