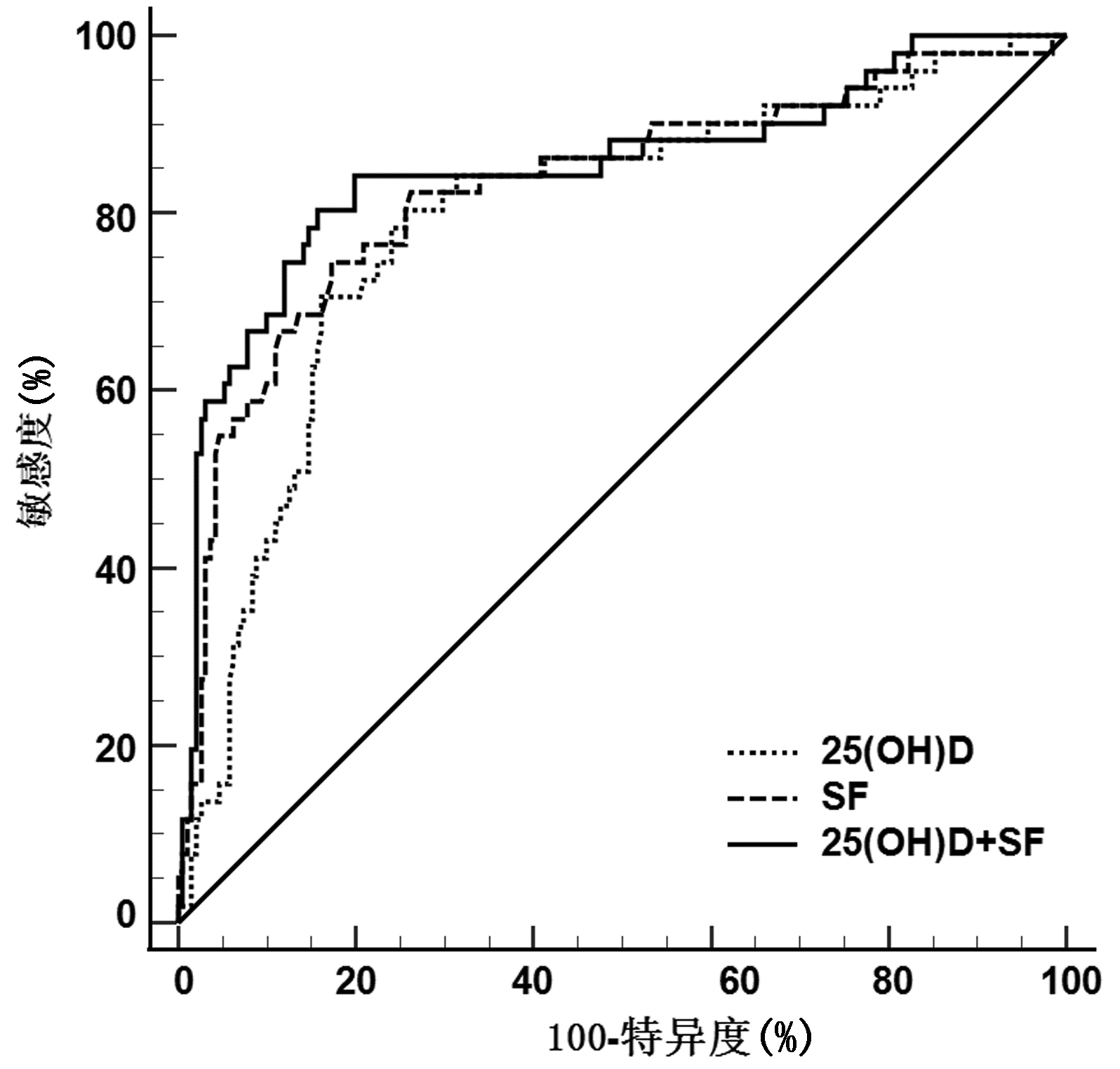
Objective To investigate the association of serum 25-hydroxyvitamin D [25(OH)D] and serum ferritin (SF) with metabolic associated fatty liver disease (MAFLD) and fibrosis-4 (FIB-4) index.Methods A retrospective analysis was performed for the clinical data of 595 patients who were hospitalized in Department of Gastroenterology, Wuhan Hankou Hospital, from August 2020 to December 2021. Clinical features were compared between 242 patients with MAFLD and 353 patients without MAFLD, and the prevalence rate of MAFLD and SF level were compared between the groups with different 25(OH)D levels. The non-normally distributed continuous data were expressed as M(P25-P75), and the Mann-Whitney U test was used for comparison between two groups; the chi-square test was used for comparison of categorical data between groups. A Spearman correlation analysis was used to investigate the correlation between serum 25(OH)D and SF in different populations; a binary logistic regression analysis was used to investigate the association of 25(OH)D and SF with the risk of MAFLD and FIB-4 index; the receiver operating characteristic (ROC) curves were used to assess the value of 25(OH)D and SF in the diagnosis of liver fibrosis in patients with MAFLD.Results Compared with the non-MAFLD patients, the MAFLD patients had a significant reduction in serum 25(OH)D level [15.35(11.26-20.02) vs 21.71(15.39-27.84), Z=-9.761, P < 0.05] and a significant increase in SF level [365.50(251.75-525.00) vs 205.00(112.50-275.00), Z=-13.317, P < 0.05]. The prevalence rate of MAFLD and SF level tended to increase with the reduction in serum 25(OH)D level (Z=75.512, P < 0.05). Serum 25(OH)D level was significantly negatively correlated with SF in MAFLD patients (r=-0.460, P < 0.05). The logistic regression analysis showed that the reduction in serum 25(OH)D level (odds ratio [OR]=0.934, 95% confidence interval [CI]: 0.879-0.992, P=0.028) and the increase in SF level (OR=1.009, 95%CI: 1.006-1.013, P < 0.001) were independent risk factors for MAFLD, and the reduction in serum 25(OH)D level (OR=0.852, 95%CI: 0.752-0.965, P=0.012) was also an independent risk factor for elevated FIB-4 index (> 2.67) in MAFLD patients. The ROC curve analysis showed that serum 25(OH)D, SF, and their combination had an area under the ROC curve of 0.793, 0.829, and 0.851, respectively, in predicting elevated FIB-4 index (> 2.67) in MAFLD patients (all P < 0.05).Conclusion Serum 25(OH)D is negatively correlated with SF, and the reduction in serum 25(OH)D and the increase in SF are associated with the risk of MAFLD and elevated FIB-4 index. Serum 25(OH)D and SF levels have a certain value in predicting liver fibrosis in patients with MAFLD.
LAZARUS JV, MARK HE, ANSTEE QM, et al. Advancing the global public health agenda for NAFLD: A consensus statement[J]. Nat Rev Gastroenterol Hepatol, 2022, 19(1): 60-78. DOI: 10.1038/s41575-021-00523-4.
[2]
DU SX, LU LL, GENG N, et al. Association of serum ferritin with non-alcoholic fatty liver disease: A meta-analysis[J]. Lipids Health Dis, 2017, 16(1): 228. DOI: 10.1186/s12944-017-0613-4.
[3]
ALI SANGOUNI A, GHAVAMZADEH S, JAMALZEHI A. A narrative review on effects of vitamin D on main risk factors and severity of non-alcoholic fatty liver disease[J]. Diabetes MetabSyndr, 2019, 13(3): 2260-2265. DOI: 10.1016/j.dsx.2019.05.013.
[4]
ESLAM M, NEWSOME PN, SARIN SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement[J]. J Hepatol, 2020, 73(1): 202-209. DOI: 10.1016/j.jhep.2020.03.039.
[5]
LIN S, HUANG JF, WANG MF, et al. Comparison of MAFLD and NAFLD diagnostic criteria in real world[J]. Liver Int, 2020, 40(9): 2082-2089. DOI: 10.1111/liv.14548.
[6]
CIARDULLO S, PERSEGHIN G. Prevalence of NAFLD, MAFLD and associated advanced fibrosis in the contemporary United States population[J]. Liver Int, 2021, 41(6): 1290-1293. DOI: 10.1111/liv.14828.
[7]
SHAH AG, LYDECKER A, MURRAY K, et al. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease[J]. Clin Gastroenterol Hepatol, 2009, 7(10): 1104-1112. DOI: 10.1016/j.cgh.2009.05.033.
[8]
LIAO XP, ZHANG ZL, ZHANG HH, et al. Application guideline for vitamin D and bone health in adult Chinese(2014 standard edition) vitamin D working group of osteoporosis committee of China gerontological society[J]. Chin J Osteoporos, 2014, 20(9): 1011-1030. DOI: 10.3969/j.issn.1006-7108.2014.09.002.
ZHOU Q, LI JQ, LI XW. Influence of vitamin D deficiency on fibrosis-4 index and disease severity in patients with nonalcoholic steatohepatitis[J]. J Clin Hepatol, 2022, 38(6): 1293-1298. DOI: 10.3969/j.issn.1001-5256.2022.06.015.
SUN CJ, ZUO XQ, YAO N, et al. Study on the correlation between serum ferritin and non-alcoholic fatty liver disease[J]. Zhejiang J Integr Tradit Chin West Med, 2019, 29(5): 371-375. DOI: 10.3969/j.issn.1005-4561.2019.05.008.
BACCHETTA J, ZARITSKY JJ, SEA JL, et al. Suppression of iron-regulatory hepcidin by vitamin D[J]. J Am Soc Nephrol, 2014, 25(3): 564-572. DOI: 10.1681/ASN.2013040355.
[12]
LIU ZP, ZHANG JH, WANG XN, et al. Effect of vitamin D on serum markers of iron metabolism in patients with non-alcoholic fatty liver disease[J]. Tianjin Med J, 2018, 46(12): 1316-1318. DOI: 10.11958/20180847.
PATEL YA, GIFFORD EJ, GLASS LM, et al. Identifying nonalcoholic fatty liver disease advanced fibrosis in the veterans health administration[J]. Dig Dis Sci, 2018, 63(9): 2259-2266. DOI: 10.1007/s10620-018-5123-3.
[14]
MA XH, ZHANG X, YOU Y, et al. Diagnostic value of APRI combined with FIB-4 for significant liver fibrosis in patients with chronic hepatitis B[J]. Chin J Gastroenterol, 2017, 22(9): 544-547. DOI: 10.3969/j.issn.1008-7125.2017.09.007.
YANG BB, CHEN YH, ZHANG C, et al. Low vitamin D status is associated with advanced liver fibrosis in patients with nonalcoholic fatty liver disease[J]. Endocrine, 2017, 55(2): 582-590. DOI: 10.1007/s12020-016-1152-x.
[16]
UDOMSINPRASERT W, JITTIKOON J. Vitamin D and liver fibrosis: Molecular mechanisms and clinical studies[J]. Biomed Pharmacother, 2019, 109: 1351-1360. DOI: 10.1016/j.biopha.2018.10.140.
[17]
KOWDLEY KV, BELT P, WILSON LA, et al. Serum ferritin is an independent predictor of histologic severity and advanced fibrosis in patients with nonalcoholic fatty liver disease[J]. Hepatology, 2012, 55(1): 77-85. DOI: 10.1002/hep.24706.
[18]
BUZZETTI E, PETTA S, MANUGUERRA R, et al. Evaluating the association of serum ferritin and hepatic iron with disease severity in non-alcoholic fatty liver disease[J]. Liver Int, 2019, 39(7): 1325-1334. DOI: 10.1111/liv.14096.
[19]
YONEDA M, THOMAS E, SUMIDA Y, et al. Clinical usage of serum ferritin to assess liver fibrosis in patients with non-alcoholic fatty liver disease: Proceed with caution[J]. Hepatol Res, 2014, 44(14): E499-E502. DOI: 10.1111/hepr.12327.
[20]
ZENG J, FAN JG. Clinical significance of renaming nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2020, 36(6): 1205-1207. DOI: 10.3969/j.issn.1001-5256.2020.06.002.
CAI X, CHEN JJ, TANG DL, et al. Value of alpha-fetoprotein combined with gamma-glutamyl transpeptidase/aspartate aminotransferase ratio in diagnosis of HBV-associated hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(9): 2109-2112. DOI: 10.3969/j.issn.1001-5256.2021.09.021.
CAI X, CHEN JJ, TANG DL, et al. Value of alpha-fetoprotein combined with gamma-glutamyl transpeptidase/aspartate aminotransferase ratio in diagnosis of HBV-associated hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(9): 2109-2112. DOI: 10.3969/j.issn.1001-5256.2021.09.021.

 下载:
下载:








 DownLoad:
DownLoad: