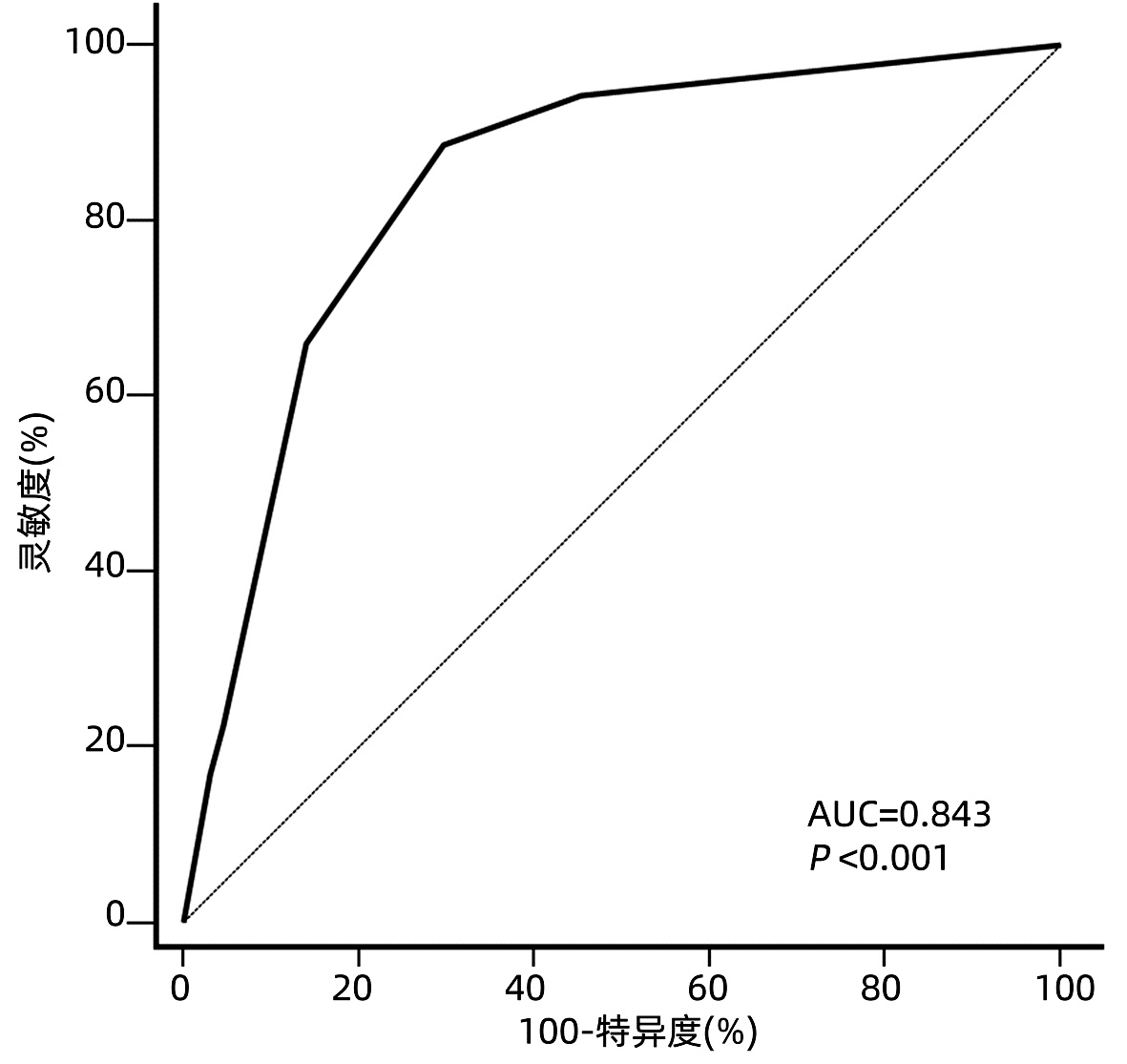
Objective To develop a new model for predicting recurrence after liver transplantation for hepatocellular carcinoma (HCC) beyond Milan criteria based on related preoperative and postoperative indicators.Methods A retrospective analysis was performed for the clinical data of the patients with HCC beyond Milan criteria who underwent orthotopic liver transplantation for the first time in Tianjin First Central Hospital from August 2014 to July 2018, and according to the presence or absence of recurrence during follow-up, the patients were divided into recurrence group and no-recurrence group. The t-test or the Mann-Whitney U test was used for comparison of continuous data between groups, and the chi-square test or the Fisher's exact test was used for comparison of categorical data between groups. The Kaplan-Meier method was used to plot survival curves, and the log-rank test was used for comparison of survival curves. Univariate and multivariate Cox proportional hazards regression analyses were used to identify the risk factors for recurrence-free survival after surgery. A new model was developed for recurrence after liver transplantation in the patients with HCC beyond Milan criteria based on the risk factors identified. The area under the receiver operating characteristic curve (AUC) was used to evaluate predictive performance, and the Hosmer-Lemeshow test was used to assess the goodness of fit of the model.Results A total of 117 patients with HCC beyond Milan criteria were enrolled in this study, with a median follow-up time of 24 (1-74) months. A total of 53 patients (45.3%) experienced recurrence after surgery, among whom 52 (98.1%) had recurrence within 3 years after surgery, with a median time to recurrence of 6 (1-52) months. The Cox proportional hazards regression analysis showed that preoperative serum alpha-fetoprotein (AFP) >769 ng/mL, neutrophil-lymphocyte ratio (NLR) >3.75, and ki67 index >0.25 were independent risk factors for recurrence-free survival after liver transplantation. The model established based on these three risk factors had an AUC of 0.843, with good sensitivity (88.7%) and specificity (70.3%). The optimal cut-off value was selected according to the maximization of Youden index, and then the patients were divided into low-risk group (0-1 point) and high-risk group (1.5-4 points). The log-rank test showed that the low-risk group had significantly higher 3-and 5-year recurrence-free survival rates than the high-risk group (84.1%/72.0% vs 10.9%/10.9%, χ2=29.425, P < 0.001).Conclusion Liver transplantation for HCC beyond Milan criteria should be performed with caution, and the predictive model established based on preoperative AFP, NLR, and ki67 index can accurately assess the indication for liver transplantation in such patients.
BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. DOI: 10.3322/caac.21492.
[2]
MAZZAFERRO V, REGALIA E, DOCI R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis[J]. N Engl J Med, 1996, 334(11): 693-699. DOI: 10.1056/NEJM199603143341104.
[3]
XU X, LU D, LING Q, et al. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria[J]. Gut, 2016, 65(6): 1035-1041. DOI: 10.1136/gutjnl-2014-308513.
[4]
SAPISOCHIN G, BRUIX J. Liver transplantation for hepatocellular carcinoma: Outcomes and novel surgical approaches[J]. Nat Rev Gastroenterol Hepatol, 2017, 14(4): 203-217. DOI: 10.1038/nrgastro.2016.193.
[5]
ZAVAGLIA C, de CARLIS L, ALBERTI AB, et al. Predictors of long-term survival after liver transplantation for hepatocellular carcinoma[J]. Am J Gastroenterol, 2005, 100(12): 2708-2716. DOI: 10.1111/j.1572-0241.2005.00289.x.
[6]
REN A, LI Z, ZHOU X, et al. Evaluation of the alpha-fetoprotein model for predicting recurrence and survival in patients with hepatitis B virus (HBV)-related cirrhosis who received liver transplantation for hepatocellular carcinoma[J]. Front Surg, 2020, 7: 52. DOI: 10.3389/fsurg.2020.00052.
[7]
ZHANG X, WU Z, PENG Y, et al. Correlationship between Ki67, VEGF, and p53 and hepatocellular carcinoma recurrence in liver transplant patients[J]. Biomed Res Int, 2021, 2021: 6651397. DOI: 10.1155/2021/6651397.
[8]
FENG J, ZHU R, FENG D, et al. Prediction of early recurrence of solitary hepatocellular carcinoma after orthotopic liver transplantation[J]. Sci Rep, 2019, 9(1): 15855. DOI: 10.1038/s41598-019-52427-8.
[9]
COUSSENS LM, WERB Z. Inflammation and cancer[J]. Nature, 2002, 420(6917): 860-867. DOI: 10.1038/nature01322.
[10]
COFFELT SB, de VISSER KE. Cancer: Inflammation lights the way to metastasis[J]. Nature, 2014, 507(7490): 48-49. DOI: 10.1038/nature13062.
[11]
AINO H, SUMIE S, NⅡZEKI T, et al. The systemic inflammatory response as a prognostic factor for advanced hepatocellular carcinoma with extrahepatic metastasis[J]. Mol Clin Oncol, 2016, 5(1): 83-88. DOI: 10.3892/mco.2016.879.
[12]
MOTOMURA T, SHIRABE K, MANO Y, et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment[J]. J Hepatol, 2013, 58(1): 58-64. DOI: 10.1016/j.jhep.2012.08.017.
[13]
XU ZG, YE CJ, LIU LX, et al. The pretransplant neutrophil-lymphocyte ratio as a new prognostic predictor after liver transplantation for hepatocellular cancer: A systematic review and meta-analysis[J]. Biomark Med, 2018, 12(2): 189-199. DOI: 10.2217/bmm-2017-0307.
[14]
SULLIVAN LM, MASSARO JM, SR DRB. Presentation of multivariate data for clinical use: The Framingham Study risk score functions[J]. Stat Med, 2004, 23(10): 1631-1660. DOI: 10.1002/sim.1742.
[15]
JOU Y, HUANG C, CHO H. A VIF-based optimization model to alleviate collinearity problems in multiple linear regression[J]. Computational Statistics, 2014, 29(6): 1515-1541. DOI: 10.1007/s00180-014-0504-3.
[16]
MA E, LI J, XING H, et al. Development of a predictive nomogram for early recurrence of hepatocellular carcinoma in patients undergoing liver transplantation[J]. Ann Transl Med, 2021, 9(6): 468. DOI: 10.21037/atm-21-334.
[17]
MA KW, SHE WH, CHAN A, et al. Validated model for prediction of recurrent hepatocellular carcinoma after liver transplantation in Asian population[J]. World J Gastrointest Oncol, 2019, 11(4): 322-334. DOI: 10.4251/wjgo.v11.i4.322.
[18]
SHIMAMURA T, AKAMATSU N, FUJIYOSHI M, et al. Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: The 5-5-500 rule-a retrospective study[J]. Transpl Int, 2019, 32(4): 356-368. DOI: 10.1111/tri.13391.
[19]
SHI K, LI P, XUE D, et al. Neutrophil-lymphocyte ratio and the risk of hepatocellular carcinoma in patients with hepatitis B-caused cirrhosis[J]. Eur J Gastroenterol Hepatol, 2021, 33(1S Suppl 1): e686-e692. DOI: 10.1097/MEG.0000000000002217.
[20]
SILVA TH, SCHILITHZ A, PERES W, et al. Neutrophil-lymphocyte ratio and nutritional status are clinically useful in predicting prognosis in colorectal cancer patients[J]. Nutr Cancer, 2020, 72(8): 1345-1354. DOI: 10.1080/01635581.2019.1679198.
[21]
CHEN L, QI L, ZHANG J, et al. Neutrophil-lymphocyte ratio as a prognostic factor for minute clear cell renal cell carcinoma diagnosed using multi-slice spiral CT[J]. Medicine (Baltimore), 2021, 100(23): e26292. DOI: 10.1097/MD.0000000000026292.
[22]
KOTEISH A, THULUVATH PJ. Screening for hepatocellular carcinoma[J]. J Vasc Interv Radiol, 2002, 13(9 Pt 2): s185-s190. DOI: 10.1016/s1051-0443(07)61785-0.
[23]
JIANG N, ZENG KN, DOU KF, et al. Preoperative alfa-fetoprotein and fibrinogen predict hepatocellular carcinoma recurrence after liver transplantation regardless of the Milan criteria: model development with external validation[J]. Cell Physiol Biochem, 2018, 48(1): 317-327. DOI: 10.1159/000491731.
[24]
HALAZUN KJ, NAJJAR M, ABDELMESSIH RM, et al. Recurrence after liver transplantation for hepatocellular carcinoma: A new MORAL to the story[J]. Ann Surg, 2017, 265(3): 557-564. DOI: 10.1097/SLA.0000000000001966.
[25]
FENG J, WU J, ZHU R, et al. Simple risk score for prediction of early recurrence of hepatocellular carcinoma within the Milan criteria after orthotopic liver transplantation[J]. Sci Rep, 2017, 7: 44036. DOI: 10.1038/srep44036.
[26]
MEHTA N, HEIMBACH J, HARNOIS DM, et al. Validation of a risk estimation of tumor recurrence after transplant (RETREAT) score for hepatocellular carcinoma recurrence after liver transplant[J]. JAMA Oncol, 2017, 3(4): 493-500. DOI: 10.1001/jamaoncol.2016.5116.
[27]
JIANG P, JIA M, HU J, et al. Prognostic value of Ki67 in patients with stage 1-2 endometrial cancer: Validation of the cut-off value of Ki67 as a predictive factor[J]. Onco Targets Ther, 2020, 13: 10841-10850. DOI: 10.2147/OTT.S274420.
[28]
CSERNI G, VÖRÖS A, LIEPNIECE-KARELE I, et al. Distribution pattern of the Ki67 labelling index in breast cancer and its implications for choosing cut-off values[J]. Breast, 2014, 23(3): 259-263. DOI: 10.1016/j.breast.2014.02.003.
[29]
WILKINS AC, GUSTERSON B, SZIJGYARTO Z, et al. Ki67 Is an independent predictor of recurrence in the largest randomized trial of 3 radiation fractionation schedules in localized prostate cancer[J]. Int J Radiat Oncol Biol Phys, 2018, 101(2): 309-315. DOI: 10.1016/j.ijrobp.2018.01.072.
[30]
GRANT L, BANERJI S, MURPHY L, et al. Androgen receptor and Ki67 expression and survival outcomes in non-small cell lung cancer[J]. Horm Cancer, 2018, 9(4): 288-294. DOI: 10.1007/s12672-018-0336-7.
[31]
JACOBSEN F, KOHSAR J, GEBAUER F, et al. Loss of p16 and high Ki67 labeling index is associated with poor outcome in esophageal carcinoma[J]. Oncotarget, 2020, 11(12): 1007-1016. DOI: 10.18632/oncotarget.27507.
[32]
TEMRAZ S, SHAMSEDDINE A, MUKHERJI D, et al. Ki67 and P53 in relation to disease progression in metastatic pancreatic cancer: A single institution analysis[J]. Pathol Oncol Res, 2019, 25(3): 1059-1066. DOI: 10.1007/s12253-018-0464-y.

 下载:
下载:











 DownLoad:
DownLoad: