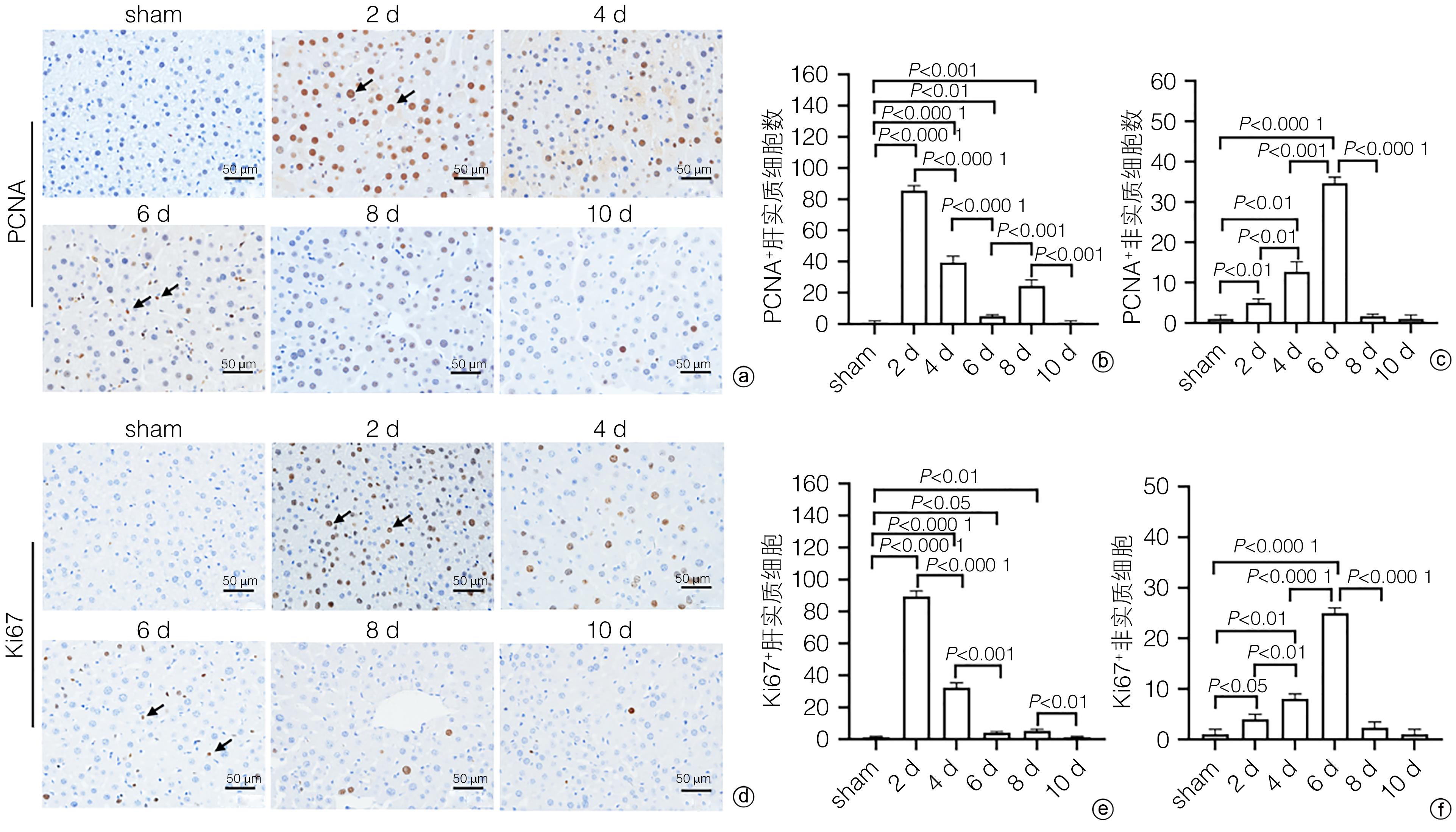
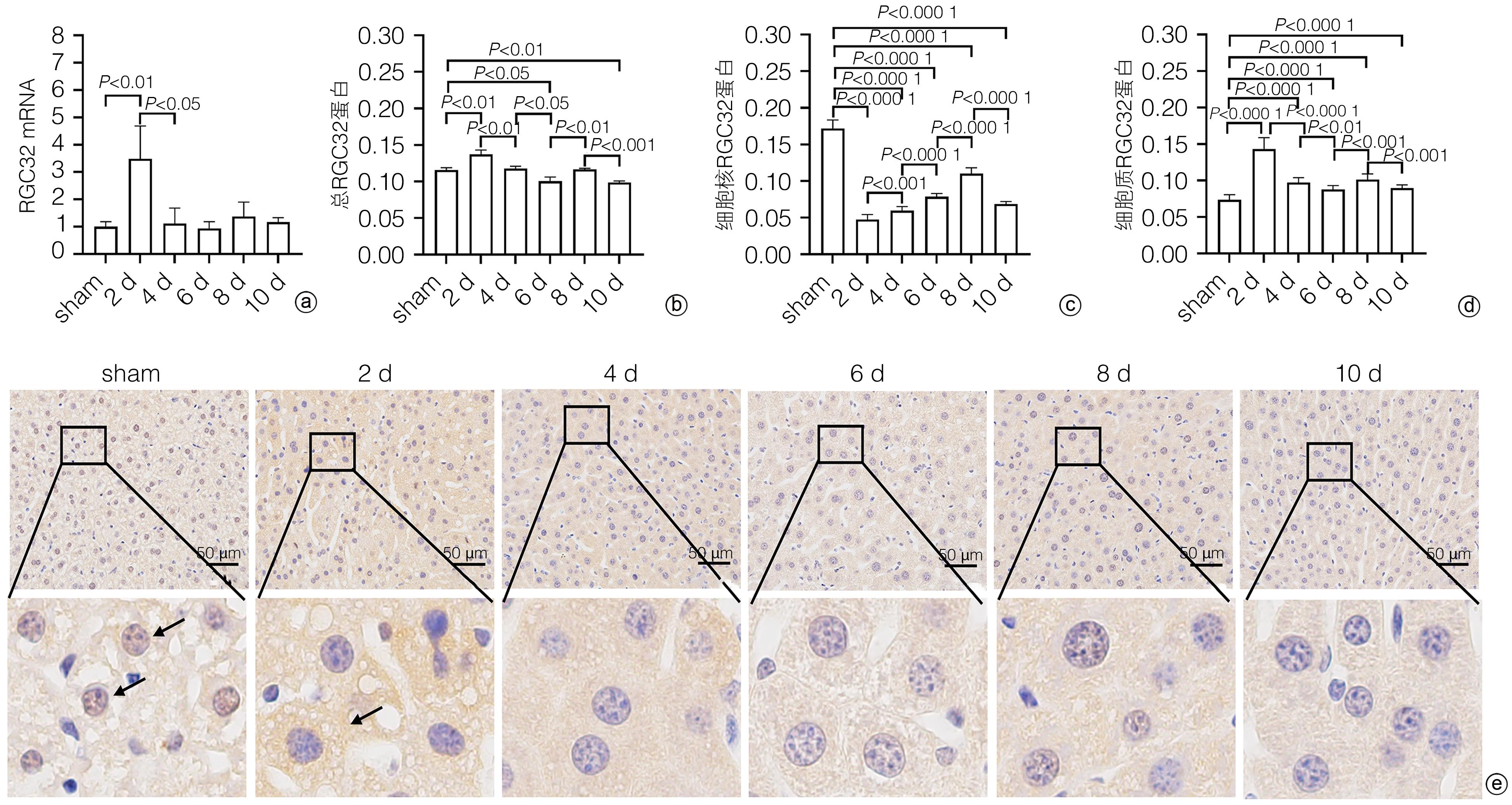
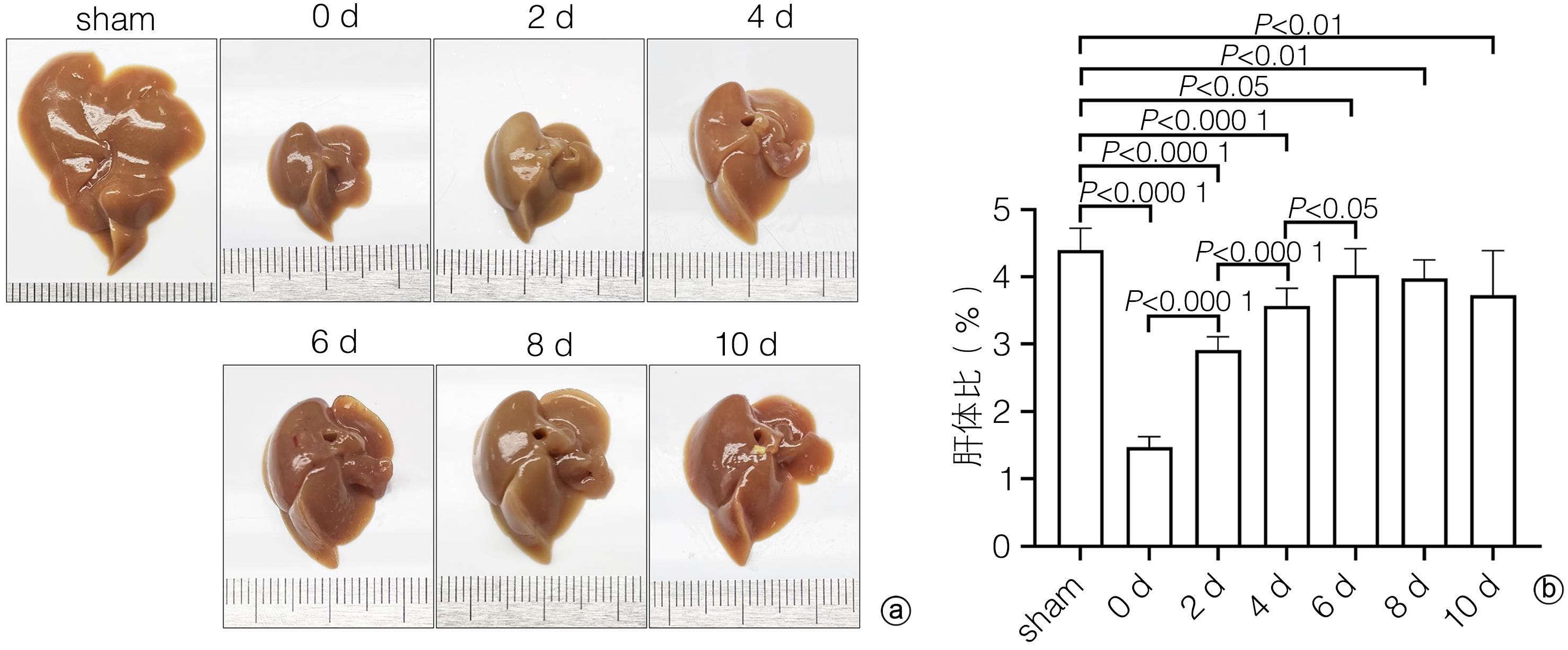
Objective To investigate the expression and role of response gene to complement 32 (RGC32) in liver regeneration after partial hepatectomy (PH).Methods A total of 42 male C57BL/6 mice, aged 10 weeks, were randomly divided into control group, postoperative day 1 group (1-d group), postoperative day 2 group (2-d group), postoperative day 4 group (4-d group), postoperative day 6 group (6-d group), postoperative day 8 group (8-d group), and postoperative day 10 group (10-d group), with 6 mice in each group. In the control group, the complete liver of the mice was resected for weighing and photography as the normal control group (sham group); further, the left and middle lobes of the liver were resected for weighing and photography as the surgical control group (0-day group); the sham group and the 0-day group shared the same group of mice. After successful modeling by PH, the mice were sacrificed on days 1, 2, 4, 6, 8, and 10 after surgery, and the liver was collected to measure the change in size. HE staining and oil red O staining were used to evaluate liver histomorphological changes; serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were measured to evaluate the changes in liver function; immunohistochemical staining was used to measure the expression of proliferating cell nuclear antigen (PCNA) and Ki67 and analyze the change in cell proliferation during liver regeneration; quantitatie real-time PCR and immunohistochemical staining were uused to measure the expression and subcellular distribution of RGC32 during liver regeneration; EdU cell proliferation assay was used to analyze the effect of RGC32 overexpression or knocknout on hepatocyte proliferation in L02 cells. For continuous data, comparison between multiple groups was made by analysis of variance, and further pairwise comparisons were conducted using the LSD-t test. The independent samples t-test was used for comparison of continuous data between two groups. A Pearson correlation analysis was performed.Results The liver gradually enlarged after PH, and the liver/body weight ratio rose to the peak from days 0 to 6, with significant differences between different time points (all P<0.05), while there was no significant change in liver size from days 6 to 10. The number of liver lipid droplets significantly increased after PH surgery and gradually decreased with liver regeneration, with a significant difference between the portal vein region and the central vein region (all P<0.05). Compared with the sham group, the 1d group had significant increases in the serum levels of ALT and AST (all P<0.05), which gradually returned to the levels of the sham group on day 6 and day 2 after surgery, respectively (P>0.05). Immunohistochemical staining showed that there were rapid increases in the numbers of PCNA- and Ki67-positive liver parenchymal cells after PH surgery, with the highest numbers of 86±5 and 89±5, respectively, on day 2, which then gradually decreased; however, there were gradual increases in the numbers of PCNA- and Ki67-positive nonparenchymal cells, with the peak numbers of 34±5 and 25±3, respectively, on day 6, which then gradually decreased. The total expression of RGC32 increased to the highest level on day 2 after PH surgery and then gradually decreased, and the changing trend of RGC32 expression in cytoplasm was consistent with that of total RGC32 expression; however, the expression of RGC32 in nucleus decreased to the lowest level on day 2 after PH surgery and then increased gradually. The correlation analysis showed that the expression of RGC32 in nucleus was negatively correlated with the proliferation of liver parenchymal cells (R2=0.308 3, P=0.016 7), and the expression of RGC32 in cytoplasm was positively correlated with the proliferation of liver parenchymal cells (R2=0.808 6, P<0.000 1). Cell experiments showed that compared with the control group, the EdU-positive rate was reduced by 15.6% after RGC32 overexpression (P<0.01) and was increased by 19.2% after RGC32 knockdown (P<0.01).Conclusion Liver parenchymal cells and nonparenchymal cells show asynchronous proliferation and participate in liver regeneration together. During liver regeneration after hepatectomy, there are differences in the expression of RGC32 between nucleus and cytoplasm, and RGC32 in nucleus may inhibit hepatocyte proliferation.
MICHALOPOULOS GK, BHUSHAN B. Liver regeneration: biological and pathological mechanisms and implications[J]. Nat Rev Gastroenterol Hepatol, 2021, 18( 1): 40- 55. DOI: 10.1038/s41575-020-0342-4.
[2]
LIN S, NASCIMENTO EM, GAJERA CR, et al. Distributed hepatocytes expressing telomerase repopulate the liver in homeostasis and injury[J]. Nature, 2018, 556( 7700): 244- 248. DOI: 10.1038/s41586-018-0004-7.
[3]
CHEN HX, HUANG SJ, CHEN JY, et al. Role of complement in liver injury and regeneration[J]. Central South Pharm, 2021, 19( 10): 2123- 2127. DOI: 10.7539/j.issn.1672-2981.2021.10.023.
WANG Q, QU X. New insights into the roles of RGC32[J]. Cell Mol Immunol, 2018, 15( 8): 803- 804. DOI: 10.1038/cmi.2017.154.
[5]
LI JX, LI MY. Research progress in animal models of regeneration[J]. Med Recapitulate, 2021, 27( 23): 4629- 4633. DOI: 10.3969/j.issn.1006-2084.2021.23.011.
NEVZOROVA YA, TOLBA R, TRAUTWEIN C, et al. Partial hepatectomy in mice[J]. Lab Anim, 2015, 49( Suppl 1): 81- 88. DOI: 10.1177/0023677215572000.
[7]
LÓPEZ-LUQUE J, FABREGAT I. Revisiting the liver: from development to regeneration-what we ought to know![J]. Int J Dev Biol, 2018, 62( 6- 7- 8): 441- 451. DOI: 10.1387/ijdb.170264JL.
[8]
van HAELE M, SNOECK J, ROSKAMS T. Human liver regeneration: an etiology dependent process[J]. Int J Mol Sci, 2019, 20( 9): 2332. DOI: 10.3390/ijms20092332.
[9]
YAGI S, HIRATA M, MIYACHI Y, et al. Liver regeneration after hepatectomy and partial liver transplantation[J]. Int J Mol Sci, 2020, 21( 21): 8414. DOI: 10.3390/ijms21218414.
[10]
YU ZY, LIN X, HAN Y, et al. Role of liver sinusoidal endothelial cells in liver regeneration and the development of liver fibrosis[J]. J Clin Hepatol, 2019, 35( 9): 2072- 2074. DOI: 10.3969/j.issn.1001-5256.2019.09.041.
LI N, LIU C, MA G, et al. Asparaginyl endopeptidase may promote liver sinusoidal endothelial cell angiogenesis via PI3K/Akt pathway[J]. Rev Esp Enferm Dig, 2019, 111( 3): 214- 222. DOI: 10.17235/reed.2018.5709/2018.
[12]
VLAICU SI, TATOMIR A, ANSELMO F, et al. RGC32 and diseases: the first 20 years[J]. Immunol Res, 2019, 67( 2- 3): 267- 279. DOI: 10.1007/s12026-019-09080-0.
VLAICU SI, TATOMIR A, BOODHOO D, et al. RGC32 is expressed in the human atherosclerotic arterial wall: Role in C5b-9-induced cell proliferation and migration[J]. Exp Mol Pathol, 2016, 101( 2): 221- 230. DOI: 10.1016/j.yexmp.2016.09.004.
[15]
CUI XB, GUO X, CHEN SY. Response gene to complement 32 deficiency causes impaired placental angiogenesis in mice[J]. Cardiovasc Res, 2013, 99( 4): 632- 639. DOI: 10.1093/cvr/cvt121.
[16]
CUI XB, LUAN JN, DONG K, et al. RGC32(response gene to complement 32) deficiency protects endothelial cells from inflammation and attenuates atherosclerosis[J]. Arterioscler Thromb Vasc Biol, 2018, 38( 4): e36-e47. DOI: 10.1161/ATVBAHA.117.310656.
[17]
HU C, WU Z, LI L. Mesenchymal stromal cells promote liver regeneration through regulation of immune cells[J]. Int J Biol Sci, 2020, 16( 5): 893- 903. DOI: 10.7150/ijbs.39725.
[18]
ZHENG J, LI JT, JIN J, et al. Characteristics of incision bacterial infection and changes of immune cytokines in patients with hepatocellular carcinoma after hepatectomy[J]. Chin J Microecol, 2022, 34( 7): 819- 823, 845. DOI: 10.13381/j.cnki.cjm.202207014.
SAIGUSA K, IMOTO I, TANIKAWA C, et al. RGC32, a novel p53-inducible gene, is located on centrosomes during mitosis and results in G2/M arrest[J]. Oncogene, 2007, 26( 8): 1110- 1121. DOI: 10.1038/sj.onc.1210148.
 下载:
下载:

 本站查看
本站查看




 DownLoad:
DownLoad: