
 PDF下载 ( 2480 KB)
PDF下载 ( 2480 KB)

肝肌信号强度比及血清标志物对慢性乙型肝炎肝纤维化的诊断价值
DOI: 10.3969/j.issn.1001-5256.2023.03.014
Value of liver-muscle signal intensity and serum markers in diagnosis of chronic hepatitis B liver fibrosis
-
摘要:
目的 结合ALT和肝脏硬度值水平分组,探讨磁敏感加权成像(SWI)的肝肌信号强度比(LMR)及血清标志物诊断慢性乙型肝炎纤维化严重程度的价值。 方法 回顾性收集2018年10月—2021年9月就诊于延安大学附属医院的慢性乙型肝炎患者255例,将患者分为严重肝纤维化(SLF)组77例与非SLF组178例,SLF组定义为ALT水平在正常范围内且肝脏硬度大于9.0 kPa,或ALT水平高于正常值上限1~5倍且肝脏硬度大于12.0 kPa的患者。在SWI序列下测量肝脏的平均SWI值(SWIliver)及竖脊肌信号强度并计算LMR。正态分布的计量资料2组间比较采用t检验,非正态分布的计量资料2组间比较采用Mann-Whitney U检验。计数资料组间比较采用χ2检验。利用二元Logistic回归分析SLF的影响因素。采用受试者工作特征(ROC)曲线分析LMR及其联合血清学的诊断效能,使用DeLong检验比较不同AUC的差异。 结果 SLF组较非SLF组的ALT(Z=-3.569, P<0.001)、AST(Z=-5.495, P<0.001)、透明质酸(HA)(Z=-6.746, P<0.001)、层粘连蛋白(LN)(Z=-5.459, P<0.001)、Ⅳ型胶原(Ⅳ-C)(Z=-8.470, P<0.001)、Ⅲ型前胶原(PCⅢ)(Z=-6.326, P<0.001)、APRI(Z=-9.004, P<0.001)、FIB-4(Z=-8.357, P<0.001) 高,较非SLF组的PTA(t=10.088, P<0.001)、PLT(t=9.163, P<0.001)、SWIliver(t=2.347, P=0.02)、LMR× 10(Z=-4.447, P<0.001)低。PTA、HA、Ⅳ-C、LMR×10为发生SLF的独立影响因素(P值均<0.05)。LMR×10诊断SLF的ROC曲线下面积(AUC)为0.675(95%CI: 0.614~0.732), 高于SWIliver的0.594(95%CI: 0.531~0.655)(Z=3.984, P<0.001),PTA+HA+Ⅳ-C+LMR×10(AUC=0.937, 95%CI: 0.896~0.966)的诊断效能优于PTA+HA+Ⅳ-C(AUC=0.905, 95%CI: 0.858~0.941)(Z=2.228, P=0.026)。 结论 LMR及血清标志物可较准确区分SLF,LMR为一项定量、客观的影像学指标,优于SWIliver,并可提升血清学标志物对临床判定SLF的诊断效能。 Abstract:Objective To investigate the value of liver/muscle ratio (LMR) on susceptibility-weighted imaging (SWI) and serum markers in the diagnosis of the severity of chronic hepatitis B liver fibrosis after grouping based on alanine aminotransferase (ALT) level. Methods A retrospective analysis was performed for 255 patients with chronic hepatitis B who attended Affiliated Hospital of Yan'an University from October 2018 to September 2021, and the patients were divided into severe liver fibrosis group (SLF group) and non-severe liver fibrosis group (non-SLF group). The SLF group was defined as liver stiffness measurement (LSM) > 9.0 kPa and ALT level within the normal range or LSM > 12.0 kPa and ALT level greater than 1-5 times of the upper limit of normal. LMR was calculated by measuring the mean SWI value of the liver (SWIliver) and the signal intensity of the erector spinae. The t-test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two group; the chi-square test was used for comparison of categorical data between two groups. The binary logistic regression analysis was used to investigate the influencing factors for SLF. The receiver operating characteristic (ROC) curve was used to analyze the diagnostic performance of LMR and its combination with serum markers, and the DeLong test was used to compare the difference in the area under the ROC curve (AUC). Results Compared with the non-SLF group, the SLF group had significantly higher ALT (Z=-3.569, P < 0.001), aspartate aminotransferase (AST) (Z=-5.495, P < 0.001), hyaluronic acid (HA) (Z=-6.746, P < 0.001), laminin (LN) (Z=-5.459, P < 0.001), type Ⅳ collagen (Ⅳ-C)(Z=-8.470, P < 0.001), type Ⅲ procollagen (PCⅢ) (Z=-6.326, P < 0.001), aspartate aminotransferase-to-platelet ratio index (Z=-9.004, P < 0.001), and FIB-4 (Z=-8.357, P < 0.001) and significantly lower prothrombin time activity (PTA) (t=10.088, P < 0.001), platelet count (t=9.163, P < 0.001), SWIliver (t=2.347, P=0.02), and LMR×10 (Z=-4.447, P < 0.001). PTA, HA, Ⅳ-C, and LMR×10 were independent influencing factors for SLF. LMR×10 had an AUC of 0.675 (95% confidence interval [CI]: 0.614-0.732) in the diagnosis of SLF, which was significantly higher than that of SWIliver (AUC=0.594, 95%CI: 0.531-0.655) (Z=3.984, P < 0.001). PTA+HA+Ⅳ-C+LMR×10 and PTA+HA+Ⅳ-C had an AUC of 0.937 (95%CI: 0.896-0.966) and 0.905 (95%CI: 0.858-0.941), respectively, suggesting that PTA+HA+Ⅳ-C+LMR×10 had a better diagnostic performance than PTA+HA+Ⅳ-C (Z=2.228, P=0.026). Conclusion LMR and serum markers can accurately distinguish SLF after grouping based on ALT level. LMR is a quantitative and objective imaging indicator and is better than SWIliver, and it can also improve the diagnostic performance of serum markers for SLF in clinical practice. -
Key words:
- Hepatitis B, Chronic /
- Liver Cirrhosis /
- Magnetic Resonance Imaging /
- Biomarkers /
- Liver Muscle Ratio /
- Diagnosis
-

注:a,1例慢性乙型肝炎SLF患者,男性32岁,LMR×10为5.11,ALT为86 U/L,LSM为14 kPa。b,1例慢性乙型肝炎非SLF患者,男性55岁,LMR×10为8.87,ALT为33 U/L,LSM为8.5 kPa。
图 1 LMR测量示例图
Figure 1. Sample figure of LMR measurements
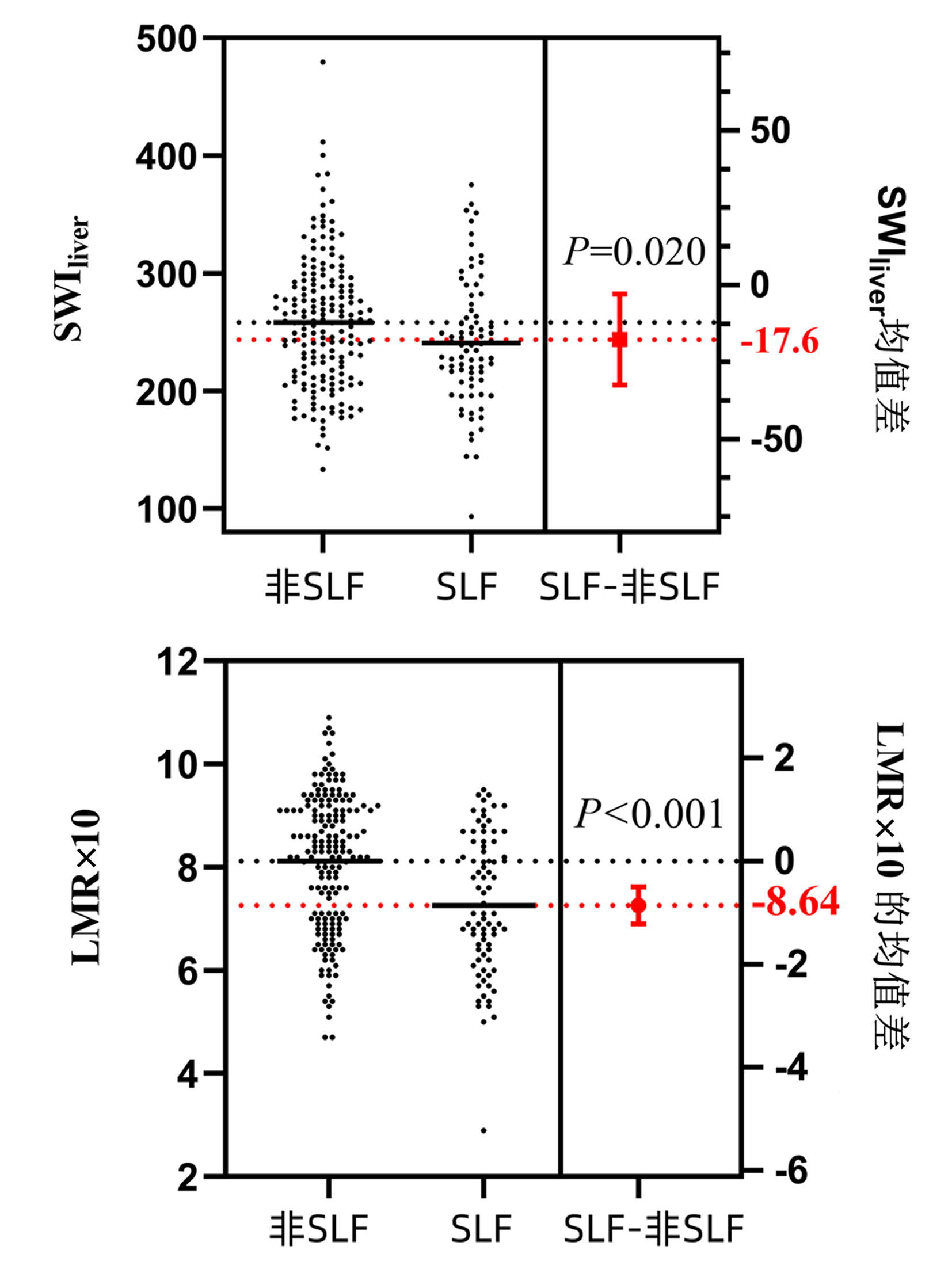
图 2 不同程度纤维化SWIliver、LMR的均值差异
Figure 2. Estimation plot of SWIliver and LMR for different degree of fibrosis
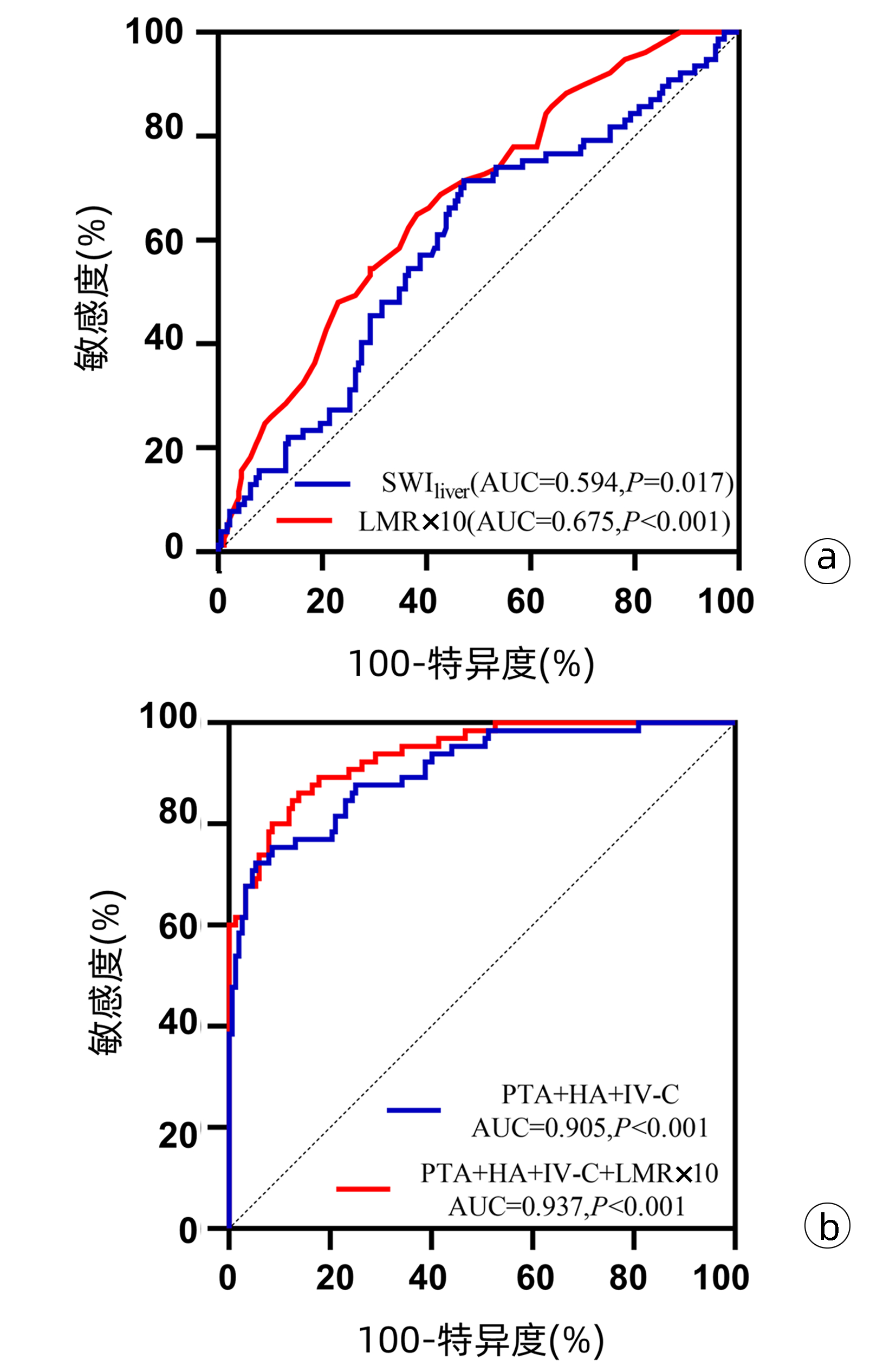
注:a,SWIliver与LMR×10的ROC曲线;b,联合PTA、HA、Ⅳ-C与联合PTA、HA、Ⅳ-C、LMR×10的ROC曲线。
图 3 MRI参数及血清学诊断SLF的ROC曲线
Figure 3. ROC curve of MRI parameters and serology in the diagnosis of SLF
表 1 不同程度纤维化患者基本特征、血清学及影像学特征比较
Table 1. Comparison of basic features, serological and imaging features of different degrees of fibrosis
项目 非SLF组(n=178) SLF组(n=77) 统计值 P值 男性[例(%)] 108(60.67) 45(58.44) χ2=0.112 0.738 年龄(岁) 47.40±11.19 50.12±10.56 t=-1.810 0.070 BMI(kg/m2) 24.02±2.94 23.49±3.98 t=1.162 0.247 PTA(%) 90.43±14.57 70.18±14.56 t=10.088 <0.001 PLT(×109/L) 175.50±65.81 94.66±61.97 t=9.163 <0.001 ALT(U/L) 22.0(16.0~34.3) 32.0(22.0~46.5) Z=-3.569 <0.001 AST(U/L) 23.0(19.0~30.0) 34.0(25.5~44.0) Z=-5.495 <0.001 HA(ng/mL) 116.90(72.45~182.60) 263.42(136.15~427.72) Z=-6.746 <0.001 LN(ng/mL) 69.64 (53.25~84.39) 99.16(73.84~147.48) Z=-5.459 <0.001 Ⅳ-C(S/CO) 42.05(28.69~58.67) 91.99(64.64~131.93) Z=-8.470 <0.001 PCⅢ(ng/mL) 6.28(4.08~8.75) 10.18(6.97~14.27) Z=-6.326 <0.001 LSM(kPa) 5.60(4.50~6.93) 16.20(11.85~21.30) Z=-12.543 <0.001 SWIliver 258.45±55.24 240.84±54.47 t=2.347 0.020 LMR×10 8.30(7.00~9.13) 7.10(6.25~8.50) Z=-4.447 <0.001 APRI 0.40(0.29~0.60) 1.12(0.73~1.97) Z=-9.004 <0.001 FIB-4 1.42(0.96~2.13) 3.70(2.16~7.19) Z=-8.357 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 二元Logistic回归分析SLF的影响因素
Table 2. Binary Logistic regression analysis of SLF
变量 B值 SE Wald OR(95%CI) P值 PTA -0.069 0.021 10.251 0.93(0.90~0.97) 0.001 HA 0.007 0.002 13.262 1.01(1.00~1.01) <0.001 Ⅳ-C 0.036 0.036 15.115 1.04(1.02~1.06) <0.001 LMR×10 -0.949 0.219 18.867 0.39(0.25~0.59) <0.001
下载: 导出CSV
表 3 MRI参数及血清学诊断SLF的效能
Table 3. Efficacy of MRI parameters and serology in the diagnosis of SLF
参数 AUC 95%CI 最佳截断值 敏感度(%) 特异度(%) Z值 P值 SWIliver 0.594 0.531~0.655 257.43 71.43 52.81 2.396 0.017 LMR×10 0.675 0.614~0.732 0.79 64.94 61.80 4.918 <0.001 PTA+HA+Ⅳ-C 0.905 0.858~0.941 0.39 72.31 94.74 17.840 <0.001 PTA+HA+Ⅳ-C+LMR×10 0.937 0.896~0.966 0.28 86.15 86.18 26.161 <0.001
下载: 导出CSV
-
[1] Chinese Society of Infectious Diseases, Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [2] SHIHA G, IBRAHIM A, HELMY A, et al. Asian-Pacific Association for the Study of the Liver (APASL) consensus guidelines on invasive and non-invasive assessment of hepatic fibrosis: a 2016 update[J]. Hepatol Int, 2017, 11(1): 1-30. DOI: 10.1007/s12072-016-9760-3. [3] Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Infectious Diseases, Chinese Medical Association. Consensus on the diagnosis and therapy of hepatic fibrosis(2019)[J]. J Clin Hepatol, 2019, 35(10): 2163-2172. DOI: 10.3969/j.issn.1001-5256.2019.10.007.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会感染病学分会. 肝纤维化诊断及治疗共识(2019年)[J]. 临床肝胆病杂志, 2019, 35(10): 2163-2172. DOI: 10.3969/j.issn.1001-5256.2019.10.007. [4] European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis[J]. J Hepatol, 2015, 63(1): 237-264. DOI: 10.1016/j.jhep.2015.04.006. [5] WANG L, ZHU M, CAO L, et al. Liver stiffness measurement can reflect the active liver necroinflammation in population with chronic liver disease: a real-world evidence study[J]. J Clin Transl Hepatol, 2019, 7(4): 313-321. DOI: 10.14218/JCTH.2019.00040. [6] HUANG LL, YU XP, LI JL, et al. Effect of liver inflammation on accuracy of FibroScan device in assessing liver fibrosis stage in patients with chronic hepatitis B virus infection[J]. World J Gastroenterol, 2021, 27(7): 641-653. DOI: 10.3748/wjg.v27.i7.641. [7] SETO WK, HUI R, MAK LY, et al. Association between hepatic steatosis, measured by controlled attenuation parameter, and fibrosis burden in chronic hepatitis B[J]. Clin Gastroenterol Hepatol, 2018, 16(4): 575-583.e2. DOI: 10.1016/j.cgh.2017.09.044. [8] CHENG Y, GUO R, LIU MG, et al. Value of MRI and quantitative serological markers detection to the diagnosis of liver fibrosis[J]. J Chin Pract Diagn Ther, 2018, 32 (6): 589-593. DOI: 10.13507/j.ssn.1674-3474.2018.06.021.程渝, 郭锐, 刘明国, 等. MRI与血清学定量指标检测对肝纤维化的诊断价值[J]. 中华实用诊断与治疗杂志, 2018, 32(6): 589-593. DOI: 10.13507/j.issn.1674-3474.2018.06.021. [9] Chinese Society of Infectious Diseases, Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [10] CHENG DY, LI B, JI SJ, et al. Application of transient elastography in noninvasive diagnosis of liver fibrosis[J/CD]. Chin J Liver Dis (Electronic Version), 2021, 13(4): 9-13. DOI: 10.3969/j.issn.1674-7380.2021.04.003 .程丹颖, 李贲, 纪世博, 等. 瞬时弹性成像技术在肝纤维化无创诊断中的应用[J/CD]. 中国肝脏病杂志(电子版), 2021, 13(4): 9-13. DOI:10.3969/j.issn.1674-7380.2021.04.003 .[11] OBMANN VC, MARX C, BERZIGOTTI A, et al. Liver MRI susceptibility-weighted imaging (SWI) compared to T2* mapping in the presence of steatosis and fibrosis[J]. Eur J Radiol, 2019, 118: 66-74. DOI: 10.1016/j.ejrad.2019.07.001. [12] JIANG JZ, DENG LB, RUAN JY, et al. Value of susceptibility weighted imaging in hepatic fibrosis staging by using MR in a rabbit model[J]. J Chin Med, 2016, 96(17): 1371-1376. DOI: 10.3760/cma.j.issn.0376-2491.2016.17.015江锦赵, 邓灵波, 阮继银, 等. 磁敏感加权成像在兔肝脏纤维化模型分期中的诊断价值[J]. 中华医学杂志, 2016, 96(17): 1371-1376. DOI: 10.3760/cma.j.issn.0376-2491.2016.17.015. [13] GANDON Y, OLIVIÉ D, GUYADER D, et al. Non-invasive assessment of hepatic iron stores by MRI[J]. Lancet, 2004, 363(9406): 357-362. DOI: 10.1016/S0140-6736(04)15436-6. [14] BALASSY C, FEIER D, PECK-RADOSAVLJEVIC M, et al. Susceptibility-weighted MR imaging in the grading of liver fibrosis: a feasibility study[J]. Radiology, 2014, 270(1): 149-158. DOI: 10.1148/radiol.13122440. [15] SHI DD, GUO R, LIU YH, et al. The value of gadoxetate disodium enhanced MRI in the quantitative assessment of liver fibrosis[J]. Chin J Radio, 2022, 56(3): 273-278. DOI: 10.3760/cma.j.cn112149-20210316-00236.师丹丹, 郭然, 刘月华, 等. 钆塞酸二钠增强MRI定量评估肝纤维化的价值[J]. 中华放射学杂志, 2022, 56(3): 273-278. DOI: 10.3760/cma.j.cn112149-20210316-00236. [16] LI GP, ZHANG HX, ZHANG L, et al. HA, Ⅳ-C, APRI and Fib-4 for diagnosis of liver fibrosis effect after hepatitis B[J]. J Clin Exp Med, 2021, 20(13): 1385-1388. https://www.cnki.com.cn/Article/CJFDTOTAL-SYLC202113011.htm李广平, 张红心, 张蕾, 等. 透明质酸、Ⅳ型胶原、APRI及纤维蛋白原-4对乙型肝炎后肝纤维化的诊断价值[J]. 临床和实验医学杂志, 2021, 20(13): 1385-1388. https://www.cnki.com.cn/Article/CJFDTOTAL-SYLC202113011.htm [17] YANG XZ, GEN AW, XIAN JC, et al. Diagnostic value of various noninvasive indexes in the diagnosis of chronic hepatic fibrosis[J]. Eur Rev Med Pharmacol Sci, 2018, 22(2): 479-485. DOI: 10.26355/eurrev_201801_14198. -



