Value of alpha-fetoprotein combined with gamma-glutamyl transpeptidase/aspartate aminotransferase ratio in diagnosis of HBV-associated hepatocellular carcinoma
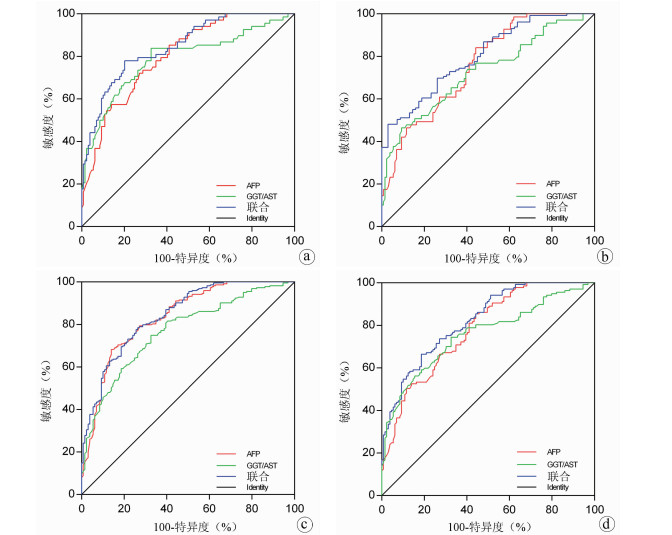
Objective To investigate the clinical value of alpha-fetoprotein (AFP) combined with gamma-glutamyl transpeptidase (GGT)/aspartate aminotransferase (AST) ratio in the diagnosis of hepatitis B virus (HBV)-associated hepatocellular carcinoma (HCC).Methods A total of 352 subjects who received treatment or underwent physical examination in Renmin Hospital of Wuhan University from January 15 to June 15, 2020, were enrolled, among whom there were 86 healthy controls (HC group), 68 patients with chronic hepatitis B (CHB group), 69 patients with liver cirrhosis (LC group), and 129 patients with HCC (HCC group), and a retrospective analysis was performed for the serological test results of all subjects. An analysis of variance was used for comparison of normally distributed continuous data between multiple groups, and the least significant difference t-test was used for further comparison between two groups; the Kruskal-Wallis H test was used for comparison of continuous data with skewed distribution between multiple groups, and the Nemenyi method was used for further comparison between two groups. A binary logistic regression analysis was used to calculate predictor variables; a receiver operating characteristic (ROC) curve was plotted for AFP, GGT/AST, and the predictor variables used alone or in combination, and the area under the ROC curve (AUC), sensitivity, and specificity were calculated; the Z test was used for comparison of AUC.Results The HCC group had significantly higher GGT/AST ratio and AFP than the other groups (all P < 0.05). The ROC curve analysis showed that AFP combined with GGT/AST ratio had a significantly higher AUC than AFP alone in the HCC group vs the LC group, the HCC group vs the HC+CHB+LC groups, and the HCC group vs the CHB+LC groups (Z=2.684, 2.241, and 2.415, P=0.007, 0.025, and 0.016).Conclusion AFP combined with GGT/AST ratio can improve the clinical diagnostic performance of HBV-related HCC and thus has a certain diagnostic value.
Table
3.
Comparison of HBV pgRNA, HBcrAg, HBV DNA and HBsAg levels in circulating serum between relapse group and non relapse group of CHB patients after drug withdrawal
Table
4.
Comparison of HBV pgRNA, HBcrAg expression levels in circulating serum of CHB patients in relapse and non relapse groups at the time of drug withdrawal
CHEN Y, TIAN Z. HBV-induced immune imbalance in the development of HCC[J]. Front Immunol, 2019, 10: 2048. DOI: 10.3389/fimmu.2019.02048.
[2]
ORTEGA-PRIETO AM, DORNER M. Immune evasion strategies during chronic hepatitis B and C virus infection[J]. Vaccines (Basel), 2017, 5(3): 24. DOI: 10.3390/vaccines5030024.
[3]
TAROCCHI M, POLVANI S, MARRONCINI G, et al. Molecular mechanism of hepatitis B virus-induced hepatocarcinogenesis[J]. World J Gastroenterol, 2014, 20(33): 11630-11640. DOI: 10.3748/wjg.v20.i33.11630.
[4]
AFFO S, YU LX, SCHWABE RF. The role of cancer-associated fibroblasts and fibrosis in liver cancer[J]. Annu Rev Pathol, 2017, 12: 153-186. DOI: 10.1146/annurev-pathol-052016-100322.
[5]
DIMITROULIS D, DAMASKOS C, VALSAMI S, et al. From diagnosis to treatment of hepatocellular carcinoma: An epidemic problem for both developed and developing world[J]. World J Gastroenterol, 2017, 23(29): 5282-5294. DOI: 10.3748/wjg.v23.i29.5282.
[6]
National Health and Family Planning Commission of the People' s Republic of China. Diagnosis, management, and treatment of hepatocellular carcinoma (V2017)[J]. J Clin Hepatol, 2017, 33(8): 1419-1431. DOI: 10.3969/j.issn.1001-5256.2017.08.003.
Chinese Journal of Hepatology, Liver Cancer Study Group, Chinese Society of Hepatology, Chinese Medical Association. Expert consensus on multidisciplinary diagnosis and treatment of precancerous lesions of hepatocellular carcinoma(2020 edition)[J]. J Clin Hepatol, 2020, 36(3): 514-518. DOI: 10.3969/j.issn.1001-5256.2020.03.007.
ZHENG Y, ZHU M, LI M. Effects of alpha-fetoprotein on the occurrence and progression of hepatocellular carcinoma[J]. J Cancer Res Clin Oncol, 2020, 146(10): 2439-2446. DOI: 10.1007/s00432-020-03331-6.
[9]
LUO P, WU S, YU Y, et al. Current status and perspective biomarkers in AFP negative HCC: Towards screening for and diagnosing hepatocellular carcinoma at an earlier stage[J]. Pathol Oncol Res, 2020, 26(2): 599-603. DOI: 10.1007/s12253-019-00585-5.
[10]
SONG P, TOBE RG, INAGAKI Y, et al. The management of hepatocellular carcinoma around the world: A comparison of guidelines from 2001 to 2011[J]. Liver Int, 2012, 32(7): 1053-1063. DOI: 10.1111/j.1478-3231.2012.02792.x.
[11]
GALLE PR, FOERSTER F, KUDO M, et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma[J]. Liver Int, 2019, 39(12): 2214-2229. DOI: 10.1111/liv.14223.
[12]
WANG T, ZHANG KH. New blood biomarkers for the diagnosis of AFP-negative hepatocellular carcinoma[J]. Front Oncol, 2020, 10: 1316. DOI: 10.3389/fonc.2020.01316.
[13]
GAO C, FANG L, YAO SK. Correlation of GGT with AFP and diagnostic value of GGT for hepatocellular carcinoma[J]. J Clin Hepatol, 2014, 30(9): 921-925. DOI: 10.3969/j.issn.1001-5256.2014.09.021.
XIA J, SONG P, SUN Z, et al. Advances of diagnostic and mechanistic studies of γ-glutamyl transpeptidase in hepatocellular carcinoma[J]. Drug Discov Ther, 2016, 10(4): 181-187. DOI: 10.5582/ddt.2016.01052.
[15]
ZHOU L, WANG SB, CHEN SG, et al. Prognostic value of ALT, AST, and AAR in hepatocellular carcinoma with B-type hepatitis-associated cirrhosis after radical hepatectomy[J]. Clin Lab, 2018, 64(10): 1739-1747. DOI: 10.7754/Clin.Lab.2018.180532.
[16]
YANG JG, HE XF, HUANG B, et al. Rule of changes in serum GGT levels and GGT/ALT and AST/ALT ratios in primary hepatic carcinoma patients with different AFP levels[J]. Cancer Biomark, 2018, 21(4): 743-746. DOI: 10.3233/CBM-170088.
ZHANG SW, CHEN X, LIU J, et al. Expression levels of HBV pregenomic RNA and hepatitis B core-related antigen in circulating serum and their association with recurrence in chronic hepatitis B patients after withdrawal from nucleos(t)ide analogues[J]. J Clin Hepatol, 2023, 39(1): 56-62. DOI: 10.3969/j.issn.1001-5256.2023.01.009.
ZHANG SW, CHEN X, LIU J, et al. Expression levels of HBV pregenomic RNA and hepatitis B core-related antigen in circulating serum and their association with recurrence in chronic hepatitis B patients after withdrawal from nucleos(t)ide analogues[J]. J Clin Hepatol, 2023, 39(1): 56-62. DOI: 10.3969/j.issn.1001-5256.2023.01.009.
Table
3.
Comparison of HBV pgRNA, HBcrAg, HBV DNA and HBsAg levels in circulating serum between relapse group and non relapse group of CHB patients after drug withdrawal
Table
4.
Comparison of HBV pgRNA, HBcrAg expression levels in circulating serum of CHB patients in relapse and non relapse groups at the time of drug withdrawal

 下载:
下载:






 DownLoad:
DownLoad: