
图
1
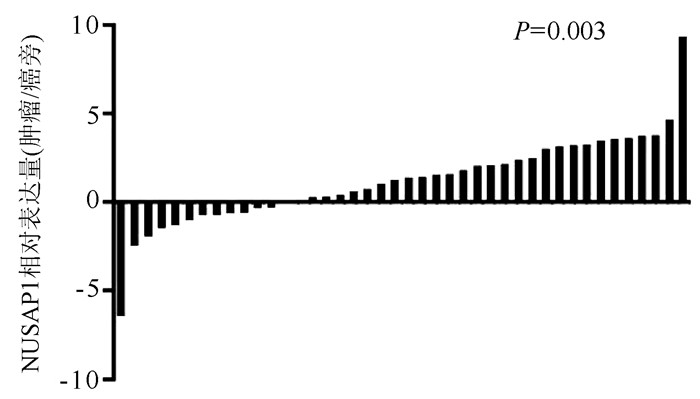
NUSAP1在临床肝癌样本中高表达
Objective To investigate the expression of T-cell immunoglobulin and mucin domain-containing molecule 3 ( TIM-3) in natural killer T ( NKT) cells and its association with liver injury and prognosis in patients with hepatitis B virus-related acute-on-chronic liver failure ( HBV-ACLF) . Methods Peripheral blood mononuclear cells were isolated from 43 patients with HBV-ACLF and 28 patients with chronic hepatitis B ( CHB) who were treated in Beijing YouAn Hospital, Capital Medical University, from September 2016 to June 2018, and flow cytometry was used to measure the number of peripheral blood CD3+CD56+NKT cells and the expression of TIM-3.The t-test was used for comparison of normally distributed continuous data between two groups. The Kruskal-Wallis H test was used for comparision of non-normally distributed continuous data between multiple groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between groups, and the Pearson correlation coefficient was used to investigate correlation. Results Compared with the CHB group, the HBV-ACLF group had significantly higher alanine aminotransferase ( ALT) , aspartate aminotransferase ( AST) , total bilirubin ( TBil) , creatinine, international normalized ratio ( INR) , HBV DNA, TBil/ALT ratio, and Model for End-Stage Liver Disease ( MELD) score, as well as significantly lower albumin and prothrombin time activity ( PTA) ( all P < 0. 05) . Compared with the CHB group, the HBV-ACLF grouphad a significantly higher number of CD3+CD56+NKT cells ( 19. 13% ± 13. 82% vs 26. 75% ± 11. 84%, t = 2. 401, P = 0. 019) and significantly higher expression of TIM-3 in CD3+CD56+NKT cells [5. 53% ( 2. 95%-10. 2%) vs 1. 59% ( 0. 91%-2. 7%) , Z =-5. 260, P < 0. 001]. The expression of TIM-3 in CD3+CD56+NKT cells was positively correlated with ALT ( r = 0. 637, P < 0. 000 1) , AST ( r = 0. 414, P = 0. 006) , INR ( r = 0. 335, P = 0. 031) , and MELD score ( r = 0. 355, P = 0. 021) and was negatively correlated with PTA% ( r =-0. 313, P = 0. 043) . Among the 43 patients with HBV-ACLF, 12 had early-stage HBV-ACLF, 21 had middle-stage HBV-ACLF, and 10 had advanced HBV-ACLF, and there was no significant difference in the number of CD3+CD56+NKT cells between the three groups ( all P > 0. 05) , but with a tendency of increase; the patients with middle-stage or advanced HBV-ACLF had significantly higher expression of TIM-3 in CD3+CD56+NKT cells than those with early-stage HBV-ACLF [6. 5% ( 3. 16%-11. 45%) /8. 56% ( 4%-10. 93%) vs 2. 58% ( 1. 92%-6. 02%) , Z =-2. 284, -2. 641, both P < 0. 05]. Among the 43 patients with HBV-ACLF, the28-day survival group had significantly lower expression of TIM-3 in CD3+CD56+NKT cells than the 28-day liver transplantation/death group [2. 98% ( 1. 94%-6. 88%) vs 8. 56% ( 4. 27%-11. 43%) , Z =-2. 831, P = 0. 005]. Conclusion There is an increase in the expression of TIM-3 in peripheral blood CD3+CD56+NKT cells in patients with HBV-ACLF, which is associated with the degree of liver injury and prognosis.
肝癌作为消化系统最常见的恶性肿瘤之一,其发病率与致死率在各类肿瘤中一直位居前列[1]。我国每年肝癌新发病例数与死亡病例数约占全球总病例数的一半[2],其中肝细胞癌占绝大多数,因此本文主要讨论肝细胞癌。肝癌的发展,除因环境因素影响外,往往还与基因的突变或异常表达有关[3]。由于肝癌具有早期症状不明显、进展隐匿等特点,尽管在肝癌发现后可以进行手术为主的多种治疗方法,但总体预后不佳[4-6]。肿瘤发生与进展的关键在于正常的细胞周期被破坏,失去分化的能力,最终发生恶性增殖。因此,可以将抑制肝癌细胞的恶性增殖、恢复其正常的细胞进程作为治疗肝癌的潜在靶向。
核仁纺锤体相关蛋白1(nuclelar spindle-associated protein 1, NUSAP1)作为一种微管结合蛋白,在人体内高度保守,其作用在于调控纺锤体的正确装配以及染色体的形成,在有丝分裂过程中发挥不可或缺的作用[7-9]。在正常的组织中,NUSAP1的表达水平受到严格的调控,以防止细胞增殖异常。当NUSAP1表达异常增高时,会导致细胞有丝分裂进程无法终止,引起细胞的无限增殖以及遗传物质的不稳定。现有研究[10-16]已经证实,NUSAP1在多种肿瘤中表达异常增高,提示其密切参与肿瘤的发生与发展。
生物信息学分析在近几年越来越多的用于研究肿瘤进展过程中的基因表达变化[17]。通过对大量共享数据的挖掘、分析及解释,可以方便、快捷地发现具有表达差异的基因,找到疾病治疗的潜在靶标以及预后评估的可能标志物[18]。本研究通过对GEO及TCGA数据库公共数据的整理分析,对NUSAP1在肝癌组织及细胞亚群中的表达差异及其对预后的影响进行了初步的探索。
从TCGA数据库下载肝癌转录组信息及临床数据,选择临床信息完善的数据进行基因表达差异分析,以剔除肿瘤复发类型为非肝癌的R0切除术后患者的临床信息评估其预后。在GEO官网下载GSE57957、GSE14520、GSE22058、GSE46444、GSE54236、GSE36376、GSE64041、GSE76297、GSE76427、GSE102079共10个种属为Homo sapiens的肝癌数据集。在GEO官网下载单细胞测序数据集GSE149614。选取2018年1月—2019年11月在青岛大学附属医院进行同种异体肝移植术的随访信息完善、病理诊断明确、生物样本取材规范的乙型肝炎相关肝癌患者42例,统计其临床资料,包括性别、血型、年龄、BMI、血清AFP水平、MELD评分、Child-Pugh分级、肿瘤直径、肿瘤数目、TNM分期及Okuda分期等。
对选取的42例临床样本利用Trizol法提取总RNA,并通过TaKaRa反转录试剂盒合成cDNA。利用TaKaRa PCR试剂盒进行实时荧光定量-PCR反应,以GAPDH为内参照,测定NUSAP1相对表达水平。GAPDH引物序列为:F:5′-CGGGCTCTCCAGAACATC-3′,R:5′-ATGACCTTGCCCACAGCCT-3′;NUSAP1引物序列为F:5′-ACCCTGACTCACAGCAGAATC-3′,R:5′-CAGCTTCTTGGTGCTCGTCT-3′。
本研究方案经由青岛大学附属医院伦理委员会审批,批号:QYFYWZLL26046。
R 4.0软件用于所有数据集基因表达差异分析及单细胞测序数据的聚类分析。采用SPSS 21.0软件对数据进行统计分析。计数资料2组间比较采用χ2检验。以Kaplan-Meier方法生存分析NUSAP1表达水平与总体生存率及无病间隔生存率之间的关系,运用log-rank进行检验,通过Graphpad prim 7使其结果可视化。P<0.05为差异有统计学意义。
为研究NUSAP1在肝癌组织中的表达,同时从GEO和TCGA中下载肝癌和癌旁组织基因表达数据。结果显示,NUSAP1在10个GEO肝细胞数据集中的肝癌组织中高表达,在TCGA数据库中也呈高表达(P值均<0.001)(附录1)。
为避免肿瘤异质性对本研究的影响,从GEO中下载了肝细胞癌的单细胞测序数据集GSE149614并进行聚类分析。依据细胞标志物和组织来源的差异,将所有细胞分为来源于肿瘤组织的细胞与来源于癌旁组织的细胞。结果显示,来源于肿瘤组织的细胞其NUSAP1高表达细胞明显高于癌旁组织细胞(附录2)。
数据库的测序结果,通过实时荧光定量PCR检测42例患者肝癌和癌旁组织中NUSAP1的相对表达。与GEO和TCGA数据库分析结果一致,NUSAP1在29例患者的肝癌组织中高表达,在13例患者的肝癌组织中低表达(P=0.003)(图 1)。
NUSAP1在肝细胞癌组织中高表达组及低表达组间,Child-Pugh分级、TNM分期、Okuda分期比较差异均有统计学意义(P值均<0.05)(表 1), 表明NUSAP1的表达水平与肝癌患者的病情严重程度有关。
| 项目 | 高表达(n=29) | 低表达(n=13) | χ2值 | P值 |
| 性别(例) | 0.022 | 0.88 | ||
| 男 | 24 | 11 | ||
| 女 | 5 | 2 | ||
| 血型(例) | 0.628 | 0.89 | ||
| O型 | 5 | 3 | ||
| A型 | 11 | 5 | ||
| B型 | 12 | 5 | ||
| AB型 | 1 | 0 | ||
| 年龄 | 2.143 | 0.14 | ||
| <50岁 | 16 | 4 | ||
| ≥50岁 | 13 | 9 | ||
| BMI | 0.633 | 0.43 | ||
| 18.5~23.9 kg/m2 | 14 | 8 | ||
| <18.5 kg/m2或≥24 kg/m2 | 15 | 5 | ||
| AFP(例) | 0.252 | 0.62 | ||
| <20 ng/ml | 11 | 6 | ||
| ≥20 ng/ml | 18 | 7 | ||
| MELD评分(例) | 0.032 | 0.86 | ||
| <20分 | 17 | 8 | ||
| ≥30分 | 12 | 5 | ||
| Child-Pugh分级(例) | 5.469 | 0.02 | ||
| A级 | 7 | 8 | ||
| B或C级 | 22 | 5 | ||
| 肿瘤数目(例) | 0.001 | 0.97 | ||
| 单发 | 11 | 5 | ||
| 多发 | 18 | 8 | ||
| TNM分期(例) | 6.836 | 0.01 | ||
| Ⅰ期 | 3 | 6 | ||
| Ⅱ或Ⅲ期 | 26 | 7 | ||
| Okuda分期(例) | 4.617 | 0.03 | ||
| Ⅰ | 6 | 7 | ||
| Ⅱ或Ⅲ | 23 | 6 |
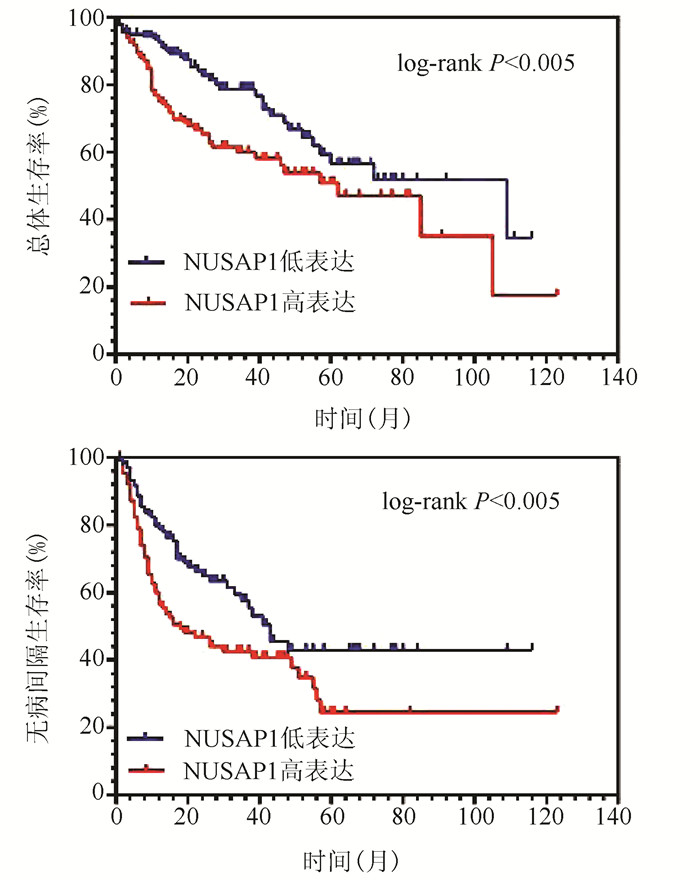
NUSAP1高表达的肝癌患者总体生存率与无病间隔生存率均显著低于低表达的肝癌患者(图 2),NUSAP1低表达患者1、3、5年生存率分别为92.96%、83.80%、76.76%,明显高于高表达的患者(76.76%、67.60%、64.78%)(χ2值分别为8.156、7.853、7.671, P值均<0.05),NUSAP1高表达的患者中位生存时间明显低于低表达的患者(61.7个月vs 108.6个月)(χ2=7.955, P<0.05)。
肝癌的发生是一个复杂的过程,有多种细胞参与肝癌的发生与进展[19]。肝癌因其恶性程度高、易复发等特点,常见的治疗手段并不能显著改善肝癌患者的生存时间[20]。遗传因素作为限制肝癌患者预后的重要因素持续受到人们的关注。相比于传统的实验方法,随着生物信息学的发展以及肿瘤基因数据的共享,使得肿瘤相关基因的发现周期大为缩短,为研究肝癌发生发展机制,探寻潜在治疗靶点提供了重大便利。
NUSAP1作为有丝分裂中的一种关键蛋白,通过参与有丝分裂中纺锤体的形成得以调控细胞的增殖,其表达水平受到严格的调控,一旦NUSAP1表达异常升高,细胞将无限增殖,甚至影响遗传物质[9]。已有研究[14-15]证实,NUSAP1在多种肿瘤(如胶质母细胞癌、肾癌、乳腺癌等)中表达均显著提高,且均与预后有关,可以作为该型肿瘤的潜在标志物。本研究通过对大量GEO芯片数据及TCGA数据集的分析,证实NUSAP1在肝癌组织中的表达明显升高。通过对单细胞测序数据的分析,使NUSAP1高表达的肝癌细胞来源于肝癌组织中的推论更为明确,进一步证实肝癌细胞的无限增殖与NUSAP1表达升高的关系。由此推断,在肝脏因遗传因素或外界理化因素刺激后,NUSAP1表达出现异常增高,使肝细胞持续增殖,最终诱导癌变的产生。通过对TCGA数据库中患者预后信息的分析发现,NUSAP1的表达水平明显影响患者的预后,高表达组的患者总体生存率、无病间隔生存率均显著低于低表达组。进一步临床资料分析证实了上述结论,并发现NUSAP1在肝癌中的表达水平与Child-Pugh分级、TNM分期、Okuda分期显著相关,表明NUSAP1的表达升高使得肿瘤细胞增殖旺盛,使肝癌进展迅速,患者病情恶化加快,从而影响预后。综上所述,NUSAP1可以作为肝癌不良预后的新标志物并可以成为肝癌治疗的潜在新靶点。
综上所述,本研究将高通量基因芯片数据、单细胞测序数据的分析与现有临床样本PCR验证相结合,避免了单一研究方式的不足,结论更有说服力。研究验证了NUSAP1在肝癌细胞中的异常表达升高且与患者预后相关,为肝癌的靶向用药提供了新的潜在靶点。
|
|
|
[1] Liver Failure and Artificial Liver Group, Chinese Society of Infectious Diseases, CMA; Severe Liver Disease and Artificial Liver Group, Chinese Society of Hepatology, CMA. Guideline for diagnosis and treatment of liver failure[J]. Chin J Clin Infect Dis, 2012, 5 (6) :321-327. (in Chinese) 中华医学会感染病学分会肝衰竭与人工肝学组, 中华医学会肝病学分会重型肝病与人工肝学组.肝衰竭诊治指南 (2012年版) [J].中华临床感染病杂志, 2012, 5 (6) :321-327.
|
|
[2] ALAM A, CHUN SUEN K, MA D. Acute-on-chronic liver failure:Recent update[J]. J Biomed Res, 2017, 31 (3) :1-18.
|
|
[3] SMYK DS, MAVROPOULOS A, MIELI-VERGANI G, et al. The role of invariant NKT in autoi-mmune liver disease:Can vitamin D act as an immunomodulator?[J]. Can J Gastroenterol Hepatol, 2018:8197937.
|
|
[4] SIDDIQUI S, VISVABHARATHY L, WANG CR. Role of group 1CD1-restricted T cells in infectious disease[J]. Front Immunol, 2015, 6:337.
|
|
[5] BAE EA, SEO H, KIM IK, et al. Roles of NKT cells in cancer immunotherapy[J]. Arch Pharm Res, 2019, 42 (7) :543-548.
|
|
[6] SASIDHARAN NAIR V, TOOR SM, TAHA RZ, et al. DNA methylation and repressive histones in the promoters of PD-1, CTLA-4, TIM-3, LAG-3, TIGIT, PD-L1, and galectin-9 genes in human colorectal cancer[J]. Clin Epigenetics, 2018, 10 (1) :104.
|
|
[7] WANG L, ZHAO CN, PENG QX, et al. Expression levels of CD28, CTLA-4, PD-1 and Tim-3 as novel indicators of Tcell immune function in patients with chronic hepatitis B virus infection[J]. Biomed Rep, 2014, 2 (2) :270-274.
|
|
[8] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for chronic hepatitis B:A 2015 update[J]. J Clin Hepatol, 2015, 31 (12) :1941-1960. (in Chinese) 中华医学会肝病学分会, 中华医学会感染病学分会.慢性乙型肝炎防治指南 (2015年更新版) [J].临床肝胆病杂志, 2015, 31 (12) :1941-1960.
|
|
[9] BERNSMEIER C, TRIANTAFYLLOU E, BRENIG R, et al. CD14+CD15-HLA-DR-myeloid-derived suppressor cells impair antimicrobial responses in patients with acute-on-chronic liver failure[J]. Gut, 2018, 67 (6) :1155-1167.
|
|
[10] KAMATH PS, WIESNER RH, MALINCHOC M, et al. A model to predict survival in patients with end-stage liver disease[J]. Hepatology, 2001, 33 (2) :464-470.
|
|
[11] LIU J, HILL BJ, DARKO S, et al. The peripheral differentiation of human natural killer T cells[J]. Immunol Cell Biol, 2019, 97 (6) :586-596.
|
|
[12] ZHANG CP, ZHANG D. Mechanism of intrahepatic T lymphocytes in acute liver injury[J〗]. J Clin Exp Med, 2017, 16 (22) :2278-2281. (in Chinese) 张春盼, 张栋.肝内T淋巴细胞在急性肝损伤中的作用机制[J].临床和实验医学杂志, 2017, 16 (22) :2278-2281.
|
|
[13] HASHEMI V, DOLATI S, HOSSEINI A, et al. Natural killer T cells in Preeclampsia:An updated review[J]. Biomed Pharmacother, 2017, 95:412-418.
|
|
[14] PENG LS, MAO FY, ZHAO YL, et al. Altered phenotypic and functional characteristics of CD3+CD56+NKT-like cells in human gastric cancer[J]. Oncotarget, 2016, 7 (34) :55222-55230.
|
|
[15] WERNER JM, LANG C, SCHERER MN, et al. Distribution of intrahepatic T, NK and CD3 (+) CD56 (+) NKT cells alters after liver transplantation:Shift from innate to adaptive immunity?[J]. Transpl Immunol, 2011, 25 (1) :27-33.
|
|
[16] FABIANI S. Hepatitis B virus infection and interferon-inducible protein-10[J]. Clin Ter, 2015, 166 (3) :e188-e196.
|
|
[17] KARLMARK KR, WASMUTH HE, TRAUTWEIN C, et al. Chemokine-directed immune cell infiltration in acute and chronic liver disease[J]. Expert Rev Gastroenterol Hepatol, 2008, 2 (2) :233-242.
|
|
[18] S’ANCHEZ-FUEYO A, TIAN J, PICARELLA D, et al. Tim-3inhibits T helper type 1-mediated auto-and alloimmune responses and promotes immunological tolerance[J]. Nat Immunol, 2003, 4 (11) :1093-10101.
|
|
[19] ELAHI S, NIKI T, HIRASHIMA M, et al. Galectin-9 binding to Tim-3 renders activated human CD4+T cells less susceptible to HIV-1 infection[J]. Blood, 2012, 119 (18) :4192-4204.
|
|
[20] MOORMAN JP, WANG JM, ZHANG Y, et al. Tim-3 pathway controls regulatory and effector T cell balance during hepatitis C virus infection[J]. J Immunol, 2012, 189 (2) :755-766.
|
|
[21] XU Y, WANG ZH, DU XH, et al. Tim-3 blockade promotes i NKT cell function to inhibit HBV replication[J]. J Cell Mol Med, 2018, 22 (6) :3192-3201.
|
|
[22] RONG YH, WAN ZH, SONG H, et al. Tim-3 expression on peripheral monocytes and CD3+CD16/CD56+natural killerlike T cells in patients with chronic hepatitis B[J]. Tissue Antigens, 2014, 83 (2) :76-81.
|
|
[23] XU Q, HIGGINS T, CEMBROWSKI GS. Limiting the testing of AST a diagnostically nonspecific enzyme[J]. Am J Clin Pathol, 2015, 144 (3) :423-426.
|
|
[24] YU JW, SUN LJ, ZHAO YH, et al. Prediction value of model for end-stage liver disease scoring system on prognosis in patients with acute-on-chronic hepatitis B liver failure after plasma exchange and lamivudine treatment[J]. J Gastroenterol Hepatol, 2008, 23 (8 Pt 1) :1242-1249.
|
|
[25] BAO S, ZHENG J, LI N, et al. Role of interleukin-23 in monocyte-derived dendritic cells of HBV-related acute-onchronic liver failure and its correlation with the severity of liver damage[J]. Clin Res Hepatol Gastroenterol, 2017, 41 (2) :147-155.
|
| 1. | 王锐,白皓天,李娅兰,杨婧. 基于生物信息学筛选并综合分析肝细胞癌关键基因. 海南医学院学报. 2022(21): 1634-1643 .  | |
| 2. | 陈雪岩,乔建梁,李军,牛剑祥,赵建国,韩赛,孟兴凯. 小野寺预后营养指数对消化系统恶性肿瘤预后预测价值的研究进展. 中华消化外科杂志. 2022(10): 1390-1394 . | |
| 3. | 陈新宽,杨海燕,梁伟. NuSAP1、LDLR与局部晚期乳腺癌患者腋窝淋巴结转移的关系及其危险因素分析. 肿瘤代谢与营养电子杂志. 2022(06): 747-752 . |


The first journal specializing in hepatobiliary and pancreatic diseases in China
Supervisor:Ministry of Education of the People's Republic of China
Sponsor:Jilin University
Academic Support: Chinese Society of Hepatology,Chinese Medical Association
Address: 461 Xinjiang Road, Changchun
Submit:0431-88782044
Peer review:0431-88783542
Email:lcgdb@vip.163.com
Website Design © 2020 Editorial Board of Journal of Clinical Hepatology
吉ICP备10000617号-1
Supported by: Beijing Renhe Information Technology Co. Ltd

LI YJ, WANG S, WANG N, et al. Clinical efficacy of Jiedu Huayu Hushen prescription in treatment of acute-on-chronic liver failure complicated by hepatorenal syndrome[J]. J Clin Hepatol, 2023, 39(9): 2151-2157. DOI: 10.3969/j.issn.1001-5256.2023.09.018.

| 项目 | 高表达(n=29) | 低表达(n=13) | χ2值 | P值 |
| 性别(例) | 0.022 | 0.88 | ||
| 男 | 24 | 11 | ||
| 女 | 5 | 2 | ||
| 血型(例) | 0.628 | 0.89 | ||
| O型 | 5 | 3 | ||
| A型 | 11 | 5 | ||
| B型 | 12 | 5 | ||
| AB型 | 1 | 0 | ||
| 年龄 | 2.143 | 0.14 | ||
| <50岁 | 16 | 4 | ||
| ≥50岁 | 13 | 9 | ||
| BMI | 0.633 | 0.43 | ||
| 18.5~23.9 kg/m2 | 14 | 8 | ||
| <18.5 kg/m2或≥24 kg/m2 | 15 | 5 | ||
| AFP(例) | 0.252 | 0.62 | ||
| <20 ng/ml | 11 | 6 | ||
| ≥20 ng/ml | 18 | 7 | ||
| MELD评分(例) | 0.032 | 0.86 | ||
| <20分 | 17 | 8 | ||
| ≥30分 | 12 | 5 | ||
| Child-Pugh分级(例) | 5.469 | 0.02 | ||
| A级 | 7 | 8 | ||
| B或C级 | 22 | 5 | ||
| 肿瘤数目(例) | 0.001 | 0.97 | ||
| 单发 | 11 | 5 | ||
| 多发 | 18 | 8 | ||
| TNM分期(例) | 6.836 | 0.01 | ||
| Ⅰ期 | 3 | 6 | ||
| Ⅱ或Ⅲ期 | 26 | 7 | ||
| Okuda分期(例) | 4.617 | 0.03 | ||
| Ⅰ | 6 | 7 | ||
| Ⅱ或Ⅲ | 23 | 6 |
 下载:
下载:


 DownLoad:
DownLoad: