
表
1
纳入患者分组情况及基线资料
| 组别 | 例数 | 男 | 女 | 年龄(岁) |
| HBeAg(+)、HBV DNA(+) | 22 | 13 | 9 | 35.36±7.55 |
| HBeAg(+)、HBV DNA(-) | 17 | 11 | 6 | 39.35±7.98 |
| HBeAg(-)、HBV DNA(-) | 22 | 13 | 9 | 45.00±11.16 |
全球有超过2.4亿慢性HBV感染者,若不及时进行有效、规范的治疗,15%~40%的患者会进展为肝硬化,最终导致肝衰竭和肝细胞癌(HCC)[1]。虽然乙型肝炎疫苗的接种使HBV感染的患病率逐年下降,但多数亚洲地区仍归为中至高流行区。我国HBsAg流行率为5%~6%,但因为人口基数大,所以仍存在许多的慢性HBV感染者,其中需要治疗的慢性乙型肝炎(CHB)患者约有2000万~3000万[2-3];因此慢性HBV感染依然是我国的重大公共卫生问题。当前用于抗病毒治疗的核苷(酸)类似物(nucleos(t)ide analogues, NAs)虽可有效抑制病毒复制,延缓疾病进展,但对肝细胞核内的共价闭合环状DNA(covalently closed circular DNA,cccDNA)均无明确作用,使得病毒无法完全清除。cccDNA作为HBV复制的原始模板,检测肝内cccDNA水平是评价抗病毒疗效及停止治疗的重要指标[4-5],由于肝活检为侵入性操作,cccDNA在肝组织内分布不均,松弛环状双链DNA(relaxed circularDNA,rcDNA)的存在影响cccDNA含量等因素导致cccDNA检测难以在临床广泛开展[6-7]。因此需要寻找能反映肝内cccDNA活性且方便操作的临床替代指标。近年来HBV RNA作为新的血清学标志物被广泛提出,因为其只能来自肝内cccDNA, 所以能更好的反映HBV转录活性,本研究主要探讨血清HBV RNA在HBeAg阳性CHB患者不同时期的表达水平及检测价值。
收集2019年8月—2020年12月在杭州市西溪医院肝病科门诊及住院部诊治的CHB患者,纳入标准:(1)诊断符合《慢性乙型肝炎防治指南(2019年版)》[8];(2)准备接受或已接受NAs抗病毒治疗。排除标准:(1)合并HAV、HCV、巨细胞病毒等其他嗜肝病毒感染;(2)合并HIV感染;(3)HCC患者;(4)代谢性肝病、自身免疫性肝病及近期使用肝损伤性药物者;(5)合并其他系统恶性肿瘤或严重疾病者;(6)研究者认为不适合入组的其他情况。
本研究使用的HBV RNA定量检测试剂盒由湖南圣湘科技有限公司提供,检测原理通过逆转录HBV核酸中的pgRNA(经DNA酶消化),利用针对HBV pgRNA序列设计的一组特异性引物与荧光探针,配以PCR反应液,在荧光定量PCR仪上,应用一步法RT实时荧光定量PCR检测技术,通过荧光信号的变化实现HBV pgRNA的定量检测,HBV RNA检测下限为50拷贝/mL。应用化学发光免疫分析法在美国雅培Alinity i全自动化学发光免疫分析仪上行HBV血清学标志物检测;用HBV DNA定量检测试剂盒,在ABI7500荧光定量PCR仪上行HBV DNA检测;HBV DNA检测下限为30 IU/mL;用Beckman Coulter AU5831全自动生化分析仪检测ALT(正常范围9~50 U/L)、AST(正常范围15~40 U/L)。
本研究经杭州市西溪医院伦理委员会批准, 批号:2019年(科)伦审第21号,所有患者均签署知情同意书。
采用SPSS 25.0进行统计学处理,正态分布的计量资料用x ±s表示,2组间比较采用独立样本t检验;非正态分布的计量资料用M(P25~P75)表示,2组间比较采用Mann-Whitney U检验;计数资料组间比较采用χ2检验;采用Pearson或Spearman相关分析描述两变量间的相关性。P<0.05为差异有统计学意义。
本研究共纳入61例CHB患者,平均年龄(39.95±9.88)岁。按HBeAg及HBV DNA状态分为3组:HBeAg阳性CHB[HBeAg(+)、HBV DNA(+)]未治患者,HBeAg血清学转换前[HBeAg(+)、HBV DNA(-)]经治患者,HBeAg血清学转换后[HBeAg(-)、HBV DNA(-)]经治患者(表 1)。
| 组别 | 例数 | 男 | 女 | 年龄(岁) |
| HBeAg(+)、HBV DNA(+) | 22 | 13 | 9 | 35.36±7.55 |
| HBeAg(+)、HBV DNA(-) | 17 | 11 | 6 | 39.35±7.98 |
| HBeAg(-)、HBV DNA(-) | 22 | 13 | 9 | 45.00±11.16 |
HBeAg阳性CHB未治患者血清HBV RNA阳性率100%(22/22),HBV RNA载量最大值为9 log10拷贝/mL,平均为7 log10拷贝/mL;HBeAg血清学转换前经治患者血清HBV RNA阳性率88.2%(15/17),HBV RNA载量最大值为5 log10拷贝/mL,平均4 log10拷贝/mL;HBeAg血清学转换后经治患者血清HBV RNA阳性率22.7%(6/22),HBV RNA载量最大值为4 log10拷贝/mL。
经治HBeAg阳性组的HBV RNA阳性率显著高于HBeAg阴性组,差异有统计学意义(P<0.001), 2组间HBV RNA、HBsAg水平比较,差异均有统计学意义(P值均<0.05)(表 2)。
| 项目 | HBeAg阳性组(n=17) | HBeAg阴性组(n=22) | 统计值 | P值 |
| 男/女(例) | 11/6 | 13/9 | 0.753 | |
| 年龄(岁) | 39.35±7.98 | 45.00±11.16 | t=-1.77 | 0.086 |
| HBV RNA阳性[例(%)] | 15(88.2) | 6(27.3) | <0.001 | |
| HBV RNA(log10拷贝/mL) | 4.05(3.01~5.18) | 1.40(1.40~1.83) | Z=-4.44 | <0.001 |
| HBsAg(log10IU/mL) | 3.24(2.86~3.50) | 2.76(2.07~3.35) | Z=-2.41 | 0.016 |
| ALT(U/L) | 22.24±10.83 | 25.09±11.76 | t=-0.78 | 0.442 |
| AST(U/L) | 23.00±4.48 | 23.9±14.23 | t=-0.65 | 0.521 |
CHB患者NAs治疗实现HBV DNA阴转时,肝功能复常,ALT、AST水平降低,HBV RNA、HBsAg水平也均有所降低(P值均<0.001)(表 3)。对于治疗后HBV DNA阴转的CHB患者,Spearman相关分析示,血清HBV RNA与血清HBsAg无相关性(P=0.091)。
| 项目 | HBV DNA阳性组(n=22) | HBV DNA阴性组(n=39) | 统计值 | P值 |
| 男/女(例) | 13/9 | 24/15 | χ2=0.035 | 0.851 |
| 年龄(岁) | 35.36±7.55 | 42.54±10.18 | t=-2.88 | 0.005 |
| HBV RNA(log10拷贝/mL) | 7.62(6.51~8.55) | 1.94(1.40~4.04) | Z=-6.16 | <0.001 |
| HBsAg(log10IU/mL) | 3.94(3.26~4.23) | 2.90(2.61~3.44) | Z=-4.07 | <0.001 |
| ALT(U/L) | 249.50(114.25~664.50) | 20.00(16.00~31.00) | Z=-6.45 | <0.001 |
| AST(U/L) | 106.00(63.75~418.75) | 23.00(21.00~27.00) | Z=-6.45 | <0.001 |
| HBV DNA(log10IU/ml) | 7.21±1.23 | - |
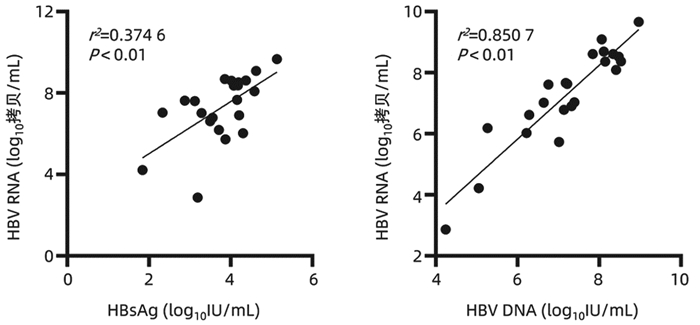
在HBeAg阳性CHB未治患者中,HBV RNA与HBsAg(r=0.612,P<0.01)、HBV DNA(r=0.922, P<0.01)均具有较强的相关性(图 1);在HBeAg血清学转换前和HBeAg血清学转换后的经治患者中,HBV RNA与HBsAg无相关性(P>0.05);3组患者HBV RNA与年龄、ALT、AST均无相关性(P值均>0.05)。
CHB是导致肝硬化、肝衰竭、HCC的主要危险因素,每年约有80万人死于HBV感染相关性疾病[9],因此如何有效的管理CHB患者仍是当前临床工作的热点和难点。随着对HBV RNA的研究深入,已知HBV感染患者血清中的HBV RNA就是前基因组RNA(pgRNA),即3.5 kb mRNA;pgRNA是HBV复制的中间产物,利用cccDNA作为模板在病毒核衣壳内转录,最后释放完整的子代病毒,因此血清HBV RNA与HBsAg不同,其只能来自于肝内cccDNA;而NAs是通过取代HBV复制过程中聚合酶区的核苷来抑制病毒复制,并不能影响cccDNA转录生成mRNA,由此可以推断HBV RNA与肝内cccDNA相关,检测外周血HBV RNA水平可以反映肝内cccDNA的转录活性。因此相比于HBsAg、HBV DNA等传统的血清学指标,血清HBV RNA水平可以更好的反映肝内病毒复制水平,其能作为CHB患者管理的新型标志物[10-11]。
HBeAg阳性CHB患者在接受抗病毒药物治疗后会逐步实现HBV DNA阴转、HBeAg血清学转换等目标,本研究通过观察HBeAg阳性的CHB患者不同时期的HBV RNA表达水平,发现未治疗的22例CHB患者血清中均能检测出较高的血清HBV RNA水平;39例治疗后HBV DNA阴转的CHB患者中仍有21例可以检测出HBV RNA,这表明在评估病毒复制方面HBV RNA比HBV DNA更灵敏,即使是在HBV DNA持续低于检测下限且发生HBeAg血清学转换也有部分患者血清HBV RNA阳性,意味HBeAg的消失只能表示病毒复制减弱,肝内cccDNA仍可能存在低水平的转录。
对HBeAg阳性CHB患者而言,发生HBeAg血清学转换是比较满意的终点,是发生HBsAg阴转的基本条件。本文通过比较治疗后HBV DNA阴转的HBeAg阳性组与HBeAg阴性组,发现HBeAg阳性组HBV RNA阳性率显著高于HBeAg阴性组(88.2% vs 27.3%),两组间HBV RNA、HBsAg水平差异也具有统计学意义,因HBV RNA只能来自于肝内cccDNA, 提示HBeAg阳性CHB患者肝内cccDNA转录活性更高。因此临床上对HBeAg阳性的CHB患者要努力实现HBeAg血清学转换。
通过分析HBV DNA阳性组与HBV DNA阴性组患者,发现接受NAs治疗后HBV DNA、HBV RNA均会发生下降,这是因为NAs类药物抑制pgRNA的逆转录,致使DNA合成受阻,而长时间接受NAs治疗使rcDNA的形成受到抑制,影响cccDNA池的回补,被感染的肝细胞数量减少,进一步导致HBV RNA的生成也减少;另外接受NAs治疗的CHB人群在病毒清除的过程中可能会促进机体免疫应答的能力从而减少cccDNA池。但是在临床上发现即使CHB患者经过长期NAs抗病毒治疗,能实现完全治愈的患者极为罕见,可能是只需要极少部分逆转录酶存在活性就能对cccDNA池进行补充,因此对大部分CHB患者而言需要长期口服NAs抗病毒治疗。
本研究发现,未接受治疗的CHB患者HBV RNA与HBsAg(r=0.612,P<0.01)、HBV DNA(r=0.922, P<0.01)均具有较强的正相关,这种血清学间良好的相关性有助于基层医院或者医疗资源匮乏地区,使用HBsAg定量水平反映HBeAg阳性CHB患者体内病毒复制水平,而另外两组HBV DNA阴性的CHB患者HBV RNA与HBsAg无相关性,这与Mak等[12]的研究结果一致,随着治疗时间的延长,HBV RNA与HBsAg相关性逐渐下降,从一定程度反映了治疗后的HBsAg水平不能准确反映肝内cccDNA转录活性。
综上所述,对未接受抗病毒治疗的CHB患者,血清HBV RNA与其他血清学标志物有一定的相关性,对NAs治疗后HBV DNA阴转的患者有望使用HBV RNA继续监测肝内病毒复制活性,为CHB患者长期抗病毒治疗提供依据。但本研究样本量较少,相关结论有待进一步证实,后续可以在未治疗组继续纳入合适患者并进行前瞻性队列研究,观察HBeAg阳性CHB患者在NAs治疗过程中HBV RNA的动态变化。
|
[1] XIE L, HAO P, WU RH, et al. Establishment and application of a database for hepatitis C virus NS3/4A protease inhibitors and their drug resistance data[J]. J Clin Hepatol, 2018, 34 (9) :1884-1890. (in Chinese) 谢磊, 郝沛, 吴瑞红, 等. HCV NS3/4A蛋白酶抑制剂药物及其耐药信息数据库的建立和应用[J].临床肝胆杂志, 2018, 34 (9) :1884-1890.
|
|
[2] MESSINA JP, HUMPHREYS I, FLAXMAN A, et al. Global distribution and prevalence of hepatitis C virus genotypes[J].Hepatology, 2015, 61 (1) :77-87.
|
|
[3] PAWLOTSKY JM, NEGRO F, AGHEMO A, et al. EASL Recommendations on treatment of hepatitis C 2018[J]. Hepatology, 2018, 69 (2) :461-511.
|
|
[4] MOHD HANAFIA K, GROEGER J, FLAXMAN AD, et al. Global epidemiology of hepatitis C virus infection:New estimates of age-specific antibody to HCV seroprevalence[J]. Hepatology, 2013, 57 (4) :1333-1342.
|
|
[5] TANG W, SU MH, JIANG JN, et al. Epidemiological characteristics and genotype distribution of hepatitis C virus in Guangxi[J]. World Chin J Dig, 2014, 22 (9) :1300-1306. (in Chinese) 唐维, 苏明华, 江建宁, 等.广西地区丙型肝炎病毒的基因型分布与流行病学特征[J].世界华人消化杂志, 2014, 22 (9) :1300-1306.
|
|
[6] MANNS M, MARCELLIN P, POORDAD F, et al. Simeprevir with pegylated interferon alfa 2a or 2b plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1infection (QUEST-2) :A randomised, double-blind, placebo-controlled phase 3 trial[J]. Lancet, 2014, 384 (9941) :414-426.
|
|
[7] DONALDSON EF, HARRINGTON PR, O'REAR JJ, et al. Clinical evidence and bioinformatics characterization of potential hepatitis C virus resistance pathways for sofosbuvir[J]. Hepatology, 2015, 61 (1) :56-65.
|
|
[8] QUAN M, XING HC. Effects of hepatitis C virus resistance associated variants on the efficacy of direct-acting antiviral agents[J/CD]. Chin J Liver Dis:Electronic Edit, 2018, 10 (3) :32-36. (in Chinese) 全敏, 邢卉春.丙型肝炎病毒耐药相关变异对直接抗病毒药物疗效的影响[J/CD].中国肝脏病杂志:电子版, 2018, 10 (3) :32-36.
|
|
[9] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guide line of prevention and treatment for chronic hepatitis C:A 2015 update[J]. J Clin Hepatol, 2015, 31 (12) :1961-1979. (in Chinese) 中华医学会肝病学分会, 中华医学会感染病学分会.丙型肝炎防治指南 (2015年更新版) [J].临床肝胆病杂志, 2015, 31 (12) :1961-1979.
|
|
[10] AN ZY, DING Y, DOU XG, et al. Selection and evaluation of treatment regimens with direct-acting antiviral agents for patients with chronic hepatitis C in the real world in China[J]. J Clin Hepatol, 2018, 34 (2) :233-237. (in Chinese) 安子英, 丁洋, 窦晓光, 等.我国慢性丙型肝炎患者真实世界中直接抗病毒药物治疗方案的选择与评价[J].临床肝胆杂志, 2018, 34 (2) :233-237.
|
|
[11] LEMM JA, LIU M, GENTLES RG, et al. Preclinical characterization of BMS-791325, an allosteric inhibitor of hepatitis C Virus NS5B polymerase[J]. Antimicrob Agents Chemother, 2014, 58 (6) :3485-3495.
|
|
[12] DVORY-SOBOL H, VOITENLEITNER C, MABERY E, et al.Clinical and in vitro resistance to GS-9669, a thumb site II nonnucleoside inhibitor of the hepatitis C virus NS5B polymerase[J]. Antimicrob Agents Chemother, 2014, 58 (11) :6599-6606.
|
|
[13] SUN D, DAI M, SHEN S, et al. Analysis of naturally occurring resistance-associated variants to NS3/4A Protein inhibitors, NS5A protein inhibitors, and NS5B polymerase inhibitors in patients with chronic hepatitis C[J]. Gene Expression, 2018, 18 (1) :63-69.
|
|
[14] CHARLTON M, GANE E, MANNS MP, et al. Sofosbuvir and ribavirin for treatment of compensated recurrent hepatitis C virus infection after liver transplantation[J]. Gastroenterology, 2015, 148 (1) :108-117.
|
|
[15] ALVES R, QUEIROZ ATL, PESSOA MG, et al. The presence of resistance mutations to protease and polymerase inhibitors in hepatitis C virus sequences from the Los Alamosdatabank[J]. J Viral Hepat, 2013, 20 (6) :414-421.
|
|
[16] WANG Y, RAO HY, XIE XW, et al. Direct-acting antiviral agents resistance-associated polymorphisms in chinese treatment-nave patients infected with genotype 1b hepatitis C virus[J]. Chin Med J (Engl) , 2015, 128 (19) :2625-2631.
|
|
[17] JI H, KOZAK RA, BIONDI MJ, et al. Next generation sequencing of the hepatitis C virus NS5B gene reveals potential novel S282drug resistance mutations[J]. Virology, 2015, 477:1-9.
|
|
[18] BARTELS DJ, SULLIVAN JC, ZHANG EZ, et al. Hepatitis C virus variants with decreased sensitivity to direct-acting antivirals (DAAs) were rarely observed in DAA-naive patients prior to treatment[J]. J Virol, 2013, 87 (3) :1544-1553.
|
|
[19] HALFON P, SARRAZIN C. Future treatment of chronic hepatitis C with direct acting antivirals:Is resistance important?[J].Liver Int, 2012, 32 (Suppl 1) :79-87.
|
|
[20] VOITENLEITNER C, CROSBY R, WALKER J, et al. In vitro characterization of GSK2485852, a novel hepatitis C virus polymerase inhibitor[J]. Antimicrob Agents Chemother, 2013, 57 (11) :5216-5224.
|


The first journal specializing in hepatobiliary and pancreatic diseases in China
Supervisor:Ministry of Education of the People's Republic of China
Sponsor:Jilin University
Academic Support: Chinese Society of Hepatology,Chinese Medical Association
Address: 461 Xinjiang Road, Changchun
Submit:0431-88782044
Peer review:0431-88783542
Email:lcgdb@vip.163.com
Website Design © 2020 Editorial Board of Journal of Clinical Hepatology
吉ICP备10000617号-1
Supported by: Beijing Renhe Information Technology Co. Ltd

WANG CK, LIU SR. Expression level of serum HBV RNA in HBeAg-positive chronic hepatitis B patients at different periods and its value of measurement[J]. J Clin Hepatol, 2021, 37(12): 2798-2801. DOI: 10.3969/j.issn.1001-5256.2021.12.014.

| 组别 | 例数 | 男 | 女 | 年龄(岁) |
| HBeAg(+)、HBV DNA(+) | 22 | 13 | 9 | 35.36±7.55 |
| HBeAg(+)、HBV DNA(-) | 17 | 11 | 6 | 39.35±7.98 |
| HBeAg(-)、HBV DNA(-) | 22 | 13 | 9 | 45.00±11.16 |
| 项目 | HBeAg阳性组(n=17) | HBeAg阴性组(n=22) | 统计值 | P值 |
| 男/女(例) | 11/6 | 13/9 | 0.753 | |
| 年龄(岁) | 39.35±7.98 | 45.00±11.16 | t=-1.77 | 0.086 |
| HBV RNA阳性[例(%)] | 15(88.2) | 6(27.3) | <0.001 | |
| HBV RNA(log10拷贝/mL) | 4.05(3.01~5.18) | 1.40(1.40~1.83) | Z=-4.44 | <0.001 |
| HBsAg(log10IU/mL) | 3.24(2.86~3.50) | 2.76(2.07~3.35) | Z=-2.41 | 0.016 |
| ALT(U/L) | 22.24±10.83 | 25.09±11.76 | t=-0.78 | 0.442 |
| AST(U/L) | 23.00±4.48 | 23.9±14.23 | t=-0.65 | 0.521 |
| 项目 | HBV DNA阳性组(n=22) | HBV DNA阴性组(n=39) | 统计值 | P值 |
| 男/女(例) | 13/9 | 24/15 | χ2=0.035 | 0.851 |
| 年龄(岁) | 35.36±7.55 | 42.54±10.18 | t=-2.88 | 0.005 |
| HBV RNA(log10拷贝/mL) | 7.62(6.51~8.55) | 1.94(1.40~4.04) | Z=-6.16 | <0.001 |
| HBsAg(log10IU/mL) | 3.94(3.26~4.23) | 2.90(2.61~3.44) | Z=-4.07 | <0.001 |
| ALT(U/L) | 249.50(114.25~664.50) | 20.00(16.00~31.00) | Z=-6.45 | <0.001 |
| AST(U/L) | 106.00(63.75~418.75) | 23.00(21.00~27.00) | Z=-6.45 | <0.001 |
| HBV DNA(log10IU/ml) | 7.21±1.23 | - |
| 组别 | 例数 | 男 | 女 | 年龄(岁) |
| HBeAg(+)、HBV DNA(+) | 22 | 13 | 9 | 35.36±7.55 |
| HBeAg(+)、HBV DNA(-) | 17 | 11 | 6 | 39.35±7.98 |
| HBeAg(-)、HBV DNA(-) | 22 | 13 | 9 | 45.00±11.16 |
| 项目 | HBeAg阳性组(n=17) | HBeAg阴性组(n=22) | 统计值 | P值 |
| 男/女(例) | 11/6 | 13/9 | 0.753 | |
| 年龄(岁) | 39.35±7.98 | 45.00±11.16 | t=-1.77 | 0.086 |
| HBV RNA阳性[例(%)] | 15(88.2) | 6(27.3) | <0.001 | |
| HBV RNA(log10拷贝/mL) | 4.05(3.01~5.18) | 1.40(1.40~1.83) | Z=-4.44 | <0.001 |
| HBsAg(log10IU/mL) | 3.24(2.86~3.50) | 2.76(2.07~3.35) | Z=-2.41 | 0.016 |
| ALT(U/L) | 22.24±10.83 | 25.09±11.76 | t=-0.78 | 0.442 |
| AST(U/L) | 23.00±4.48 | 23.9±14.23 | t=-0.65 | 0.521 |
| 项目 | HBV DNA阳性组(n=22) | HBV DNA阴性组(n=39) | 统计值 | P值 |
| 男/女(例) | 13/9 | 24/15 | χ2=0.035 | 0.851 |
| 年龄(岁) | 35.36±7.55 | 42.54±10.18 | t=-2.88 | 0.005 |
| HBV RNA(log10拷贝/mL) | 7.62(6.51~8.55) | 1.94(1.40~4.04) | Z=-6.16 | <0.001 |
| HBsAg(log10IU/mL) | 3.94(3.26~4.23) | 2.90(2.61~3.44) | Z=-4.07 | <0.001 |
| ALT(U/L) | 249.50(114.25~664.50) | 20.00(16.00~31.00) | Z=-6.45 | <0.001 |
| AST(U/L) | 106.00(63.75~418.75) | 23.00(21.00~27.00) | Z=-6.45 | <0.001 |
| HBV DNA(log10IU/ml) | 7.21±1.23 | - |
 下载:
下载:

 DownLoad:
DownLoad: