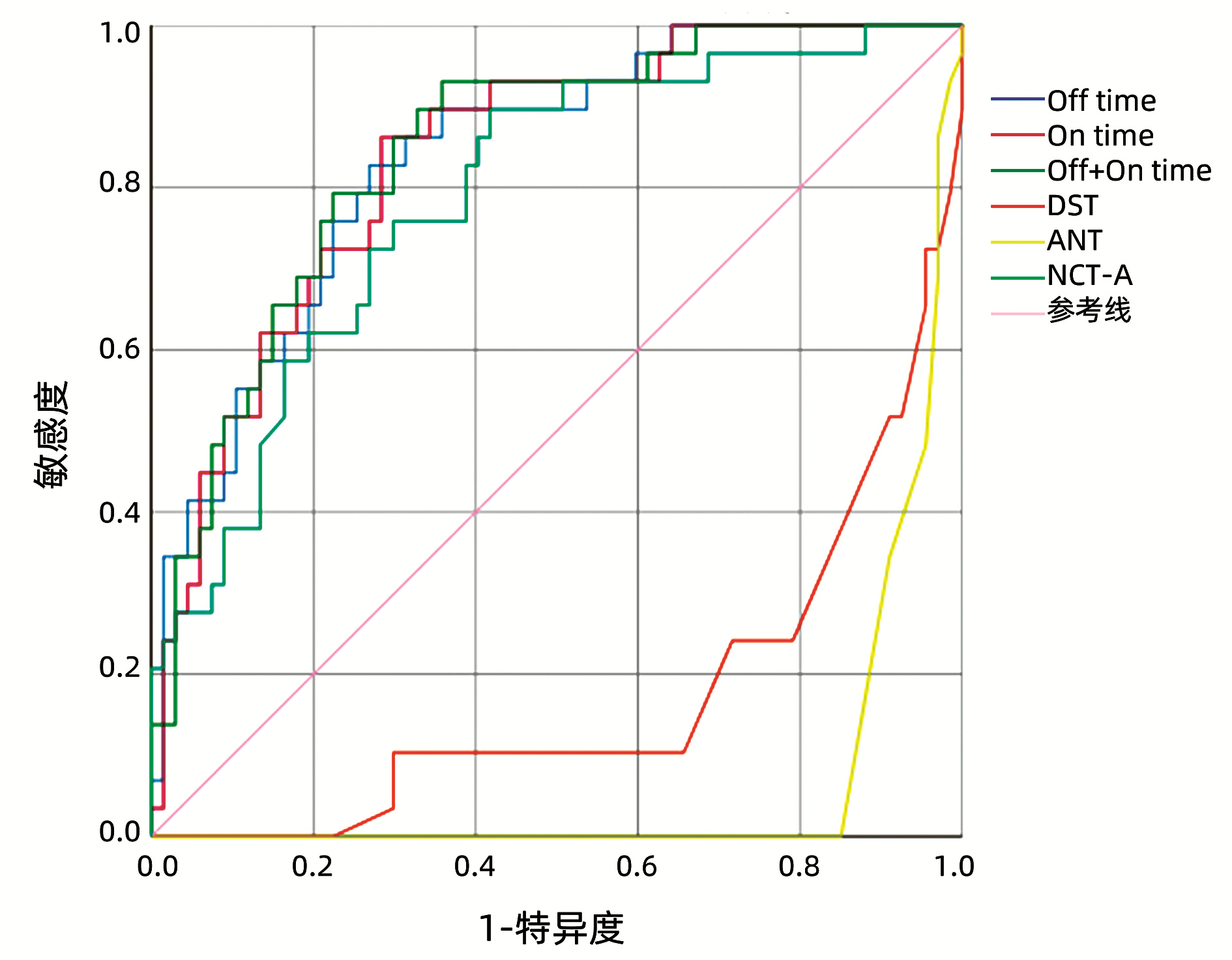
Objective To investigate the value of Stroop test, a neuropsychological test, in the diagnosis of minimal hepatic encephalopathy (MHE).Methods A total of 96 patients with liver cirrhosis who were hospitalized in Department of Infectious Diseases, The First Affiliated Hospital of Bengbu Medical College, from August 2020 to March 2021 were enrolled, and the number connection test-A (NCT-A), digit symbol test (DST), animal naming test (ANT), and Stroop test were performed for all patients. Test results were recorded and related clinical data were collected. The t-test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between groups. The receiver operating characteristic (ROC) curve was used to investigate the value of Stroop test in the diagnosis of MHE, and the Pearson correlation coefficient was used to analyze the correlation of the results of Stroop test with those of NCT-A, DST, and ANT.Results For the 96 patients with liver cirrhosis, the prevalence rate of MHE was 30.21% (29/96). The Off+On time of Stroop test had a cut-off value of 212.49 s in the diagnosis of MHE, with an area under the ROC curve of 0.845, a sensitivity of 93.10%, and a specificity of 64.20%. The Pearson correlation analysis showed that the On+Off time and On time of Stroop test were moderately correlated with NCT-A(r=0.580 and 0.590, both P < 0.01), the Off time of Stroop test was strongly correlated with NCT-A(r=0.620, P < 0.01), and the On+Off time, On time, and Off time of Stroop test were strongly correlated with DST(r=-0.650, -0.650, and -0.630, all P < 0.01).Conclusion In the diagnosis of MHE, Stroop test is a highly sensitive method with easy-to-read results and a high diagnostic value and does not require professional equipment.
Chinese Society of Hepatology, Chinese Medical Association. Guidelines on the management of hepatic encephalopathy in cirrhosis[J]. J Clin Hepatol, 2018, 34(10): 2076-2089. DOI: 10.3969/j.issn.1001-5256.2018.10.007.
Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35(11): 2408-2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.
WANG YL, SHAO LC, YANG Z. Diagnostic value of number connection test for minimal hepatic encephalopathy and related factors of cirrhosis complicated with hepatic encephalopathy[J]. Clin J Med Offic, 2020, 48(12): 1424-1426, 1429. DOI: 10.16680/j.1671-3826.2020.12.11.
CAMPAGNA F, MONTAGNESE S, RIDOLA L, et al. The animal naming test: An easy tool for the assessment of hepatic encephalopathy[J]. Hepatology, 2017, 66(1): 198-208. DOI: 10.1002/hep.29146.
[6]
BAJAJ JS, THACKER LR, HEUMAN DM, et al. The Stroop smartphone application is a short and valid method to screen for minimal hepatic encephalopathy[J]. Hepatology, 2013, 58(3): 1122-1132. DOI: 10.1002/hep.26309.
[7]
LABENZ C, BARON JS, TOENGES G, et al. Prospective evaluation of the impact of covert hepatic encephalopathy on quality of life and sleep in cirrhotic patients[J]. Aliment Pharmacol Ther, 2018, 48(3): 313-321. DOI: 10.1111/apt.14824.
[8]
SAN MARTÍN-VALENZUELA C, BORRAS-BARRACHINA A, GALLEGO JJ, et al. Motor and cognitive performance in patients with liver cirrhosis with minimal hepatic encephalopathy[J]. J Clin Med, 2020, 9(7): 2154. DOI: 10.3390/jcm9072154.
[9]
LABENZ C, ADARKWAH CC, WÖRNS MA, et al. Management of hepatic encephalopathy in Germany: A survey among physicians[J]. Z Gastroenterol, 2020, 58(1): 49-56. DOI: 10.1055/a-1010-6974.
[10]
WANG JY, ZHANG NP, CHI BR, et al. Prevalence of minimal hepatic encephalopathy and quality of life evaluations in hospitalized cirrhotic patients in China[J]. World J Gastroenterol, 2013, 19(30): 4984-4991. DOI: 10.3748/wjg.v19.i30.4984.
[11]
GIMÉNEZ-GARZÓ C, GARCÉS JJ, URIOS A, et al. The PHES battery does not detect all cirrhotic patients with early neurological deficits, which are different in different patients[J]. PLoS One, 2017, 12(2): e0171211. DOI: 10.1371/journal.pone.0171211.
[12]
BAJAJ JS, DUARTE-ROJO A, XIE JJ, et al. Minimal hepatic encephalopathy and mild cognitive impairment worsen quality of life in elderly patients with cirrhosis[J]. Clin Gastroenterol Hepatol, 2020, 18(13): 3008-3016. e2. DOI: 10.1016/j.cgh.2020.03.033.
[13]
ZENG X, ZHANG LY, LIU Q, et al. Combined scores from the encephalapp stroop test, number connection test B, and serial dotting test accurately identify patients with covert hepatic encephalopathy[J]. Clin Gastroenterol Hepatol, 2020, 18(7): 1618-1625. e7. DOI: 10.1016/j.cgh.2019.11.018.
[14]
LABENZ C, BEUL L, TOENGES G, et al. Validation of the simplified Animal Naming Test as primary screening tool for the diagnosis of covert hepatic encephalopathy[J]. Eur J Intern Med, 2019, 60: 96-100. DOI: 10.1016/j.ejim.2018.08.008.
[15]
QU Y, LI T, LIN C, et al. Animal naming test for the assessment of minimal hepatic encephalopathy in Asian cirrhotic populations[J]. Clin Res Hepatol Gastroenterol, 2021, 45(5): 101729. DOI: 10.1016/j.clinre.2021.101729.
QIAN FF, DAI MQ, ZHAO L, et al. Association between serum alkaline phosphatase and type 2 diabetes mellitus with nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2023, 39(1): 83-88. DOI: 10.3969/j.issn.1001-5256.2023.01.013.
QIAN FF, DAI MQ, ZHAO L, et al. Association between serum alkaline phosphatase and type 2 diabetes mellitus with nonalcoholic fatty liver disease[J]. J Clin Hepatol, 2023, 39(1): 83-88. DOI: 10.3969/j.issn.1001-5256.2023.01.013.

 下载:
下载:






 DownLoad:
DownLoad: