图
1
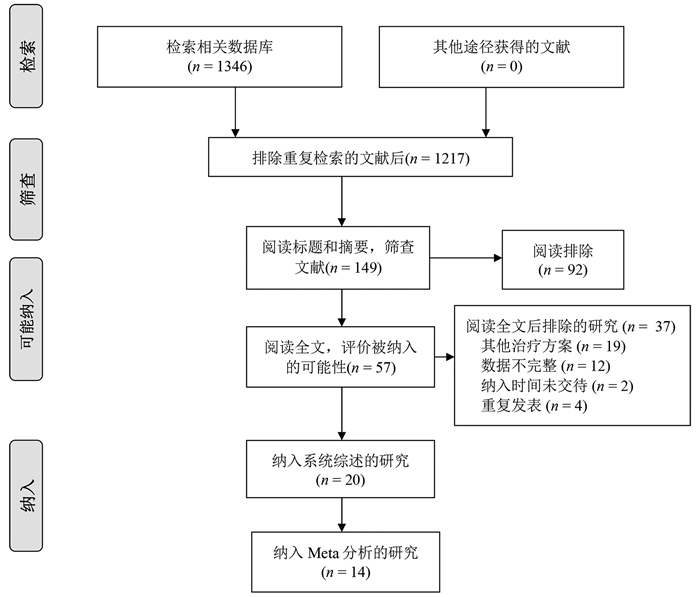
文献检索流程图
肝细胞癌(简称肝癌)术后复发是导致患者死亡的主要原因[1]。对于复发性肝癌,临床上常用的治疗方法包括再次肝切除术、射频消融(radiofrequency ablation,RFA)、肝移植、介入、靶向药物治疗等[2]。然而,目前国内外肝癌诊疗指南均未对复发性肝癌提供具体的诊疗推荐。再次肝切除术和RFA属于根治性治疗方法,临床应用广泛,文献报道较多。但单个研究样本量小,且研究间的结论不统一,临床上对复发性肝癌的根治性治疗方案尚存争议。本文使用Meta分析的方法,客观分析两种治疗措施对复发性肝癌的疗效与安全性。
系统检索PubMed、中国知网和万方数据库,检索日期自建库至2020年6月15日。英文检索词包括:recurrent、recurrence、hepatocellular carcinoma、liver cancer、hepatic resection、hepatectomy、resection、radiofrequency ablation等,中文检索词包括:复发、肝癌、肝细胞癌、手术、再次肝切除术、射频消融等。
(1) 研究:比较再次肝切除术与RFA治疗复发性肝癌的随机对照试验或队列研究,英文或中文发表。(2)患者:罹患原发性肝癌,接受首次肝切除术治疗后,肝癌复发,复发肿瘤符合米兰标准,且无大血管侵犯及肝外转移。(3)干预措施:肝癌复发后,接受再次肝切除术或RFA治疗。(4)结局指标:报道了总生存期(overall survival,OS)、无瘤生存期(recurrence-free survival,RFS)、围手术期并发症和围手术期病死率中的任何一项。
(1) 肝切除和RFA治疗原发性肝癌、胆管细胞癌或转移性肝癌的研究;(2)单组样本量过小(<10例)或单臂研究;(3)未提供病例具体纳入时间段的研究;(4)肝癌复发后,接受再次肝切除术或RFA治疗前,接受其他的治疗方案(如介入、靶向药物等)。再次肝切除术或RFA治疗后,序贯介入或其他治疗措施,不在排除标准范围之内。对于重复性发表的研究,仅纳入样本量最大的一项。
两位评价者独立检索并提取纳入文献的数据,数据提取过程中若有分歧则通过双方讨论或询问第3位评价者解决。提取的数据包括人口统计学资料及临床基线数据、OS、RFS、围手术期并发症发生率及病死率。若原始文献未详细描述生存数据,则从其Kaplan-Meier生存曲线图估算。
统计分析采用RevMan 5.4.1软件(Cochrane协作组,牛津,英国)。采用从纳入文献提取的风险比(HR)进行OS和RFS的Meta分析。统计学异质性的评估采用I2检验。I2≥50%时采用随机效应模型,I2<50%时采用固定效应模型。P<0.05为差异有统计学意义。采用漏斗图估计发表偏倚。由于纳入文献提供的数据存在一定的局限性,无法根据患者性别、肿瘤大小、肿瘤个数、肿瘤位置等进行亚组分析。
根据纳入和排除标准,18篇回顾性队列研究[3-20]和2篇随机对照试验[21-22]比较了再次肝切除术和RFA治疗复发性肝癌的临床疗效与安全性,共2903例患者(图 1)。全部纳入患者均来自亚洲国家,基线数据详见表 1。
| 第一作者和年份 | 国家/地区 | 纳入时间(年) | 组别 | 样本量 | 男/女(例) | 年龄(岁) | 单个/多个肿瘤(例) | 复发肿瘤直径(cm) | 肝硬化[例(%)] | CTP分级(A/B/C,例) | 随访(月) |
| Wang 2015[3] | 中国 | 2004—2010 | 肝切除 | 128 | 113/15 | 50.2±10.1 | 89/39 | 2.4±0.9 | 66(51.6) | - | - |
| RFA | 162 | 148/14 | 52.7±10.9 | 107/55 | 2.3±0.7 | - | - | - | |||
| Sun 2017[4] | 中国台湾 | 2002—2014 | 肝切除 | 43 | 34/9 | 60(35~76) | - | 1.9(0.8~3.0) | 36(83.7) | 42/1 | 53 |
| RFA | 57 | 38/19 | 63(27~81) | - | 1.8(1.0~3.0) | 50(87.7) | 57/0 | 54 | |||
| Umeda 2011[5] | 日本 | 1998—2007 | 肝切除 | 29 | - | - | - | 3.20±0.57 | - | 29/0 | 48 |
| RFA | 58 | - | - | - | 2.1±0.3 | - | 51/7 | 48 | |||
| Song 2015[6] | 韩国 | 1994—2012 | 肝切除 | 39 | 31/8 | 52.5±9.8 | 32/7 | 2.2±1.1 | 23(59) | 39/0 | 36.3(0.8~126.6) |
| RFA | 178 | 145/33 | 55.4±10.6 | 156/22 | 1.7±0.6 | 130(73.0) | 172/6 | 44.7(5.6~139.8) | |||
| Liang 2008[7] | 中国 | 1999—2007 | 肝切除 | 44 | 39/5 | 48.8±12.0 | 34/10 | ≤3 (26) | - | 44/0 | 33.5±24.1 |
| RFA | 66 | 54/12 | 54.6±10.8 | 48/18 | ≤3 (44) | - | 64/2 | 21.1±19.1 | |||
| Ho 2012[8] | 中国台湾 | 2001—2007 | 肝切除 | 54 | 40/14 | 56.3±12.3 | - | 2.9±1.8 | 26(48.1) | 51/2/1 | 32(0~79) |
| RFA | 50 | 39/11 | 61.0±11.1 | - | 2.3±1.9 | 28(56.0) | 50/0 | 27(0~96) | |||
| Chan 2012[9] | 中国香港 | 2001—2008 | 肝切除 | 29 | - | 52(38~79) | 21/8 | 2.1(0.8~5.5) | 25(86.2) | 29/0 | 44.9 |
| RFA | 45 | - | 59(36~80) | 29/16 | 2.2(0.8~6.0) | 40(88.9) | 40/5 | 44.9 | |||
| Chen 2018[10] | 中国 | 2009—2015 | 肝切除 | 48 | 41/7 | 73.5±3.5 | 28/20 | 2.6±1.1 | 41(85.4) | 39/9 | 36.9(2~78) |
| RFA | 57 | 51/6 | 73.7±2.9 | 30/27 | 2.5±1.2 | 49(86.0) | 45/12 | 37.3(2~78) | |||
| 岑峰2016[11] | 中国 | 2011—2015 | 肝切除 | 28 | 22/6 | 53.6 | 12/16 | - | 23(82.1) | 18/10 | - |
| RFA | 24 | 19/5 | 55.7 | 10/14 | - | 19(79.2) | - | - | |||
| 陈康2019[12] | 中国 | 2005—2014 | 肝切除 | 77 | 65/12 | - | - | - | 57(74) | 76/1 | 57(2~168) |
| RFA | 82 | 72/10 | - | - | - | 50(61) | 77/5 | 51(4~111) | |||
| 黄新辉2013[13] | 中国 | 2007—2011 | 肝切除 | 66 | 51/15 | 50.5±10.1 | 66/0 | 2.9±1.1 | 57(86.3) | 66/0 | - |
| RFA | 46 | 36/10 | 54.1±12.1 | 46/0 | 2.6±0.9 | 39(84.8) | 46/0 | - | |||
| 梁惠宏2011[14] | 中国 | 1999—2009 | 肝切除 | 72 | 65/7 | 49±12 | 72/0 | 2.1±0.1 | - | 70/2 | 36±25 |
| RFA | 79 | 69/10 | 55±11 | 79/0 | 2.5±0.1 | - | 73/6 | 32±21 | |||
| 任正刚2008[15] | 中国 | 2000—2005 | 肝切除 | 145 | 127/18 | 51 | 127/18 | 2.0 | - | 145/0 | 23(3~88) |
| RFA | 68 | 64/4 | 52 | 52/16 | 2.0 | - | 68/0 | 23(3~88) | |||
| 田正灵2016[16] | 中国 | 2012—2015 | 肝切除 | 30 | 28/2 | 48.8±9.6 | 24/6 | - | 24(80) | - | 17(6.0~42.5) |
| RFA | 27 | 26/1 | 50.9±10.1 | 19/8 | - | 23(85.2) | - | 17(6.0~42.5) | |||
| 张辉2013[17] | 中国 | 2003—2011 | 肝切除 | 69 | - | - | - | 3.5 | 61(88.4) | 54/15 | - |
| RFA | 99 | - | - | 2.1 | 76(76.8) | 71/28 | - | ||||
| 张婷婷2014[18] | 中国 | 1998—2010 | 肝切除 | 27 | 25/2 | 47±13 | 25/2 | 3.2±1.1 | - | 27/0 | 32(9~118) |
| RFA | 39 | 37/2 | 52±13 | 37/2 | 2.7±1.1 | - | 37/2 | 28(2~79) | |||
| Peng 2018[19] | 中国 | 2006—2015 | 肝切除 | 79 | 67/2 | 55 | 59/20 | ≤3(48) | - | - | 53.2(4~96) |
| RFA | 107 | 95/12 | 57 | 75/32 | ≤3(73) | - | - | 52.3(3~96) | |||
| Lu 2020[20] | 中国 | 2004—2015 | 肝切除 | 138 | 124/16 | 50.1±10.9 | 112/26 | 2.8±1.9 | 96(70) | 138/0 | 37.6 |
| RFA | 194 | 172/22 | 52.9±11.8 | 162/32 | 1.9±0.9 | 134(69) | 194/0 | 41.6 | |||
| Xia 2019[21] | 中国 | 2010—2013 | 肝切除 | 120 | 107/13 | 52.4(25.7~60.5) | 96/24 | 2.9(1.0~5.0) | 50(41.7) | 120/0 | 44.3(4.3~90.6) |
| RFA | 120 | 109/11 | 53.5(28.0~59.9) | 94/26 | 2.7(1.0~4.8) | 55(45.8) | 120/0 | 44.3(4.3~90.6) | |||
| 刘嘉龙2019[22] | 中国 | 2016—2017 | 肝切除 | 39 | 38/1 | 50.0±10.0 | 37/2 | 2.1±0.7 | 37(94.9) | 38/1 | 24 |
| RFA | 41 | 37/4 | 48.9±11.3 | 39/2 | 1.8±0.8 | 39(95.1) | 39/2 | 24 | |||
| 注:-,未报道。 | |||||||||||
15篇文献[4, 6-7, 9-17, 19, 21-22]报道了再次肝切除术围手术期并发症发生率为5.5%~68.2%,中位值为22.4%,常见并发症包括肝功能不全、胸腔积液、腹水、胆瘘等。14篇文献[4, 6-7, 9-10, 12-17, 19, 21-22]报道了RFA的围手术期并发症发生率为0~13%,中位值为3.3%,常见并发症包括胆漏、腹腔出血等。16篇文献[4, 6-7, 9-19, 21-22]报道了再次肝切除术和RFA围手术期病死率,其中6篇文献[4, 6, 10, 12, 17, 19]报道再次肝切除术组围手术期病死率为1.3%~2.6%,中位值为2%,其余文献报道发生率为0;仅1篇文献[9]报道RFA围手术期病死率为2.2%,其余文献报道发生率为0(表 2)。
| 第一作者和年份 | 组别 | 并发症发生率(%) | 围手术期病死率(%) | 复发[例(%)] | RFS | OS | |||||||
| 1年 | 3年 | 5年 | P值1) | 1年 | 3年 | 5年 | P值1) | ||||||
| Wang 2015[3] | 肝切除 | - | - | - | - | - | - | - | 97.7 | 84.1 | 64.5 | <0.001 | |
| RFA | - | - | - | - | - | - | 96.9 | 73.4 | 37.0 | ||||
| Sun 2017[4] | 肝切除 | 16 | 2 | 30(69.8) | 57.0 | 32.1 | 28.6 | 0.89 | 97.6 | 82.7 | 56.4 | 0.69 | |
| RFA | 7 | 0 | 41(71.9) | 60.8 | 26.6 | 16.6 | 98.2 | 77.2 | 52.6 | ||||
| Umeda 2011[5] | 肝切除 | - | - | - | - | - | - | - | 93.1 | 66.8 | 58.1 | 0.899 | |
| RFA | - | - | - | - | - | - | 94.7 | 75.1 | 48.3 | ||||
| Song 2015[6] | 肝切除 | 64 | 2.6 | 18(46.2) | 66.1 | 48.5 | 43.1 | 0.834 | 88.8 | 88.8 | 83.9 | 0.686 | |
| RFA | 2.2 | 0 | 117(65.7) | 70.1 | 40.8 | 30.0 | 98.9 | 82.5 | 71.0 | ||||
| Liang 2008[7] | 肝切除 | 68.2 | 0 | 86.4 | - | - | - | - | 78.6 | 44.5 | 27.6 | 0.79 | |
| RFA | 3.0 | 0 | 78.8 | - | - | - | 76.6 | 48.6 | 39.9 | ||||
| Ho 2012[8] | 肝切除 | - | - | - | - | - | - | - | - | - | 72.0 | - | |
| RFA | - | - | - | - | - | - | - | - | 83.0 | ||||
| Chan 2012[9] | 肝切除 | 24.1 | 0 | 21(72.4) | 41.1 | 24.2 | 24.2 | 0.14 | 89.7 | 56.5 | 35.2 | 0.51 | |
| RFA | 2.2 | 2.2 | 38(84.4) | 32.2 | 12.4 | 9.3 | 83.7 | 43.1 | 29.1 | ||||
| Chen 2018[10] | 肝切除 | 25 | 2.1 | 26(54.2) | 73.1 | 49.7 | 40.7 | 0.465 | 76.3 | 52.5 | 42.6 | 0.413 | |
| RFA | 0 | 0 | 27(47.4) | 69.5 | 37.8 | 33.1 | 78.2 | 40.8 | 36.7 | ||||
| 岑峰2016[11] | 肝切除 | 50 | 0 | - | 46.4 | 0 | 0 | - | - | - | - | - | |
| RFA | - | 0 | - | 20.8 | 0 | 0 | - | - | - | ||||
| 陈康2019[12] | 肝切除 | 17.1 | 1.3 | - | - | - | - | - | 88.8 | 68.8 | 51.1 | 0.258 | |
| RFA | 9.8 | 0 | - | - | - | - | 91.4 | 73.4 | 61.1 | ||||
| 黄新辉2013[13] | 肝切除 | 18.1 | 0 | - | 43.9 | 14.4 | 8.2 | 0.548 | 89.5 | 54.3 | 28.8 | 0.780 | |
| RFA | 0 | 0 | - | 56.9 | 12.4 | 5.0 | 82.6 | 50.8 | 20.5 | ||||
| 梁惠宏2011[14] | 肝切除 | 36 | 0 | ≤1年: 39>1年: 33 | - | - | - | - | 95.3 | 65.7 | 54.5 | >0.05 | |
| RFA | 13 | 0 | ≤1年: 37>1年: 42 | - | - | - | - | 100 | 79.4 | 62.1 | |||
| 任正刚2008[15] | 肝切除 | 5.5 | 0 | ≤2年: 71>2年: 74 | 79.4 | 48.1 | 34.4 | 0.001 | 88.1 | 62.6 | 41.0 | 0.693 | |
| RFA | 1.5 | 0 | ≤2年: 37>2年: 31 | 58.0 | 27.8 | 12.4 | 94.7 | 65.1 | 37.3 | ||||
| 田正灵2016[16] | 肝切除 | 6.7 | 0 | 10(33.3) | 73.3 | 64.3 | - | 0.002 | 96.7 | 93.3 | - | 0.54 | |
| RFA | 3.7 | 0 | 24(88.9) | 46.7 | 26.7 | - | 96.3 | 84.0 | - | ||||
| 张辉2013[17] | 肝切除 | 15.9 | 1.45 | - | - | - | - | - | 68.2 | 45.4 | - | >0.05 | |
| RFA | 0 | 0 | - | - | - | - | 73.7 | 53.6 | - | ||||
| 张婷婷2014[18] | 肝切除 | - | 0 | 22(56.4) | 66.7 | 50.7 | 43.4 | 0.323 | 96.2 | 76.9 | 61.2 | 0.471 | |
| RFA | - | 0 | 14(52.9) | 65.8 | 28.0 | 14.0 | 86.2 | 73.3 | 62.2 | ||||
| Peng 2018[19] | 肝切除 | 17.7 | 1.3 | - | 64.8 | 41.6 | 38.3 | 0.258 | 84.8 | 60.2 | 51.9 | 0.871 | |
| RFA | 4.7 | 0 | - | 58.2 | 35.2 | 29.6 | 84.6 | 66.9 | 49.1 | ||||
| Lu 2020[20] | 肝切除 | - | - | - | 91.8 | 82.0 | 72.9 | 0.38 | - | - | - | - | |
| RFA | - | - | - | 94.4 | 75.4 | 61.7 | - | - | - | ||||
| Xia 2019[21] | 肝切除 | 22.4 | 0 | 60.8 | 85.0 | 52.4 | 36.2 | 0.09 | 92.5 | 65.8 | 43.6 | 0.17 | |
| RFA | 7.3 | 0 | 64.2 | 74.2 | 41.7 | 30.2 | 87.5 | 52.5 | 38.5 | ||||
| 刘嘉龙2019[22] | 肝切除 | 35.9 | 0 | 19(48.7) | 69.2 | - | - | <0.001 | 92.3 | - | - | 0.292 | |
| RFA | 4.9 | 0 | 32(78.0) | 26.8 | - | - | 85.4 | - | - | ||||
| 注:-,未报道;1) P值来源于原文报道。 | |||||||||||||
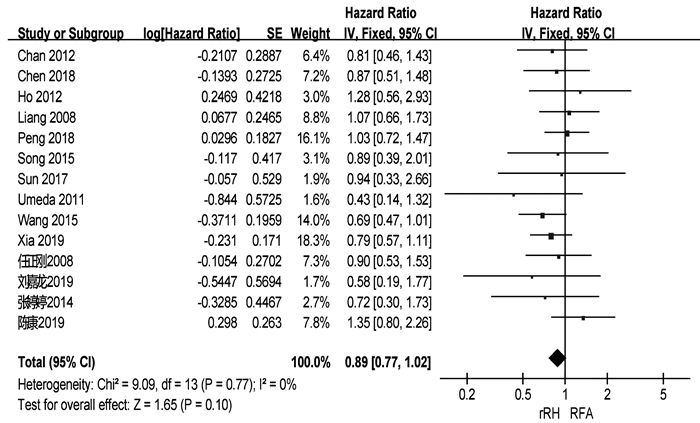
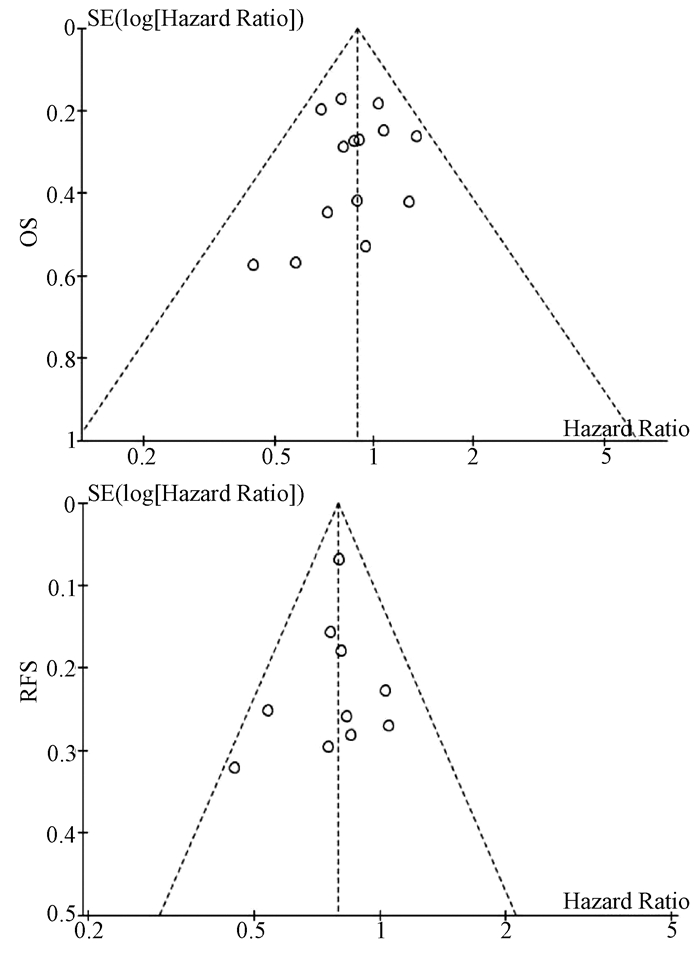
共有18篇研究[3-10, 12-18, 21-22]报道了OS(表 2)。两组患者术后1、3、5年中位OS分别为92.3%、66.3%、51.1%与91.4%、69.2%、39.9%。共有14篇研究[3-10, 12, 15, 18-19, 21-22]可提取数据统计HR,各组间不存在异质性(I2=0,P=0.77),采用固定效应模型进行分析。结果显示,两组患者的OS差异无统计学意义(HR= 0.89,95%CI:0.77~1.02,P=0.10)(图 2)。
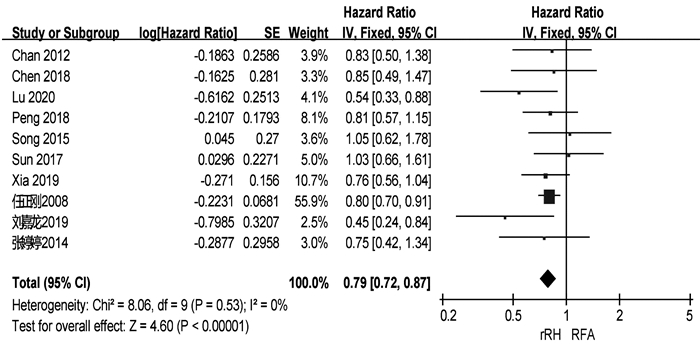
共有13篇研究[4, 6, 9-11, 13, 15-16, 18-19, 20-22]报道了RFS(表 2)。两组患者术后1、3、5年中位RFS分别为67.9%、48.3%、34.4%和57.5%、27.9%、14.0%。共有10篇研究[4, 6, 9-10, 15, 18-22]可提取数据统计HR,各组间不存在异质性(I2=0,P=0.53),采用固定效应模型进行分析。结果显示,再次肝切除术组患者的RFS显著高于RFA组(HR=0.79,95%CI:0.72~0.87,P<0.001)(图 3)。
基于OS和RFS HR的漏斗图提示,发表偏倚不明显(图 4)。
肝癌术后复发是影响患者术后长期生存的主要危险因素。对于复发性肝癌,目前临床上以多学科综合治疗为主。肝移植能显著提高复发性肝癌患者的RFS和远期生存率[23],但肝移植适应证严格、肝源匮乏和费用昂贵等问题仍限制其广泛的临床应用。此外,既往研究[24-25]表明再次肝切除术和RFA对复发性肝癌的疗效均优于介入。因此,针对肝内复发性肝癌患者,再次肝切除术和RFA是目前较为理想的治疗方案。有研究[3]认为再次肝切除术是治疗复发性肝癌的首选治疗方案,即使患者的原发癌更具侵袭性,肝功能水平更差,肝癌复发后行再次肝切除术仍可以获得与RFA相似的疗效。梁惠宏等[14]的研究则发现,RFA治疗复发性小肝癌的长期疗效优于再次肝切除术。因此,关于再次肝切除术和RFA治疗复发性肝癌的选择仍存在较大争议。本研究通过Meta分析的方法,综合评估再次肝切除术和RFA治疗复发性肝癌的疗效和安全性。
本研究结果显示,两组患者的OS无显著性差异,但再次肝切除术组患者的RFS显著高于RFA组。这一结论与肝切除术和RFA治疗原发性肝癌的结果一致[26-27]。RFA组患者RFS偏低的原因可能是:(1)再次肝切除术能将复发肿瘤以及潜在的瘤周子灶及血管癌栓同时切除,减少肿瘤再次局部复发和转移的可能性;(2)RFA后部分患者的肿瘤消融不完全而需进行二次消融或其他治疗;(3)术前影像学检查未能发现主瘤旁的微小卫星灶,导致消融不完全而引起肝癌再次复发。虽然RFA可用于治疗直径≤5 cm的肝癌,但目前认为其最佳适应证为直径≤3 cm的小肝癌[28]。有研究[29]发现,肝癌的直径和数目是导致RFA消融不完全的主要因素,随着肝癌直径的增加,RFA的疗效逐步下降。Livraghi等[30]的研究也表明RFA治疗直径3~5 cm的肝癌时完全消融率显著降低,导致RFA治疗复发性肝癌后局部复发和早期复发的比例明显升高。无论是原发性还是复发性肝癌,肿瘤直径在3~5 cm时经RFA治疗后其RFS和远期生存率均低于再次肝切除术[21, 31]。因此,在选择复发性肝癌治疗方案时,肿瘤直径应作为重要的参考指标。
本研究中,在围手术期并发症方面,再次肝切除术组和RFA组患者的中位发生率分别为22.4%和3.3%,与原发性肝癌接受肝切除术或RFA治疗后的并发症发生率相似[32-33]。此外,本研究还发现RFA治疗复发性肝癌的安全性明显优于再次肝切除术。RFA组患者术后并发症发生率及严重程度更低。虽然再次肝切除术能改善患者的远期生存率及RFS,但再次肝切除术的实施仍受诸多因素的限制,例如复发肿瘤的位置、数量以及肝硬化严重程度等。手术造成较大的创伤导致患者术后更容易发生严重并发症。此外,肝癌患者常伴有不同程度的肝硬化,无疑增加了手术的风险,部分患者最终死于肝衰竭而非肝癌本身带来的肿瘤负担[32]。相比于再次肝切除术,RFA在超声等影像学技术引导下精准地对复发肿瘤进行消融,从而最大限度地避免正常肝组织的破坏。对于手术无法切除、无法耐受手术的患者亦可选择RFA治疗。此外,RFA还可联合介入或无水酒精注射提高患者的OS和RFS[10, 19]。RFA本身具有微创和可重复的优点,肝癌再次复发后相当一部分患者仍可及时接受RFA或其他治疗[12],从而获得与再次肝切除相似的短期OS。
值得注意的是,本研究纳入文献中多数为回顾性研究,仅有2篇随机对照试验,因此本研究结论仍需更多的随机对照试验进行验证。其次,再次肝切除术和RFA治疗复发性肝癌的适应证存在一定的区别。然而,本Meta分析纳入的多数文献均仅纳入符合米兰标准的复发性肝癌,这些患者同时符合再次肝切除术和RFA的适应证。最后,肝癌术后复发(甚至多次)比较常见,对于复发肿瘤的治疗,多采取综合治疗方案(如介入、靶向、免疫治疗等),而非再次肝切除术或RFA等“单一”治疗模式。因此,联合治疗方案可能影响本荟萃分析对患者OS的判断。
总而言之,对于复发性肝癌的治疗,再次肝切除术能提高患者RFS,RFA则具有安全性高的优点。因此,在复发性肝癌患者的治疗中应遵循个体化和多学科治疗原则,合理选择治疗方案。
|
[1]CHEON YK,LEHMAN GA.Identification of risk factors for stone recurrence after endoscopic treatment of bile duct stones[J].Eur JGastroenterol Hepatol,2006,18(18):461-464.
|
|
[2]SCHONFELS W,BUCH S,WOLK M,et al.Recurrence of gallstones after cholecystectomy is associated with ABCG5/8 genotype[J].J Gastroenterol,2013,48(3):391-396.
|
|
[3]KEIZMAN D,ISH-SHALOM M,KONIKOFF FM.The clinical significance of bile duct sludge:is it different from bile duct stones?[J].Surg Endosc,2007,21(5):769-773.
|
|
[4]SEO DB,BANG BW,JEONG S,et al.Does the bile duct angulation affect recurrence of choledocholithiasis?[J].World J Gastroenterol,2011,17(36):4118-4123.
|
|
[5]LI X,ZHU KX,ZHANG L,et al.Periampullary diverticulum may be an important factor for the occurrence and recurrence of bile duct stones[J].World J Surg,2012,36(11):2666-2669.
|
|
[6]YAMAMOTO R,TAZUMA S,KANNO K,et al.Ursodeoxycholic acid after bile duct stone removal and risk factors for recurrence:a randomized trial[J].J Hepatobiliary Pancreat Sci,2016,23(2):132-136.
|
|
[7]TAO YT,MENG XL,XU AM,et al.Study on the role of the activities ofβ-glucuronidase in the two type of primary cholelithiasis in the common bile duct[J].J Hepatobiliary Surg,2012,20(2):122-126.(in Chinese)陶应田,孟翔凌,徐阿曼,等.β-葡萄糖醛酸酶与两类原发性胆总管结石形成关系的研究[J].肝胆外科杂志,2012,20(2):122-126.
|
|
[8]TAKAHASHI Y,YAMAMICHI N,SHIMAMOTO T,et al.Helicobacter pylori infection is positively associated with gallstones:a large-scale cross-sectional study in Japan[J].J Gastroenterol,2014,49(5):882-889.
|
|
[9]YANG LC,HUANG BY,XUE GF,et al.Relationship between infection of clonorchis sinensis and hepatobiliary and pancreatic diseases[J].Chin J Hepatobiliary Surg,2004,10(3):165-166.(in Chinese)杨六成,黄宝裕,薛桂芳,等.华支睾吸虫感染与肝胆胰外科疾病的关系[J].中华肝胆外科杂志,2004,10(3):165-166.
|
|
[10]LIU XF,GUO RX,TIAN YL,et al.The relationship between HBV infection and the formation of biliary sludge and its significance[J].Chin J Gen Surg,1999,14(5):329-331.(in Chinese)刘小方,郭仁宣,田雨霖,等.乙肝病毒感染与胆泥形成的关系及其意义[J].中华普通外科杂志,1999,14(5):329-331.
|
|
[11]SONG ME,CHUNG MJ,LEE DJ,et al.Cholecystectomy for prevention of recurrence after endoscopic clearance of bile duct stones in Korea[J].Yonsei Med J,2016,57(1):132-137.
|
|
[12]JAKOBS R,HARTMANN D,KUDIS V,et al.Risk factors for symptomatic stone recurrence after transpapillary laser lithotripsy for difficult bile duct stones using a laser with a stone recognition system[J].Eur J Gastroenterol Hepatol,2006,18(18):469-473.
|
|
[13]WU LY,WANG SH,JIA GF,et al.Risk factors for recurrent common bile duct stones after endoscopic sphincterotomy[J/CD].Chin J Digest Med Imageol:Electronic Edition,2015,5(1):5-9.(in Chinese)吴丽颖,王书海,贾国法,等.经十二指肠镜乳头括约肌切开取石术后胆总管结石复发危险因素分析[J/CD].中华消化病与影像杂志:电子版,2015,5(1):5-9.
|
|
[14]STRNAD P,FIGURA G,GRUSS R,et al.Oblique bile duct predisposes to the recurrence of bile duct stones[J].PLoS One,2013,8(1):e54601.
|
|
[15]KIM JH,KIM YS,KIM DK,et al.Short-term clinical outcomes based on risk factors of recurrence after removing common bile duct stones with endoscopic papillary large balloon dilatation[J].Clin Endosc,2011,44(2):123-128.
|
|
[16]HU B,TANG CB,SHI LH,et al.Study on relationship of cholelithiasis with Oddi sphincter peristalsis direction and physiological narrow distal segment length of choledochus[J].J North China Coal Medical College,2006,8(6):745-746.(in Chinese)胡兵,唐采白,石丽红,等.Oddi括约肌蠕动方向及胆总管远端生理狭窄段长度与胆石病成因的相关性研究[J].华北煤炭医学院学报,2006,8(6):745-746.
|
|
[17]PASPATIS GA,PARASKEVA K,VARDAS E,et al.Long-term recurrence of bile duct stones after endoscopic papillary large balloon dilation with sphincterotomy:4-year extended follow-up of a randomized trial[J].Surg Endosc,2016.[Epub ahead of print]
|
|
[18]MU HL,GAO JF,KONG QY,et al.Prognostic factors and postoperative recurrence of calculus following small-incision sphincterotomy with papillary balloon dilation for the treatment of intractable choledocholithiasis:a 72-month follow-up study[J].Dig Dis Sci,2015,60(7):2144-2149.
|
|
[19] ADMIRAND WH,SMALL DM.The physicochemical basis of cholesterol gallstone formation in man[J].J Clin Invest,1968,47(47):1043-1052.
|
|
[20]XIE M,KOTECHA VR,ANDRADE JD,et al.Augmented cholesterol absorption and sarcolemmal sterol enrichment slow small intestinal transit in mice,contributing to cholesterol cholelithogenesis[J].J Physiol,2012,590(8):1811-1824.
|
|
[21]YANG Y,QU Q,LIU W,et al.Increased bile cholesterol content inhibits gallbladder contraction by affecting the re-distribution of CCK-1R[J].Basic Clin Med,2014,34(7):984-989.(in Chinese)杨阳,曲强,刘卫,等.胆汁中胆固醇升高通过影响CCK-1R再分布抑制胆囊收缩[J].基础医学与临床,2014,34(7):984-989.
|
|
[22]WANG HH,PORTINCASA P,WANG DQ.Molecular pathophysiology and physical chemistry of cholesterol gallstones[J].Front Biosci,2008,13(2):401-423.
|
|
[23]LI L,LI B,DING HG.Effect of ursodeoxycholic acid on bile secretion after endoscopic nanobiliary drainage in patients with cholestatic liver disease of various causes[J].J Clin Hepatol,2016,32(3):522-525.(in Chinese)李磊,李冰,丁惠国.熊去氧胆酸对不同原因胆汁淤积性肝病患者鼻胆管引流术后胆汁排泌的影响[J].临床肝胆病杂志,2016,32(3):522-525.
|
|
[24]SUN Z,BO WH,JIANG P,et al.Different types of periampullary duodenal diverticula are associated with occurrence and recurrence of bile duct stones:a case-control study from a Chinese center[J].Gastroenterol Res Pract,2016,2016:9381759.
|
|
[25]KIM CW,CHANG JH,KIM JH,et al.Size and type of periampullary duodenal diverticula are associated with bile duct diameter and recurrence of bile duct stones[J].J Gastroenterol Hepatol,2013,28(5):893-898.
|
|
[26]LAU JY,LEOW CK,FUNG TM,et al.Cholecystectomy or gallbladder in situ after endoscopic sphincterotomy and bile duct stone removal in chinese patients[J].Gastroenterology,2006,130(1):96-103.
|
|
[27]LI JS,ZHANG GN,ZHONG Y.Clinical efficacy of laparoscope combined with choledochoscope in treatment of choledocholithiasis after cholesystectomy[J].Chin J Dig Surg,2015,14(2):155-156.(in Chinese)李建水,张光年,钟扬.腹腔镜联合胆道镜治疗胆囊切除术后胆总管结石的临床疗效[J].中华消化外科杂志,2015,14(2):155-156.
|
|
[28]CHEN Z,ZHANG HY,XU XB,et al.Recurrence after gallbladder-preserving cholecystolithotomy for sand-like and non-sandlike gallstones:a comparative analysis[J].J Clin Hepatol,2016,32(7):1351-1353.(in Chinese)陈智,张洪义,徐新保,等.胆囊泥沙样与非泥沙样结石保胆取石术后复发情况的比较[J].临床肝胆病杂志,2016,32(7):1351-1353.
|
|
[29]YOON H,KWON C,JEONG S,et al.Clinical significance of biliary dilatation and cholelithiasis after subtotal gastrectomy[J].Korean J Gastroenterol,2015,66(1):33-40.
|
|
[30]LIU YG.Study on risk factors for the recurrence of cholecystolithiasis after surger[J].Hainan Med J,2012,23(8):57-58.(in Chinese)刘永国.胆总管结石术后复发的相关因素分析[J].海南医学,2012,23(8):57-58.
|
|
[31]HARADA R,MAGUCHI H,TAKAHASHI K,et al.Large balloon dilation for the treatment of recurrent bile duct stones prevents short-term recurrence in patients with previous endoscopic sphincterotomy[J].J Hepatobiliary Pancreat Sci,2013,20(5):498-503.
|
|
[32]TAZUMA S.Epidemiology,pathogenesis,and classification of biliary stones(common bile duct and intrahepatic)[J].Best Pract Res Clin Gastroenterol,2006,20(6):1075-1083.
|
|
[33]TSAI TJ,LAI KH,LIN CK,et al.The relationship between gallbladder status and recurrent biliary complications in patients with choledocholithiasis following endoscopic treatment[J].J Chin Med Assoc,2012,75(11):560-566.
|
|
[34]ZHANG Z,TIAN J,LIAO Q,et al.The analysis of expression of CCK and IP3 receptors in gallstones patients with type 2 diabetes mellitus[J].Hepatogastroenterology,2014,61(136):2173-2176.
|
|
[35]KEIZMAN D,SHALOM MI,KONIKOFF FM.Recurrent symptomatic common bile duct stones after endoscopic stone extraction in elderly patients[J].Gastrointest Endosc,2006,64(1):60-65.
|
|
[36]FAN Y,WU SD,FU BB,et al.Decreased number of interstitial cells of Cajal play an important role in the declined intestinal transit during cholesterol gallstone formation in guinea pigs fed on high cholesterol diet[J].Int J Clin Exp Med,2014,7(5):1262-1268.
|
| 1. | 刘新,金子铮,刘宁,陈淑湘,刘辉,于艳华,娄金丽. 乙肝核心相关抗原联合AFP、PIVKA-Ⅱ对乙肝相关肝癌的诊断价值研究. 北京医学. 2023(10): 852-857 .  | |
| 2. | 周莉,陈辰,翟璐,程晓静,韩旭,姚升娟,高敏,李嘉. 血清AFP、PIVKA-Ⅱ、miR-21检测对肝细胞癌的诊断意义. 实用器官移植电子杂志. 2022(02): 135-139 . | |
| 3. | 董磊. 血清FER、AFP-L3联合检测诊断肝细胞癌的价值分析. 检验医学与临床. 2020(11): 1561-1563+1567 . | |
| 4. | 李惠军,李彩东,田鹏飞,段正军,雷志萍,张旭强. 乙肝病毒相关肝癌行AFP、PIVKA-Ⅱ和AFU联合检测的价值研究. 中国卫生标准管理. 2020(13): 108-110 . | |
| 5. | 张莉. 血清铁蛋白、甲胎蛋白异质体3联合腓骨蛋白-1检测诊断肝细胞癌的价值分析. 医学理论与实践. 2020(14): 2247-2249+2240 . | |
| 6. | 王傲然,李晓玲,门秋爽,孙凤霞. 血清铁蛋白与肝脏疾病研究进展. 中国肝脏病杂志(电子版). 2020(04): 34-37 . | |
| 7. | 许羚雁. GALAD模型在原发性肝细胞癌诊断和预后评估中的价值研究. 循证医学. 2020(05): 277-281 . | |
| 8. | 高光剑,潘耀振. PIVKA-Ⅱ及AFP对原发性肝癌的诊断价值. 贵州医科大学学报. 2019(01): 100-104 . | |
| 9. | 董秋月. 慢性乙型肝炎患者32例的肿瘤标志物检测的临床意义. 世界最新医学信息文摘. 2019(53): 13-14 . | |
| 10. | 孔令希,覃山子,秦雪,陈志坚. PIVKA-Ⅱ、AFP、RDW联合检测在肝细胞癌中的诊断价值. 广西医科大学学报. 2018(06): 839-841 . | |
| 11. | 张莹,颜学兵. 血清异常凝血酶原Ⅱ对HBV相关肝细胞癌的诊断价值. 临床肝胆病杂志. 2018(07): 1470-1474 .  本站查看 本站查看 | |
| 12. | 王欢,陆惠慧,尚琴,徐令清. PIVKA-Ⅱ在乙型肝炎病毒感染者中筛查HCC的应用价值分析. 中国医学创新. 2018(12): 62-65 . | |
| 13. | 赵芬,郭庆波,曲凯,梁欢. 联合检测PIVKAⅡ、AFP、Ferrtin对肝细胞癌的诊断价值. 国际检验医学杂志. 2018(21): 2615-2617+2621 . |

The first journal specializing in hepatobiliary and pancreatic diseases in China
Supervisor:Ministry of Education of the People's Republic of China
Sponsor:Jilin University
Academic Support: Chinese Society of Hepatology,Chinese Medical Association
Address: 461 Xinjiang Road, Changchun
Submit:0431-88782044
Peer review:0431-88783542
Email:lcgdb@vip.163.com
Website Design © 2020 Editorial Board of Journal of Clinical Hepatology
吉ICP备10000617号-1
Supported by: Beijing Renhe Information Technology Co. Ltd

LI MJ, DENG ZJ, LIU HT, et al. Clinical effect of re-hepatic resection versus radiofrequency ablation in treatment of recurrent hepatocellular carcinoma in Asia: A Meta-analysis [J]. J Clin Hepatol, 2021, 37(5): 1103-1109. DOI: 10.3969/j.issn.1001-5256.2021.05.025.

| 第一作者和年份 | 国家/地区 | 纳入时间(年) | 组别 | 样本量 | 男/女(例) | 年龄(岁) | 单个/多个肿瘤(例) | 复发肿瘤直径(cm) | 肝硬化[例(%)] | CTP分级(A/B/C,例) | 随访(月) |
| Wang 2015[3] | 中国 | 2004—2010 | 肝切除 | 128 | 113/15 | 50.2±10.1 | 89/39 | 2.4±0.9 | 66(51.6) | - | - |
| RFA | 162 | 148/14 | 52.7±10.9 | 107/55 | 2.3±0.7 | - | - | - | |||
| Sun 2017[4] | 中国台湾 | 2002—2014 | 肝切除 | 43 | 34/9 | 60(35~76) | - | 1.9(0.8~3.0) | 36(83.7) | 42/1 | 53 |
| RFA | 57 | 38/19 | 63(27~81) | - | 1.8(1.0~3.0) | 50(87.7) | 57/0 | 54 | |||
| Umeda 2011[5] | 日本 | 1998—2007 | 肝切除 | 29 | - | - | - | 3.20±0.57 | - | 29/0 | 48 |
| RFA | 58 | - | - | - | 2.1±0.3 | - | 51/7 | 48 | |||
| Song 2015[6] | 韩国 | 1994—2012 | 肝切除 | 39 | 31/8 | 52.5±9.8 | 32/7 | 2.2±1.1 | 23(59) | 39/0 | 36.3(0.8~126.6) |
| RFA | 178 | 145/33 | 55.4±10.6 | 156/22 | 1.7±0.6 | 130(73.0) | 172/6 | 44.7(5.6~139.8) | |||
| Liang 2008[7] | 中国 | 1999—2007 | 肝切除 | 44 | 39/5 | 48.8±12.0 | 34/10 | ≤3 (26) | - | 44/0 | 33.5±24.1 |
| RFA | 66 | 54/12 | 54.6±10.8 | 48/18 | ≤3 (44) | - | 64/2 | 21.1±19.1 | |||
| Ho 2012[8] | 中国台湾 | 2001—2007 | 肝切除 | 54 | 40/14 | 56.3±12.3 | - | 2.9±1.8 | 26(48.1) | 51/2/1 | 32(0~79) |
| RFA | 50 | 39/11 | 61.0±11.1 | - | 2.3±1.9 | 28(56.0) | 50/0 | 27(0~96) | |||
| Chan 2012[9] | 中国香港 | 2001—2008 | 肝切除 | 29 | - | 52(38~79) | 21/8 | 2.1(0.8~5.5) | 25(86.2) | 29/0 | 44.9 |
| RFA | 45 | - | 59(36~80) | 29/16 | 2.2(0.8~6.0) | 40(88.9) | 40/5 | 44.9 | |||
| Chen 2018[10] | 中国 | 2009—2015 | 肝切除 | 48 | 41/7 | 73.5±3.5 | 28/20 | 2.6±1.1 | 41(85.4) | 39/9 | 36.9(2~78) |
| RFA | 57 | 51/6 | 73.7±2.9 | 30/27 | 2.5±1.2 | 49(86.0) | 45/12 | 37.3(2~78) | |||
| 岑峰2016[11] | 中国 | 2011—2015 | 肝切除 | 28 | 22/6 | 53.6 | 12/16 | - | 23(82.1) | 18/10 | - |
| RFA | 24 | 19/5 | 55.7 | 10/14 | - | 19(79.2) | - | - | |||
| 陈康2019[12] | 中国 | 2005—2014 | 肝切除 | 77 | 65/12 | - | - | - | 57(74) | 76/1 | 57(2~168) |
| RFA | 82 | 72/10 | - | - | - | 50(61) | 77/5 | 51(4~111) | |||
| 黄新辉2013[13] | 中国 | 2007—2011 | 肝切除 | 66 | 51/15 | 50.5±10.1 | 66/0 | 2.9±1.1 | 57(86.3) | 66/0 | - |
| RFA | 46 | 36/10 | 54.1±12.1 | 46/0 | 2.6±0.9 | 39(84.8) | 46/0 | - | |||
| 梁惠宏2011[14] | 中国 | 1999—2009 | 肝切除 | 72 | 65/7 | 49±12 | 72/0 | 2.1±0.1 | - | 70/2 | 36±25 |
| RFA | 79 | 69/10 | 55±11 | 79/0 | 2.5±0.1 | - | 73/6 | 32±21 | |||
| 任正刚2008[15] | 中国 | 2000—2005 | 肝切除 | 145 | 127/18 | 51 | 127/18 | 2.0 | - | 145/0 | 23(3~88) |
| RFA | 68 | 64/4 | 52 | 52/16 | 2.0 | - | 68/0 | 23(3~88) | |||
| 田正灵2016[16] | 中国 | 2012—2015 | 肝切除 | 30 | 28/2 | 48.8±9.6 | 24/6 | - | 24(80) | - | 17(6.0~42.5) |
| RFA | 27 | 26/1 | 50.9±10.1 | 19/8 | - | 23(85.2) | - | 17(6.0~42.5) | |||
| 张辉2013[17] | 中国 | 2003—2011 | 肝切除 | 69 | - | - | - | 3.5 | 61(88.4) | 54/15 | - |
| RFA | 99 | - | - | 2.1 | 76(76.8) | 71/28 | - | ||||
| 张婷婷2014[18] | 中国 | 1998—2010 | 肝切除 | 27 | 25/2 | 47±13 | 25/2 | 3.2±1.1 | - | 27/0 | 32(9~118) |
| RFA | 39 | 37/2 | 52±13 | 37/2 | 2.7±1.1 | - | 37/2 | 28(2~79) | |||
| Peng 2018[19] | 中国 | 2006—2015 | 肝切除 | 79 | 67/2 | 55 | 59/20 | ≤3(48) | - | - | 53.2(4~96) |
| RFA | 107 | 95/12 | 57 | 75/32 | ≤3(73) | - | - | 52.3(3~96) | |||
| Lu 2020[20] | 中国 | 2004—2015 | 肝切除 | 138 | 124/16 | 50.1±10.9 | 112/26 | 2.8±1.9 | 96(70) | 138/0 | 37.6 |
| RFA | 194 | 172/22 | 52.9±11.8 | 162/32 | 1.9±0.9 | 134(69) | 194/0 | 41.6 | |||
| Xia 2019[21] | 中国 | 2010—2013 | 肝切除 | 120 | 107/13 | 52.4(25.7~60.5) | 96/24 | 2.9(1.0~5.0) | 50(41.7) | 120/0 | 44.3(4.3~90.6) |
| RFA | 120 | 109/11 | 53.5(28.0~59.9) | 94/26 | 2.7(1.0~4.8) | 55(45.8) | 120/0 | 44.3(4.3~90.6) | |||
| 刘嘉龙2019[22] | 中国 | 2016—2017 | 肝切除 | 39 | 38/1 | 50.0±10.0 | 37/2 | 2.1±0.7 | 37(94.9) | 38/1 | 24 |
| RFA | 41 | 37/4 | 48.9±11.3 | 39/2 | 1.8±0.8 | 39(95.1) | 39/2 | 24 | |||
| 注:-,未报道。 | |||||||||||
| 第一作者和年份 | 组别 | 并发症发生率(%) | 围手术期病死率(%) | 复发[例(%)] | RFS | OS | |||||||
| 1年 | 3年 | 5年 | P值1) | 1年 | 3年 | 5年 | P值1) | ||||||
| Wang 2015[3] | 肝切除 | - | - | - | - | - | - | - | 97.7 | 84.1 | 64.5 | <0.001 | |
| RFA | - | - | - | - | - | - | 96.9 | 73.4 | 37.0 | ||||
| Sun 2017[4] | 肝切除 | 16 | 2 | 30(69.8) | 57.0 | 32.1 | 28.6 | 0.89 | 97.6 | 82.7 | 56.4 | 0.69 | |
| RFA | 7 | 0 | 41(71.9) | 60.8 | 26.6 | 16.6 | 98.2 | 77.2 | 52.6 | ||||
| Umeda 2011[5] | 肝切除 | - | - | - | - | - | - | - | 93.1 | 66.8 | 58.1 | 0.899 | |
| RFA | - | - | - | - | - | - | 94.7 | 75.1 | 48.3 | ||||
| Song 2015[6] | 肝切除 | 64 | 2.6 | 18(46.2) | 66.1 | 48.5 | 43.1 | 0.834 | 88.8 | 88.8 | 83.9 | 0.686 | |
| RFA | 2.2 | 0 | 117(65.7) | 70.1 | 40.8 | 30.0 | 98.9 | 82.5 | 71.0 | ||||
| Liang 2008[7] | 肝切除 | 68.2 | 0 | 86.4 | - | - | - | - | 78.6 | 44.5 | 27.6 | 0.79 | |
| RFA | 3.0 | 0 | 78.8 | - | - | - | 76.6 | 48.6 | 39.9 | ||||
| Ho 2012[8] | 肝切除 | - | - | - | - | - | - | - | - | - | 72.0 | - | |
| RFA | - | - | - | - | - | - | - | - | 83.0 | ||||
| Chan 2012[9] | 肝切除 | 24.1 | 0 | 21(72.4) | 41.1 | 24.2 | 24.2 | 0.14 | 89.7 | 56.5 | 35.2 | 0.51 | |
| RFA | 2.2 | 2.2 | 38(84.4) | 32.2 | 12.4 | 9.3 | 83.7 | 43.1 | 29.1 | ||||
| Chen 2018[10] | 肝切除 | 25 | 2.1 | 26(54.2) | 73.1 | 49.7 | 40.7 | 0.465 | 76.3 | 52.5 | 42.6 | 0.413 | |
| RFA | 0 | 0 | 27(47.4) | 69.5 | 37.8 | 33.1 | 78.2 | 40.8 | 36.7 | ||||
| 岑峰2016[11] | 肝切除 | 50 | 0 | - | 46.4 | 0 | 0 | - | - | - | - | - | |
| RFA | - | 0 | - | 20.8 | 0 | 0 | - | - | - | ||||
| 陈康2019[12] | 肝切除 | 17.1 | 1.3 | - | - | - | - | - | 88.8 | 68.8 | 51.1 | 0.258 | |
| RFA | 9.8 | 0 | - | - | - | - | 91.4 | 73.4 | 61.1 | ||||
| 黄新辉2013[13] | 肝切除 | 18.1 | 0 | - | 43.9 | 14.4 | 8.2 | 0.548 | 89.5 | 54.3 | 28.8 | 0.780 | |
| RFA | 0 | 0 | - | 56.9 | 12.4 | 5.0 | 82.6 | 50.8 | 20.5 | ||||
| 梁惠宏2011[14] | 肝切除 | 36 | 0 | ≤1年: 39>1年: 33 | - | - | - | - | 95.3 | 65.7 | 54.5 | >0.05 | |
| RFA | 13 | 0 | ≤1年: 37>1年: 42 | - | - | - | - | 100 | 79.4 | 62.1 | |||
| 任正刚2008[15] | 肝切除 | 5.5 | 0 | ≤2年: 71>2年: 74 | 79.4 | 48.1 | 34.4 | 0.001 | 88.1 | 62.6 | 41.0 | 0.693 | |
| RFA | 1.5 | 0 | ≤2年: 37>2年: 31 | 58.0 | 27.8 | 12.4 | 94.7 | 65.1 | 37.3 | ||||
| 田正灵2016[16] | 肝切除 | 6.7 | 0 | 10(33.3) | 73.3 | 64.3 | - | 0.002 | 96.7 | 93.3 | - | 0.54 | |
| RFA | 3.7 | 0 | 24(88.9) | 46.7 | 26.7 | - | 96.3 | 84.0 | - | ||||
| 张辉2013[17] | 肝切除 | 15.9 | 1.45 | - | - | - | - | - | 68.2 | 45.4 | - | >0.05 | |
| RFA | 0 | 0 | - | - | - | - | 73.7 | 53.6 | - | ||||
| 张婷婷2014[18] | 肝切除 | - | 0 | 22(56.4) | 66.7 | 50.7 | 43.4 | 0.323 | 96.2 | 76.9 | 61.2 | 0.471 | |
| RFA | - | 0 | 14(52.9) | 65.8 | 28.0 | 14.0 | 86.2 | 73.3 | 62.2 | ||||
| Peng 2018[19] | 肝切除 | 17.7 | 1.3 | - | 64.8 | 41.6 | 38.3 | 0.258 | 84.8 | 60.2 | 51.9 | 0.871 | |
| RFA | 4.7 | 0 | - | 58.2 | 35.2 | 29.6 | 84.6 | 66.9 | 49.1 | ||||
| Lu 2020[20] | 肝切除 | - | - | - | 91.8 | 82.0 | 72.9 | 0.38 | - | - | - | - | |
| RFA | - | - | - | 94.4 | 75.4 | 61.7 | - | - | - | ||||
| Xia 2019[21] | 肝切除 | 22.4 | 0 | 60.8 | 85.0 | 52.4 | 36.2 | 0.09 | 92.5 | 65.8 | 43.6 | 0.17 | |
| RFA | 7.3 | 0 | 64.2 | 74.2 | 41.7 | 30.2 | 87.5 | 52.5 | 38.5 | ||||
| 刘嘉龙2019[22] | 肝切除 | 35.9 | 0 | 19(48.7) | 69.2 | - | - | <0.001 | 92.3 | - | - | 0.292 | |
| RFA | 4.9 | 0 | 32(78.0) | 26.8 | - | - | 85.4 | - | - | ||||
| 注:-,未报道;1) P值来源于原文报道。 | |||||||||||||
| 第一作者和年份 | 国家/地区 | 纳入时间(年) | 组别 | 样本量 | 男/女(例) | 年龄(岁) | 单个/多个肿瘤(例) | 复发肿瘤直径(cm) | 肝硬化[例(%)] | CTP分级(A/B/C,例) | 随访(月) |
| Wang 2015[3] | 中国 | 2004—2010 | 肝切除 | 128 | 113/15 | 50.2±10.1 | 89/39 | 2.4±0.9 | 66(51.6) | - | - |
| RFA | 162 | 148/14 | 52.7±10.9 | 107/55 | 2.3±0.7 | - | - | - | |||
| Sun 2017[4] | 中国台湾 | 2002—2014 | 肝切除 | 43 | 34/9 | 60(35~76) | - | 1.9(0.8~3.0) | 36(83.7) | 42/1 | 53 |
| RFA | 57 | 38/19 | 63(27~81) | - | 1.8(1.0~3.0) | 50(87.7) | 57/0 | 54 | |||
| Umeda 2011[5] | 日本 | 1998—2007 | 肝切除 | 29 | - | - | - | 3.20±0.57 | - | 29/0 | 48 |
| RFA | 58 | - | - | - | 2.1±0.3 | - | 51/7 | 48 | |||
| Song 2015[6] | 韩国 | 1994—2012 | 肝切除 | 39 | 31/8 | 52.5±9.8 | 32/7 | 2.2±1.1 | 23(59) | 39/0 | 36.3(0.8~126.6) |
| RFA | 178 | 145/33 | 55.4±10.6 | 156/22 | 1.7±0.6 | 130(73.0) | 172/6 | 44.7(5.6~139.8) | |||
| Liang 2008[7] | 中国 | 1999—2007 | 肝切除 | 44 | 39/5 | 48.8±12.0 | 34/10 | ≤3 (26) | - | 44/0 | 33.5±24.1 |
| RFA | 66 | 54/12 | 54.6±10.8 | 48/18 | ≤3 (44) | - | 64/2 | 21.1±19.1 | |||
| Ho 2012[8] | 中国台湾 | 2001—2007 | 肝切除 | 54 | 40/14 | 56.3±12.3 | - | 2.9±1.8 | 26(48.1) | 51/2/1 | 32(0~79) |
| RFA | 50 | 39/11 | 61.0±11.1 | - | 2.3±1.9 | 28(56.0) | 50/0 | 27(0~96) | |||
| Chan 2012[9] | 中国香港 | 2001—2008 | 肝切除 | 29 | - | 52(38~79) | 21/8 | 2.1(0.8~5.5) | 25(86.2) | 29/0 | 44.9 |
| RFA | 45 | - | 59(36~80) | 29/16 | 2.2(0.8~6.0) | 40(88.9) | 40/5 | 44.9 | |||
| Chen 2018[10] | 中国 | 2009—2015 | 肝切除 | 48 | 41/7 | 73.5±3.5 | 28/20 | 2.6±1.1 | 41(85.4) | 39/9 | 36.9(2~78) |
| RFA | 57 | 51/6 | 73.7±2.9 | 30/27 | 2.5±1.2 | 49(86.0) | 45/12 | 37.3(2~78) | |||
| 岑峰2016[11] | 中国 | 2011—2015 | 肝切除 | 28 | 22/6 | 53.6 | 12/16 | - | 23(82.1) | 18/10 | - |
| RFA | 24 | 19/5 | 55.7 | 10/14 | - | 19(79.2) | - | - | |||
| 陈康2019[12] | 中国 | 2005—2014 | 肝切除 | 77 | 65/12 | - | - | - | 57(74) | 76/1 | 57(2~168) |
| RFA | 82 | 72/10 | - | - | - | 50(61) | 77/5 | 51(4~111) | |||
| 黄新辉2013[13] | 中国 | 2007—2011 | 肝切除 | 66 | 51/15 | 50.5±10.1 | 66/0 | 2.9±1.1 | 57(86.3) | 66/0 | - |
| RFA | 46 | 36/10 | 54.1±12.1 | 46/0 | 2.6±0.9 | 39(84.8) | 46/0 | - | |||
| 梁惠宏2011[14] | 中国 | 1999—2009 | 肝切除 | 72 | 65/7 | 49±12 | 72/0 | 2.1±0.1 | - | 70/2 | 36±25 |
| RFA | 79 | 69/10 | 55±11 | 79/0 | 2.5±0.1 | - | 73/6 | 32±21 | |||
| 任正刚2008[15] | 中国 | 2000—2005 | 肝切除 | 145 | 127/18 | 51 | 127/18 | 2.0 | - | 145/0 | 23(3~88) |
| RFA | 68 | 64/4 | 52 | 52/16 | 2.0 | - | 68/0 | 23(3~88) | |||
| 田正灵2016[16] | 中国 | 2012—2015 | 肝切除 | 30 | 28/2 | 48.8±9.6 | 24/6 | - | 24(80) | - | 17(6.0~42.5) |
| RFA | 27 | 26/1 | 50.9±10.1 | 19/8 | - | 23(85.2) | - | 17(6.0~42.5) | |||
| 张辉2013[17] | 中国 | 2003—2011 | 肝切除 | 69 | - | - | - | 3.5 | 61(88.4) | 54/15 | - |
| RFA | 99 | - | - | 2.1 | 76(76.8) | 71/28 | - | ||||
| 张婷婷2014[18] | 中国 | 1998—2010 | 肝切除 | 27 | 25/2 | 47±13 | 25/2 | 3.2±1.1 | - | 27/0 | 32(9~118) |
| RFA | 39 | 37/2 | 52±13 | 37/2 | 2.7±1.1 | - | 37/2 | 28(2~79) | |||
| Peng 2018[19] | 中国 | 2006—2015 | 肝切除 | 79 | 67/2 | 55 | 59/20 | ≤3(48) | - | - | 53.2(4~96) |
| RFA | 107 | 95/12 | 57 | 75/32 | ≤3(73) | - | - | 52.3(3~96) | |||
| Lu 2020[20] | 中国 | 2004—2015 | 肝切除 | 138 | 124/16 | 50.1±10.9 | 112/26 | 2.8±1.9 | 96(70) | 138/0 | 37.6 |
| RFA | 194 | 172/22 | 52.9±11.8 | 162/32 | 1.9±0.9 | 134(69) | 194/0 | 41.6 | |||
| Xia 2019[21] | 中国 | 2010—2013 | 肝切除 | 120 | 107/13 | 52.4(25.7~60.5) | 96/24 | 2.9(1.0~5.0) | 50(41.7) | 120/0 | 44.3(4.3~90.6) |
| RFA | 120 | 109/11 | 53.5(28.0~59.9) | 94/26 | 2.7(1.0~4.8) | 55(45.8) | 120/0 | 44.3(4.3~90.6) | |||
| 刘嘉龙2019[22] | 中国 | 2016—2017 | 肝切除 | 39 | 38/1 | 50.0±10.0 | 37/2 | 2.1±0.7 | 37(94.9) | 38/1 | 24 |
| RFA | 41 | 37/4 | 48.9±11.3 | 39/2 | 1.8±0.8 | 39(95.1) | 39/2 | 24 | |||
| 注:-,未报道。 | |||||||||||
| 第一作者和年份 | 组别 | 并发症发生率(%) | 围手术期病死率(%) | 复发[例(%)] | RFS | OS | |||||||
| 1年 | 3年 | 5年 | P值1) | 1年 | 3年 | 5年 | P值1) | ||||||
| Wang 2015[3] | 肝切除 | - | - | - | - | - | - | - | 97.7 | 84.1 | 64.5 | <0.001 | |
| RFA | - | - | - | - | - | - | 96.9 | 73.4 | 37.0 | ||||
| Sun 2017[4] | 肝切除 | 16 | 2 | 30(69.8) | 57.0 | 32.1 | 28.6 | 0.89 | 97.6 | 82.7 | 56.4 | 0.69 | |
| RFA | 7 | 0 | 41(71.9) | 60.8 | 26.6 | 16.6 | 98.2 | 77.2 | 52.6 | ||||
| Umeda 2011[5] | 肝切除 | - | - | - | - | - | - | - | 93.1 | 66.8 | 58.1 | 0.899 | |
| RFA | - | - | - | - | - | - | 94.7 | 75.1 | 48.3 | ||||
| Song 2015[6] | 肝切除 | 64 | 2.6 | 18(46.2) | 66.1 | 48.5 | 43.1 | 0.834 | 88.8 | 88.8 | 83.9 | 0.686 | |
| RFA | 2.2 | 0 | 117(65.7) | 70.1 | 40.8 | 30.0 | 98.9 | 82.5 | 71.0 | ||||
| Liang 2008[7] | 肝切除 | 68.2 | 0 | 86.4 | - | - | - | - | 78.6 | 44.5 | 27.6 | 0.79 | |
| RFA | 3.0 | 0 | 78.8 | - | - | - | 76.6 | 48.6 | 39.9 | ||||
| Ho 2012[8] | 肝切除 | - | - | - | - | - | - | - | - | - | 72.0 | - | |
| RFA | - | - | - | - | - | - | - | - | 83.0 | ||||
| Chan 2012[9] | 肝切除 | 24.1 | 0 | 21(72.4) | 41.1 | 24.2 | 24.2 | 0.14 | 89.7 | 56.5 | 35.2 | 0.51 | |
| RFA | 2.2 | 2.2 | 38(84.4) | 32.2 | 12.4 | 9.3 | 83.7 | 43.1 | 29.1 | ||||
| Chen 2018[10] | 肝切除 | 25 | 2.1 | 26(54.2) | 73.1 | 49.7 | 40.7 | 0.465 | 76.3 | 52.5 | 42.6 | 0.413 | |
| RFA | 0 | 0 | 27(47.4) | 69.5 | 37.8 | 33.1 | 78.2 | 40.8 | 36.7 | ||||
| 岑峰2016[11] | 肝切除 | 50 | 0 | - | 46.4 | 0 | 0 | - | - | - | - | - | |
| RFA | - | 0 | - | 20.8 | 0 | 0 | - | - | - | ||||
| 陈康2019[12] | 肝切除 | 17.1 | 1.3 | - | - | - | - | - | 88.8 | 68.8 | 51.1 | 0.258 | |
| RFA | 9.8 | 0 | - | - | - | - | 91.4 | 73.4 | 61.1 | ||||
| 黄新辉2013[13] | 肝切除 | 18.1 | 0 | - | 43.9 | 14.4 | 8.2 | 0.548 | 89.5 | 54.3 | 28.8 | 0.780 | |
| RFA | 0 | 0 | - | 56.9 | 12.4 | 5.0 | 82.6 | 50.8 | 20.5 | ||||
| 梁惠宏2011[14] | 肝切除 | 36 | 0 | ≤1年: 39>1年: 33 | - | - | - | - | 95.3 | 65.7 | 54.5 | >0.05 | |
| RFA | 13 | 0 | ≤1年: 37>1年: 42 | - | - | - | - | 100 | 79.4 | 62.1 | |||
| 任正刚2008[15] | 肝切除 | 5.5 | 0 | ≤2年: 71>2年: 74 | 79.4 | 48.1 | 34.4 | 0.001 | 88.1 | 62.6 | 41.0 | 0.693 | |
| RFA | 1.5 | 0 | ≤2年: 37>2年: 31 | 58.0 | 27.8 | 12.4 | 94.7 | 65.1 | 37.3 | ||||
| 田正灵2016[16] | 肝切除 | 6.7 | 0 | 10(33.3) | 73.3 | 64.3 | - | 0.002 | 96.7 | 93.3 | - | 0.54 | |
| RFA | 3.7 | 0 | 24(88.9) | 46.7 | 26.7 | - | 96.3 | 84.0 | - | ||||
| 张辉2013[17] | 肝切除 | 15.9 | 1.45 | - | - | - | - | - | 68.2 | 45.4 | - | >0.05 | |
| RFA | 0 | 0 | - | - | - | - | 73.7 | 53.6 | - | ||||
| 张婷婷2014[18] | 肝切除 | - | 0 | 22(56.4) | 66.7 | 50.7 | 43.4 | 0.323 | 96.2 | 76.9 | 61.2 | 0.471 | |
| RFA | - | 0 | 14(52.9) | 65.8 | 28.0 | 14.0 | 86.2 | 73.3 | 62.2 | ||||
| Peng 2018[19] | 肝切除 | 17.7 | 1.3 | - | 64.8 | 41.6 | 38.3 | 0.258 | 84.8 | 60.2 | 51.9 | 0.871 | |
| RFA | 4.7 | 0 | - | 58.2 | 35.2 | 29.6 | 84.6 | 66.9 | 49.1 | ||||
| Lu 2020[20] | 肝切除 | - | - | - | 91.8 | 82.0 | 72.9 | 0.38 | - | - | - | - | |
| RFA | - | - | - | 94.4 | 75.4 | 61.7 | - | - | - | ||||
| Xia 2019[21] | 肝切除 | 22.4 | 0 | 60.8 | 85.0 | 52.4 | 36.2 | 0.09 | 92.5 | 65.8 | 43.6 | 0.17 | |
| RFA | 7.3 | 0 | 64.2 | 74.2 | 41.7 | 30.2 | 87.5 | 52.5 | 38.5 | ||||
| 刘嘉龙2019[22] | 肝切除 | 35.9 | 0 | 19(48.7) | 69.2 | - | - | <0.001 | 92.3 | - | - | 0.292 | |
| RFA | 4.9 | 0 | 32(78.0) | 26.8 | - | - | 85.4 | - | - | ||||
| 注:-,未报道;1) P值来源于原文报道。 | |||||||||||||
 下载:
下载:


 DownLoad:
DownLoad: