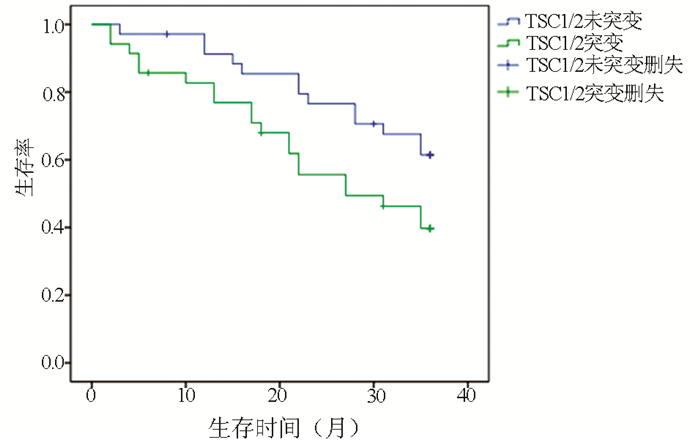
Objective To investigate the association of tuberous sclerosis gene 1/2 (TSC1/2) mutation with disease severity and prognosis in patients with hepatocellular carcinoma (HCC), and to provide a feasible basis for the diagnosis and treatment of HCC.Methods A total of 492 patients with HCC who were admitted to The Affiliated Hospital of Jiangsu University from January 2012 to January 2020 were enrolled, among whom 59 had TSC1/2 mutations (20 with TSC1 mutations, 41 with TSC2 mutations, and 2 had both TSC1 and TSC2 mutations). The clinical features of patients with TSC1/2 mutations were analyzed, and the association of TSC1/2 mutations with the clinical stage of HCC was analyzed. The 35 patients in the mutation group and 35 in the non-mutation group were followed up for 3 years to observe the effect of TSC1/2 mutations on the prognosis of HCC. The chi-square test was used for comparison of categorical data between groups; the Kruskal-Wallis H test was used for comparison of ranked data between groups; a multivariate logistic regression analysis was used to investigate association; the Kaplan-Meier survival analysis was used to analyze follow-up data.Results For the 492 patients with HCC, the overall TSC1/2 mutation rate was 11.99%. There were no significant differences in sex, age, Child score, and tumor size between the TSC1/TSC2 mutation group and the non-mutation group (all P > 0.05), while there were significant differences in tumor number, extrahepatic metastasis, and PS score between the two groups (all P < 0.05). The logistic regression analysis showed that TSC1/TSC2 gene mutation was positively correlated with the severity of HCC (odds ratio=1.706, P < 0.05). The follow-up results showed that the TSC1/2 mutation group had a significantly lower survival rate than the non-mutation group, and there was a significant difference in 3-year mortality rate between the TSC1/2 mutation group and the non-mutation group (60.3% vs 38.6%, χ2=3.923, P < 0.05).Conclusion TSC1/TSC2 gene mutation may predict the malignant progression of HCC in the early stage, and patients with TSC1/2 mutation tend to have poor prognosis. Targeted drug therapy for gene mutations may have a certain effect in delaying the progression of HCC.
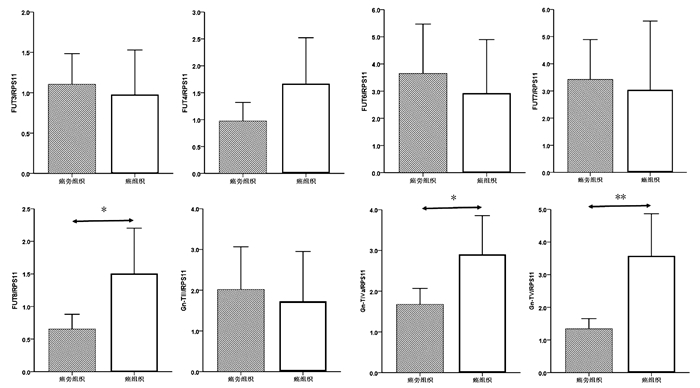
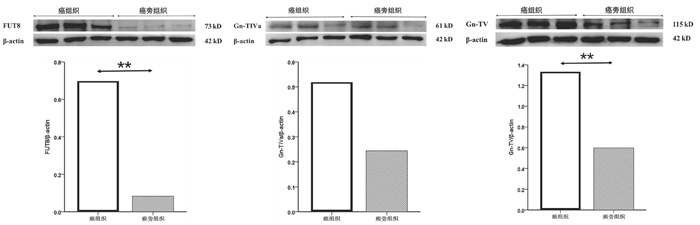
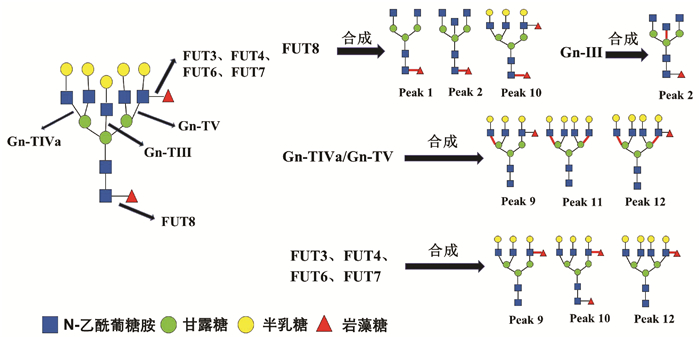
癌组织中FUT8、Gn-TⅣa和Gn-TⅤ基因mRNA表达水平显著高于癌旁组织(1.50±0.34 vs 0.65± 0.11, t=-2.354,P=0.022; 2.90±0.47 vs 1.68±0.19, t=-2.403,P=0.019; 3.57±0.64 vs 1.33±0.16, t=-3.384,P=0.001),差异均有统计学意义。FUT3、FUT4、FUT6、FUT7和Gn-TⅢ mRNA的表达水平在癌组织与癌旁组织间比较差异均无统计学意义(P值均>0.05)(图 2)。
BUDNY A, KOZŁOWSKI P, KAMIN'SKA M, et al. Epidemiology and risk factors of hepatocellular carcinoma[J]. Pol Merkur Lekarski, 2017, 43(255): 133-139.
[2]
ZHU AX, WALLNER KE, FRIVOLD GP, et al. Prostate brachytherapy seed migration to the right coronary artery associated with an acute myocardial infarction[J]. Brachytherapy, 2006, 5(4): 262-265. DOI: 10.1016/j.brachy.2006.08.004
[3]
CROCETTI L, BARGELLINI I, CIONI R. Loco-regional treatment of HCC: Current status[J]. Clin Radiol, 2017, 72(8): 626-635. DOI: 10.1016/j.crad.2017.01.013
[4]
ALGHAMDI MA, LEE YR, SWIHA M, et al. The effect of sorafenib (S) starting dose and dose intensity on survival in patients with advanced hepatocellular carcinoma (HCC)[J]. J Clin Oncol, 2017, 9(14): 4918-4928.
[5]
KAPLAN DE, YU S, TADDEI TH, et al. Up-titration of sorafenib for hepatocellular carcinoma: Impact on duration of exposure and cost[J]. J Clin Oncol, 2017, 35: 385.
[6]
CLARK JW, EDER JP, RYAN D, et al. Safety and pharmacokinetics of the dual action Raf kinase and vascular endothelial growth factor receptor inhibitor, BAY 43-9006, in patients with advanced, refractory solid tumors[J]. Clin Cancer Res, 2005, 11(15): 5472-5480. DOI: 10.1158/1078-0432.CCR-04-2658
[7]
STRUMBERG D, AWADA A, HIRTE H, et al. Pooled safety analysis of BAY 43-9006 (sorafenib) monotherapy in patients with advanced solid tumours: Is rash associated with treatment outcome?[J]. Eur J Cancer, 2006, 42(4): 548-556. DOI: 10.1016/j.ejca.2005.11.014
[8]
ZUCMAN-ROSSI J, VILLANUEVA A, NAULT JC, et al. Genetic landscape and biomarkers of hepatocellular carcinoma[J]. Gastroenterology, 2015, 149(5): 1226-1239.e4. DOI: 10.1053/j.gastro.2015.05.061
[9]
JOZWIAK J, JOZWIAK S, WLODARSKI P. Possible mechanisms of disease development in tuberous sclerosis[J]. Lancet Oncol, 2008, 9(1): 73-79. DOI: 10.1016/S1470-2045(07)70411-4
[10]
NORTHRUP H, KRUEGER DA, International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: Recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference[J]. Pediatr Neurol, 2013, 49(4): 243-254. DOI: 10.1016/j.pediatrneurol.2013.08.001
XU B, ZHANG Q, JIN J. Laparoscopic aspiration for central renal angiomyolipoma: A novel technique based on single-center initial experience[J]. Urology, 2013, 81(2): 313-318. DOI: 10.1016/j.urology.2012.09.047
[13]
HO DWH, CHAN LK, CHIU YT, et al. TSC1/2 mutations define a molecular subset of HCC with aggressive behaviour and treatment implication[J]. Gut, 2017, 66(8): 1496-1506. DOI: 10.1136/gutjnl-2016-312734
[14]
Chinese Society of Clinical Oncology. CSCO guidelines for diagnosis and treatment of hepatocellular carcinoma(2020)[M]. Beijing: China People's Health Press, 2020: 28-29. (in Chinese)
CALDERARO J, COUCHY G, IMBEAUD S, et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification[J]. J Hepatol, 2017, 67(4): 727-738. DOI: 10.1016/j.jhep.2017.05.014
[16]
NISHIDA N, KUDO M. Oncogenic signal and tumor microenvironment in hepatocellular carcinoma[J]. Oncology, 2017, 93(Suppl 1): 160-164.
[17]
DIBBLE CC, MANNING BD. Signal integration by mTORC1 coordinates nutrient input with biosynthetic output[J]. Nat Cell Biol, 2013, 15(6): 555-564. DOI: 10.1038/ncb2763
[18]
HOWELL JJ, RICOULT SJ, BEN-SAHRA I, et al. A growing role for mTOR in promoting anabolic metabolism[J]. Biochem Soc Trans, 2013, 41(4): 906-912. DOI: 10.1042/BST20130041
[19]
European Chromosome 16 Tuberous Sclerosis Consortium. Identification and characterization of the tuberous sclerosis gene on chromosome 16[J]. Cell, 1993, 75(7): 1305-1315. DOI: 10.1016/0092-8674(93)90618-Z
[20]
CRINO PB, NATHANSON KL, HENSKE EP. The tuberous sclerosis complex[J]. N Engl J Med, 2006, 355(13): 1345-1356. DOI: 10.1056/NEJMra055323
[21]
NABBOUT R, BELOUSOVA E, BENEDIK MP, et al. Epilepsy in tuberous sclerosis complex: Findings from the TOSCA Study[J]. Epilepsia Open, 2019, 4(1): 73-84. DOI: 10.1002/epi4.12286
[22]
JANSEN AC, BELOUSOVA E, BENEDIK MP, et al. Clinical characteristics of subependymal giant cell astrocytoma in tuberous sclerosis complex[J]. Front Neurol, 2019, 10: 705. DOI: 10.3389/fneur.2019.00705
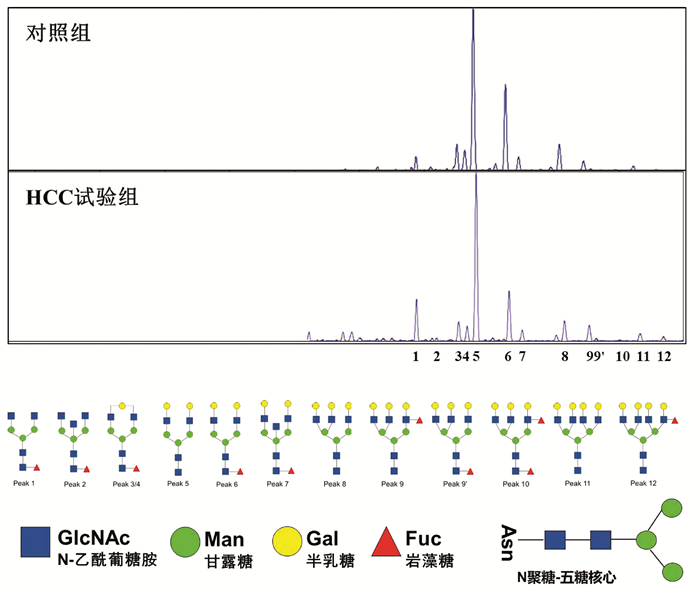
CAO X, SUN YL, CHEN CY, et al. Association between the alteration of serum N-glycan profile and the change of glycosyltransferase expression in liver tissue in patients with hepatitis B virus-related hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(6): 1336-1341. DOI: 10.3969/j.issn.1001-5256.2021.06.024.
CAO X, SUN YL, CHEN CY, et al. Association between the alteration of serum N-glycan profile and the change of glycosyltransferase expression in liver tissue in patients with hepatitis B virus-related hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(6): 1336-1341. DOI: 10.3969/j.issn.1001-5256.2021.06.024.
 下载:
下载:






 DownLoad:
DownLoad: