Objective To investigate the expression of proteasome subunit beta type 4( PSMB4) in hepatocellular carcinoma( HCC) tissue and normal liver tissue and its significance in clinical prognosis. Methods Eight fresh HCC tissue specimens were collected from the patients who underwent surgical treatment in Affiliated Hospital of Nantong University from January to October,2017,and Western Blot was used to measure the protein expression of PSMB4 in HCC tissue and the corresponding adjacent tissue. A total of 105 paraffin-embedded HCC tissue specimens and 25 paraffin-embedded normal liver tissue specimens,which were preserved in Affiliated Hospital of Nantong University from January 2009 and October 2012,were collected,and immunohistochemistry was used to measure the expression of PSMB4.According to the expression of PSMB4,105 HCC patients were divided into high PSMB4 expression group with 57 patients and low PSMB4 expression group with 48 patients. The independent samples t-test was used for comparison of continuous data between groups,and the chi-square test was used for comparison of categorical data between groups. The Cox proportional-hazards regression model and the Kaplan-Meier survival curves were used to analyze the clinicopathological features and prognosis of the patients in the two groups. Results There were significant differences between the two groups in hepatitis B virus infection,maximum tumor diameter,degree of tumor differentiation,and TNM stage( χ2= 22. 482,8. 219,14. 964,and 6. 587,all P < 0. 05). Among the 105 HCC patients,57( 54. 29%) had high PSMB4 expression and 48( 45. 71%) had low PSMB4 expression,while among the 25 normal liver tissue specimens,8( 32%) had high PSMB4 expression and 17( 68%) had low PSMB4 expression or no PSMB4 expression,and there was a significant difference in PSMB4 expression between the two groups( χ2= 4. 011,P < 0. 05). PSMB4 staining was mainly distributed in the cytoplasm and nucleus,with an appearance of brown or brownish yellow particles. Among the 8 fresh HCC tissue specimens,7 specimens had significantly higher protein expression of PSMB4 than the corresponding adjacent tissue specimens( all P < 0. 05). The patients' 5-year survival was associated with tumor size( P = 0. 01),metastasis( P < 0. 001),degree of tumor differentiation( P = 0. 01),TNM stage( P = 0,003),and PSMB4 expression( P <0. 001),among which metastasis( hazard ratio [HR]= 11. 375,95% confidence interval[CI]: 4. 911-26. 348,P < 0. 001) and high PSMB4 expression( HR = 6. 834,95% CI: 2. 939-15. 889,P < 0. 001) were independent risk factors in HCC patients. The high PSMB4 expression group had a significantly lower 5-year survival rate than the low PSMB4 expression group( 27. 6% vs 79. 2%,χ2= 22. 96,P <0. 05). Conclusion There is an increase in the expression of PSMB4 in HCC tissue,and high expression of PSMB4 is an independent risk factor for poor prognosis in HCC patients,suggesting that PSMB4 may serve as a potential prognostic marker or a potential target for treatment.
Figure
2.
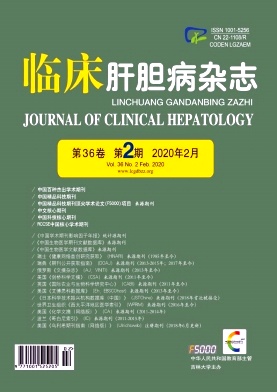
The inhibitory effects of different concentrations of Carrimycin on the proliferation of MIA PaCa-2 and BxPC-3 cells were detected by EdU and colony formation assay
Figure
3.
Cell cycle and Western Blot experiments were performed to examine the effects of different concentrations of Carrimycin on the cell cycle of MIA PaCa-2 and BxPC-3 cells
[1] BRAY F,FERLAY J,SOERJOMATARAM I,et al. Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin,2018,68(6):394-424.
[2] TORRE LA,BRAY F,SIEGEL RL,et al. Global cancer statistics,2012[J]. CA Cancer J Clin,2015,65(2):87-108.
[3] HULIN A,STOCCO J,BOUATTOUR M. Clinical pharmacokinetics and pharmacodynamics of transarterial chemoembolization and targeted therapies in hepatocellular carcinoma[J].Clin Pharmacokinet,2019,58(8):983-1014.
[4] CHEN WY. REN N. Advances in molecular targeted therapy for hepatocellular carcinoma[J]. J Clin Hepatol,2018,34(7):1387-1394.(in Chinese)陈万勇,任宁.肝细胞癌分子靶向治疗进展[J].临床肝胆病杂志,2018,34(7):1387-1394.
[5] GUO N,PENG Z. MG132,a proteasome inhibitor,induces apoptosis in tumor cells[J]. Asia Pac J Clin Oncol,2013,9(1):6-11.
[6] CHENG YC,TSAI WC,SUNG YC,et al. Interference with PSMB4 expression exerts an anti-tumor effect by decreasing the invasion and proliferation of human glioblastoma cells[J].Cell Physiol Biochem,2018,45(2):819-831.
[7] ZHU ZX,HUANG JW,LIAO MH,et al. Treatment strategy for hepatocellular carcinoma in China:Radiofrequency ablation versus liver resection[J]. Jpn J Clin Oncol,2016,46(12):1075-1080.
[8] National Health and Family Planning Commission of the People’s Republic of China. Diagnosis,management,and treatment of hepatocellular carcinoma(V2017)[J]. J Clin Hepatol,2017,33(8):1419-1431.(in Chinese)中华人民共和国国家卫生和计划生育委员会.原发性肝癌诊疗规范(2017年版)[J].临床肝胆病杂志,2017,33(8):1419-1431.
[9] KIM DW,TALATI C,KIM R. Hepatocellular carcinoma(HCC):Beyond sorafenib-chemotherapy[J]. J Gastrointest Oncol,2017,8(2):256-265.
[10] ZHU DQ,CHEN XJ. Effects of plumbagin on proliferation and apoptosis of hepatocellular carcinoma HepG2R cells resistant to sorafenib and its mechanism[J]. J Jilin Univ(Med Edit),2018,44(6):1223-1229.(in Chinese)朱德强,陈学军.白花丹素对肝癌索拉菲尼耐药细胞HepG2R增殖和凋亡的影响及其机制[J].吉林大学学报(医学版),2018,44(6):1223-1229.
[11] JANG HH. Regulation of protein degradation by proteasomes in cancer[J]. J Cancer Prev,2018,23(4):153-161.
[12] LEE GY,HAVERTY PM,LI L,et al. Comparative oncogenomics identifies PSMB4 and SHMT2 as potential cancer driver genes[J]. Cancer Res,2014,74(11):3114-3126.
[13] EANG R,GIRBAL-NEUHAUSER E,XU B,et al. Characterization and differential expression of a newly identified phosphorylated isoform of the human 20S proteasome beta7 subunit in tumor vs. normal cell lines[J]. Fundam Clin Pharmacol,2009,23(2):215-224.
[14] LEE KM,LEE J,PARK CS. Cereblon inhibits proteasome activity by binding to the 20S core proteasome subunit beta type4[J]. Biochem Biophys Res Commun,2012,427(3):618-622.
[15] LIU R,LU S,DENG Y,et al. PSMB4 expression associates with epithelial ovarian cancer growth and poor prognosis[J].Arch Gynecol Obstet,2016,293(6):1297-1307.
[16] ZHANG Y,LIU H,CUI M,et al. Effect of the HBV whole-X gene on the expression of hepatocellular carcinoma associated proteins[J]. J Microbiol Immunol Infect,2016,49(3):335-343.
[17] CUI F,WANG Y,WANG J,et al. The up-regulation of proteasome subunits and lysosomal proteases in hepatocellular carcinomas of the HBx gene knockin transgenic mice[J]. Proteomics,2006,6(2):498-504.
BAI LN, LIU Y, TANG CX, et al. Mechanism of carrimycin in regulating the biological function of pancreatic cancer cells[J]. J Clin Hepatol, 2022, 38(12): 2793-2801. DOI: 10.3969/j.issn.1001-5256.2022.12.020.
BAI LN, LIU Y, TANG CX, et al. Mechanism of carrimycin in regulating the biological function of pancreatic cancer cells[J]. J Clin Hepatol, 2022, 38(12): 2793-2801. DOI: 10.3969/j.issn.1001-5256.2022.12.020.
 下载:
下载:









 DownLoad:
DownLoad: