Objective To evaluate the clinical effect of artificial liver support system ( ALSS) on serum high-sensitivity C-reactive protein ( hs-CRP) level and investigate the influence of the change in hs-CRP level on clinical prognosis among patients with hepatic failure.Methods Patients were recruited into three groups: group one included 60 patients who received ALSS due to hepatic failure; group two included 37 patients with hepatic failure without ALSS treatment; and group three included 37 patients with chronic hepatitis B. The serum levels of hs-CRP were measured in groups two and three, and in group one before and after ALSS treatment. Comparison of continuous data between groups was made by t test, and comparison of categorical data was made by chi-square test. Results The levels of hs-CRP in group one before treatment and in groups two and three were 12. 89 ± 9. 39, 12. 22 ± 9. 73, and 2. 83 ± 6. 79, respectively. No significant difference in hs-CRP level between group one and group two was observed ( P > 0. 05) . However, the hs-CRP level in group three was significantly different from those in group one and group two ( P < 0. 001) . The improvement rate in group one after ALSS treatment ( 78.3%) was significantly higher compared with that in group two ( 54.05%) ( χ2= 6. 315, P < 0. 05) . ALSS treatment ( t = 5. 179, P <0. 05) . ALSS treatment was selectively effective in a subgroup of patients and greatly decreased the hs-CRP level in these patients ( t =5. 344, P = 0. 000) , resulting in a significant difference from the patients who were unresponsive to ALSS treatment ( t = 2. 368, P =0. 038) . Conclusion Artificial liver support system can decrease the hs-CRP level in patients with hepatic failure. Serum level of hs-CRP can be used as a clinical indicator of disease progression and predict the clinical outcomes of ALSS in patients with hepatic failure.
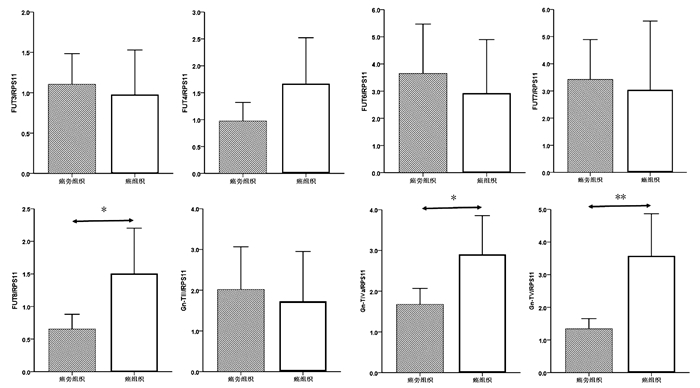
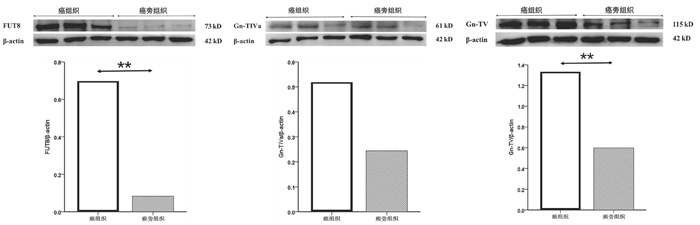
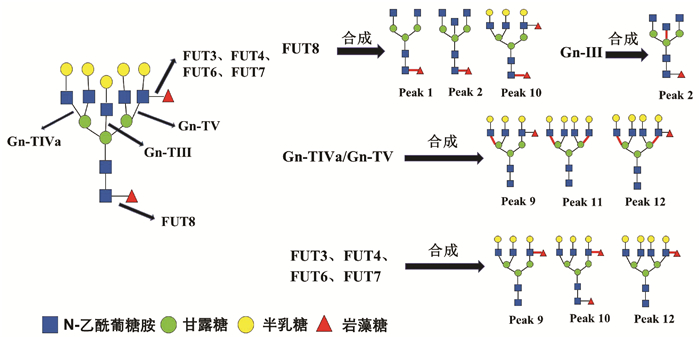
癌组织中FUT8、Gn-TⅣa和Gn-TⅤ基因mRNA表达水平显著高于癌旁组织(1.50±0.34 vs 0.65± 0.11, t=-2.354,P=0.022; 2.90±0.47 vs 1.68±0.19, t=-2.403,P=0.019; 3.57±0.64 vs 1.33±0.16, t=-3.384,P=0.001),差异均有统计学意义。FUT3、FUT4、FUT6、FUT7和Gn-TⅢ mRNA的表达水平在癌组织与癌旁组织间比较差异均无统计学意义(P值均>0.05)(图 2)。
[1]LI LJ.Difficulties and focuses in the treatment of liver failure[J].Chin J Hepatol, 2012, 20 (6) :405-407. (in Chinese) 李兰娟.肝衰竭临床治疗中的难点和热点[J].中华肝脏病杂志, 2012, 20 (6) :405-407.
[2] Liver Failure and Artificial liver Group, Chinese Society of Infectious Diseases, Chinese Medical Association;Severe Liver Diseases and Artificial liver Group, Chinese Society of Hepatology, Chinese Medical Association.Diagnostic and treatment guidelines for liver failure[J].Chin J Clin Infect Dis, 2012, 5 (6) :321-327. (in Chinese) 中华医学会感染病学分会肝衰竭与人工肝学组, 中华医学会, 肝病学分会重型肝病与人工肝学组.肝衰竭诊治指南 (2012年版) [J].中华临床感染病杂志, 2012, 5 (6) :321-327.
[3]LIANG ZH.Value of high-sensitivity C-reactive protein in diagnosis of liver diseases[J].China Modern Med, 2010, 17 (18) :74-75. (in Chinese) 梁展华.超敏C-反应蛋白在肝病诊断中的应用价值[J].中国当代医药, 2010, 17 (18) :74-75.
[4]SASAKI K, FUJITA I, HAMASAKI Y, et al.Differentiating between bacterial and viral infection by measuring both C-reactive protein and2’-5’-oligoa-denylate synthetase inflammatory markers[J].J Infect Chemother, 2002, 8 (1) :76-80.
[5] YE YN, GAO ZL.Three shock hypotheses that may induce liver failure[J].Chin J Hepatol, 2009, 17 (8) :638-640. (in Chinese) 叶一农, 高志良.乙型肝炎肝衰竭发生机制中的三重打击[J].中华肝脏病杂志, 2009, 17 (8) :638-640.
[6]HAN DW.Enterogenous endotoxin hematic disease and liver disease[M].Beijing:China Science and Technology Press, 2004. (in Chinese) 韩德五.肠源性内毒素血症与肝病[M].北京:中国科学技术出版社, 2004.
[7]ROCEN M, KIESLIEHOVA E, MERTA D, et al.The effect of Prometheus device on laboratory markers of inflammation and tissue regeneration in acute liver failure management[J].Transplant Proc, 2010, 42 (9) :3606-3611.
[8]WANG MX.Changes in C-reactive protein among 124 patients with chronic severe hepatitis[J].Lab Med Clin, 2011, 8 (1) :2234-2235. (in Chinese) 汪明星.C反应蛋白在124例慢性重型肝炎中的变化[J].检验医学与临床, 2011, 8 (1) :2234-2235.
[9]MAO WL, CHEN Y, CHEN YM, et al.Change of serum cytokine levels in patients with acute on chronic liver failure treated by plasma exchange[J].J Clin Gastroenterol, 2011, 45 (6) :551-555.
[10]LI TY, WANG WJ, ZHANG SP, et al.Expressions of IL-18、IL-12 and IFN-γin chronic severe hepatitis and treatment with artificial liver support system[J].Jiangsu Med J, 2008, 34 (5) :438-440. (in Chinese) 李天一, 叶卫江, 张松平, 等.慢性重型肝炎患者血清IL-18、IL-12和IFN-γ的表达及人工肝治疗[J].江苏医药, 2008, 34 (5) :438-440.
[11]WANG YC, ZHANG M, LI YQ, et al.Clinical efficacy of artifical liver (plasma exchange) in treatment of liver failure among patients with chronic severe hepatitis[J].Chin Hepatol, 2012, 17 (8) :570-571. (in Chinese) 王英超, 张敏, 李永勤, 等.人工肝 (血浆置换) 治疗慢性重型肝炎肝功能衰竭的临床初探[J].肝脏, 2012, 17 (8) :570-571.
[12]WANG XH, YE YN, LIANG MF, et al.Plasma exchange combined with hemofiltration influences serum levels of IL-17 and IL-6 in patients with HBV-related acute-on-chronic liver failure[J].J Clin Hepatol, 2012, 28 (10) :756-763. (in Chinese) 王向槐, 叶一农, 梁敏锋, 等.血浆置换联合血液滤过对乙型肝炎相关慢加急性肝衰竭患者血清IL-17和IL-6的影响[J].临床肝胆病杂志, 2012, 28 (10) :756-763.
[13]ZHOU J, WAN H.Relationship between changes in serum cytokine levels after artificial liver therapy and clinical prognosis in patients with liver failure[J].J Clin Hepatol, 2013, 29 (7) :535-537. (in Chinese) 周渐, 万红.肝衰竭患者血浆置换治疗前后细胞因子的变化与预后的关系[J].临床肝胆病杂志, 2013, 29 (7) :535-537.
CAO X, SUN YL, CHEN CY, et al. Association between the alteration of serum N-glycan profile and the change of glycosyltransferase expression in liver tissue in patients with hepatitis B virus-related hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(6): 1336-1341. DOI: 10.3969/j.issn.1001-5256.2021.06.024.
CAO X, SUN YL, CHEN CY, et al. Association between the alteration of serum N-glycan profile and the change of glycosyltransferase expression in liver tissue in patients with hepatitis B virus-related hepatocellular carcinoma[J]. J Clin Hepatol, 2021, 37(6): 1336-1341. DOI: 10.3969/j.issn.1001-5256.2021.06.024.
 下载:
下载:






 DownLoad:
DownLoad: