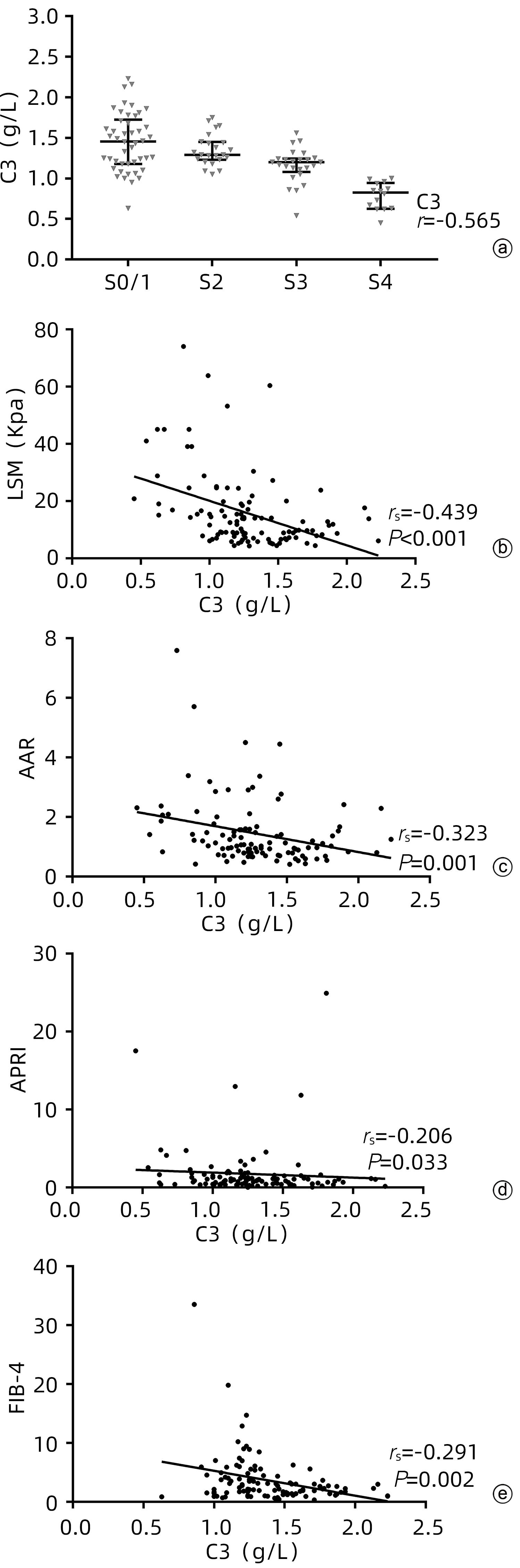
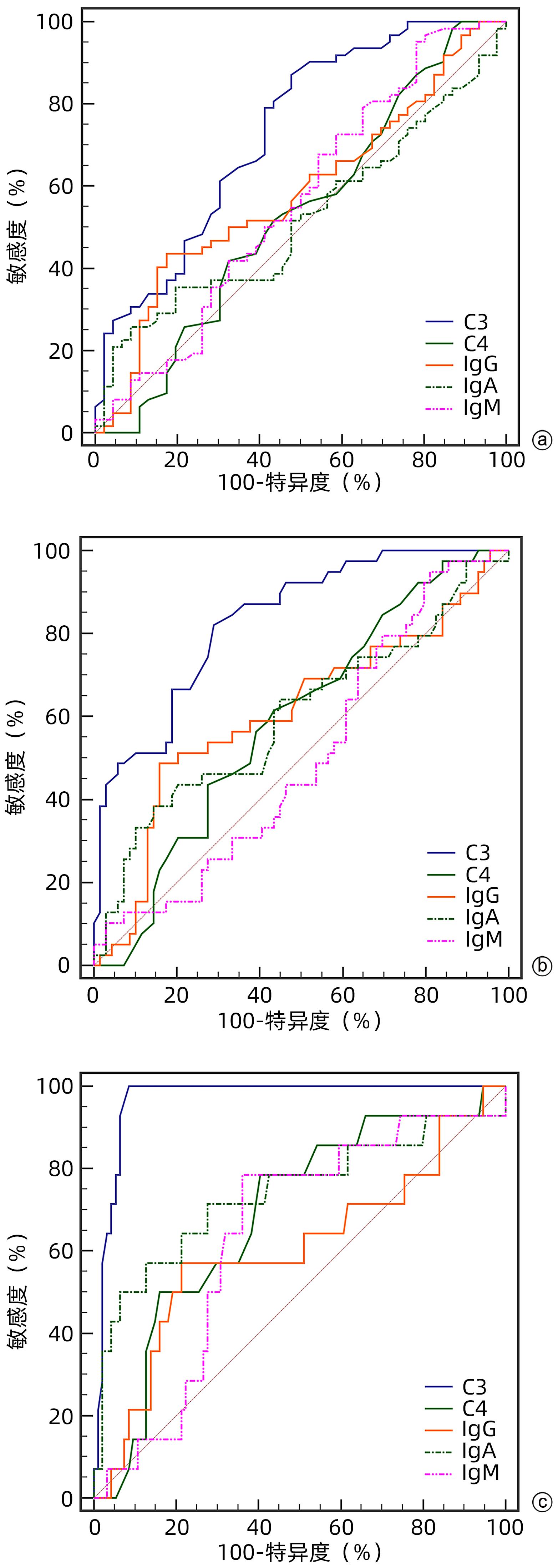
Objective To investigate the value of serum complement C3 level in determining the stage of liver fibrosis in primary biliary cholangitis (PBC).Methods Clinical data were collected from 108 patients with PBC who attended Tianjin Second People’s Hospital and underwent liver biopsy from January 2012 to October 2022. The degree of liver fibrosis (S0-4) was assessed according to the Scheuer scoring system, with ≥S2 defined as significant liver fibrosis, ≥S3 defined as progressive liver fibrosis, and S4 defined as liver cirrhosis. The independent samples t-test was used for comparison of normally distributed continuous data between two groups, and a one-way analysis of variance was used for comparison between multiple groups; the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups, and the Kruskal-Wallis H test was used for comparison between multiple groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The area under the ROC curve (AUC) was used to evaluate the efficacy of complement C3 in the diagnosis of liver fibrosis in patients with PBC. The Spearman correlation analysis was used to investigate the correlation between complement C3 and liver fibrosis stage.Results Among the 108 patients with PBC, there were 87 (80.6%) female patients and 102 patients (94.4%) with positive autoantibody. As for the stage of liver fibrosis, there were 5 patients (4.6%) in S0 stage, 41 (38.0%) in S1 stage, 23 (21.3%) in S2 stage, 25 (23.1%) in S3 stage, and 14 (13.0%) in S4 stage. There was a significant difference in the level of complement C3 between the patients with different liver fibrosis stages (H=42.891, P<0.001). The level of complement C3 gradually decreased with the aggravation of liver fibrosis, with a negative correlation between them (r=-0.565, P<0.001). Liver stiffness measurement (LSM), aspartate aminotransferase/alanine aminotransferase ratio, aspartate aminotransferase-to-platelet ratio index, and fibrosis-4 were negatively correlated with complement C3, with a correlation coefficient of -0.439 (P<0.001), -0.323 (P=0.001), -0.206 (P=0.033), and -0.291 (P=0.002), respectively. The multivariate logistic regression analysis showed that complement C3 level was an independent predictive factor for significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis, while LSM was an independent predictive factor for significant liver fibrosis and progressive liver fibrosis. The ROC curve analysis showed that complement C3 had an AUC of 0.731, 0.832, and 0.968, respectively, in the diagnosis of significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis, with a corresponding cut-off value of 1.445, 1.235, and 1.005, respectively, and complement C3 combined with LSM had an AUC of 0.811, 0.941, and 0.976, respectively, in the diagnosis of significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis. There was a significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of significant liver fibrosis (Z=2.604, P=0.009), and there was also a significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of progressive liver fibrosis (Z=3.033, P=0.002); there was no significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of liver cirrhosis (Z=1.050, P=0.294), while There was a significant difference in AUC between complement C3 combined with LSM and LSM alone in the diagnosis of liver cirrhosis (Z=2.326, P=0.020).Conclusion Serum complement C3 level has a certain clinical value in assessing the degree of liver fibrosis in patients with PBC, and complement C3 combined with LSM can further improve the efficacy of complement C3 or LSM in the diagnosis of liver fibrosis in PBC.
COLAPIETRO F, BERTAZZONI A, LLEO A. Contemporary epidemiology of primary biliary cholangitis[J]. Clin Liver Dis, 2022, 26( 4): 555- 570. DOI: 10.1016/j.cld.2022.06.001.
[2]
Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Infectious Diseases. Consensus on the diagnosis and treatment of primary biliary cirrhosis(also known as primary biliary cholangitis)(2015)[J]. J Clin Hepatol, 2015, 31( 12): 1980- 1988. DOI: 10.3969/j.issn.1001-5256.2015.12.004.
Chinese Medical Association, Branch Hepatology. Guidelines for the diagnosis and treatment of primary biliary cholangitis(2021)[J]. J Clin Hepatol, 2022, 38( 1): 35- 41. DOI: 10.3969/j.issn.1001-5256.2022.01.007.
Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Infectious Diseases. Consensus on the diagnosis and treatment of liver fibrosis(2019)[J]. J Clin Hepatol, 2019, 35( 10): 2163- 2172. DOI: 10.3969/j.issn.1001-5256.2019.10.007.
YANG YL, ZHAO RC, ZHANG FC. Potential mesenchymal stem cell therapeutics for treating primary biliary cholangitis: Advances, challenges, and perspectives[J]. Front Cell Dev Biol, 2022, 10: 933565. DOI: 10.3389/fcell.2022.933565.
[8]
BUGDACI MS, ALKIM C, KARACA C, et al. Could complement C4 be an alternative to biopsy for chronic hepatitis B histopathologic findings?[J]. J Clin Gastroenterol, 2011, 45( 5): 449- 455. DOI: 10.1097/MCG.0b013e31820f7ee5.
[9]
LI Q, LU Q, ZHU MQ, et al. Lower level of complement component C3 and C3a in the plasma means poor outcome in the patients with hepatitis B virus related acute-on-chronic liver failure[J]. BMC Gastroenterol, 2020, 20( 1): 106. DOI: 10.1186/s12876-020-01258-3.
[10]
CHEN C, YUAN Z, LI WX, et al. Complement C3 facilitates stratification of stages of chronic hepatitis B and signifies development of acute-on-chronic liver failure in acute decompensated cirrhosis[J]. Adv Ther, 2023, 40( 3): 1171- 1186. DOI: 10.1007/s12325-022-02416-7.
[11]
RICKLIN D, HAJISHENGALLIS G, YANG K, et al. Complement: A key system for immune surveillance and homeostasis[J]. Nat Immunol, 2010, 11( 9): 785- 797. DOI: 10.1038/ni.1923.
[12]
TROUW LA, DAHA MR. Role of complement in innate immunity and host defense[J]. Immunol Lett, 2011, 138( 1): 35- 37. DOI: 10.1016/j.imlet.2011.02.014.
[13]
SAHU A, LAMBRIS JD. Structure and biology of complement protein C3, a connecting link between innate and acquired immunity[J]. Immunol Rev, 2001, 180: 35- 48. DOI: 10.1034/j.1600-065x.2001.1800103.x.
[14]
LUBBERS R, van ESSEN MF, van KOOTEN C, et al. Production of complement components by cells of the immune system[J]. Clin Exp Immunol, 2017, 188( 2): 183- 194. DOI: 10.1111/cei.12952.
SCHLESINGER M, BENBASSAT C, SHOENFELD Y. Complement profile in primary biliary cirrhosis[J]. Immunol Res, 1992, 11( 2): 98- 103. DOI: 10.1007/BF02918614.
[17]
BARAK V, SELMI C, SCHLESINGER M, et al. Serum inflammatory cytokines, complement components, and soluble interleukin 2 receptor in primary biliary cirrhosis[J]. J Autoimmun, 2009, 33( 3-4): 178- 182. DOI: 10.1016/j.jaut.2009.09.010.
[18]
BIEWENGA M, FARINA SARASQUETA A, TUSHUIZEN ME, et al. The role of complement activation in autoimmune liver disease[J]. Autoimmun Rev, 2020, 19( 6): 102534. DOI: 10.1016/j.autrev.2020.102534.
[19]
HOMANN C, VARMING K, HØGÅSEN K, et al. Acquired C3 deficiency in patients with alcoholic cirrhosis predisposes to infection and increased mortality[J]. Gut, 1997, 40( 4): 544- 549. DOI: 10.1136/gut.40.4.544.
[20]
GARRED P, LYON H, CHRISTOFFERSEN P, et al. Deposition of C3, the terminal complement complex and vitronectin in primary biliary cirrhosis and primary sclerosing cholangitis[J]. Liver, 1993, 13( 6): 305- 310. DOI: 10.1111/j.1600-0676.1993.tb00650.x.
[21]
YUAN H, LI YW, LI J, et al. Clinical feature of patients with primary biliary cholangitis and primary biliary cirrhosis[J]. J Pract Hepatol, 2022, 25( 3): 403- 406. DOI: 10.3969/j.issn.1672-5069.2022.03.025.
NIU WL, WANG YS, WU QS, et al. A clinical study of clinical cure after the addition of interferon therapy in chronic hepatitis B patients with low-level HBsAg previously treated with nucleos(t)ide analogues[J]. J Clin Hepatol, 2021, 37(8): 1793-1797. DOI: 10.3969/j.issn.1001-5256.2021.08.010.
NIU WL, WANG YS, WU QS, et al. A clinical study of clinical cure after the addition of interferon therapy in chronic hepatitis B patients with low-level HBsAg previously treated with nucleos(t)ide analogues[J]. J Clin Hepatol, 2021, 37(8): 1793-1797. DOI: 10.3969/j.issn.1001-5256.2021.08.010.
 下载:
下载:






 DownLoad:
DownLoad: