Abstract:
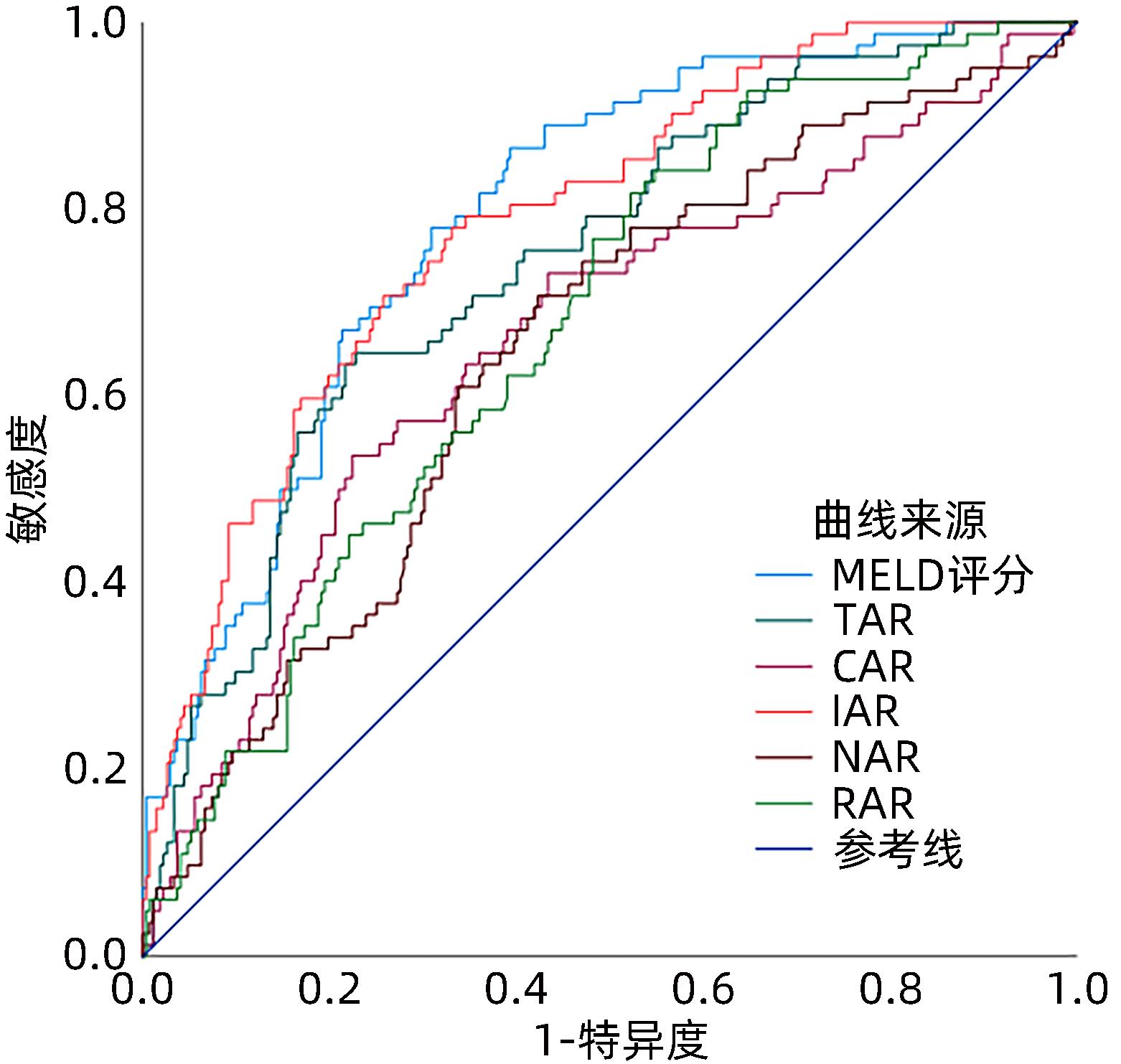
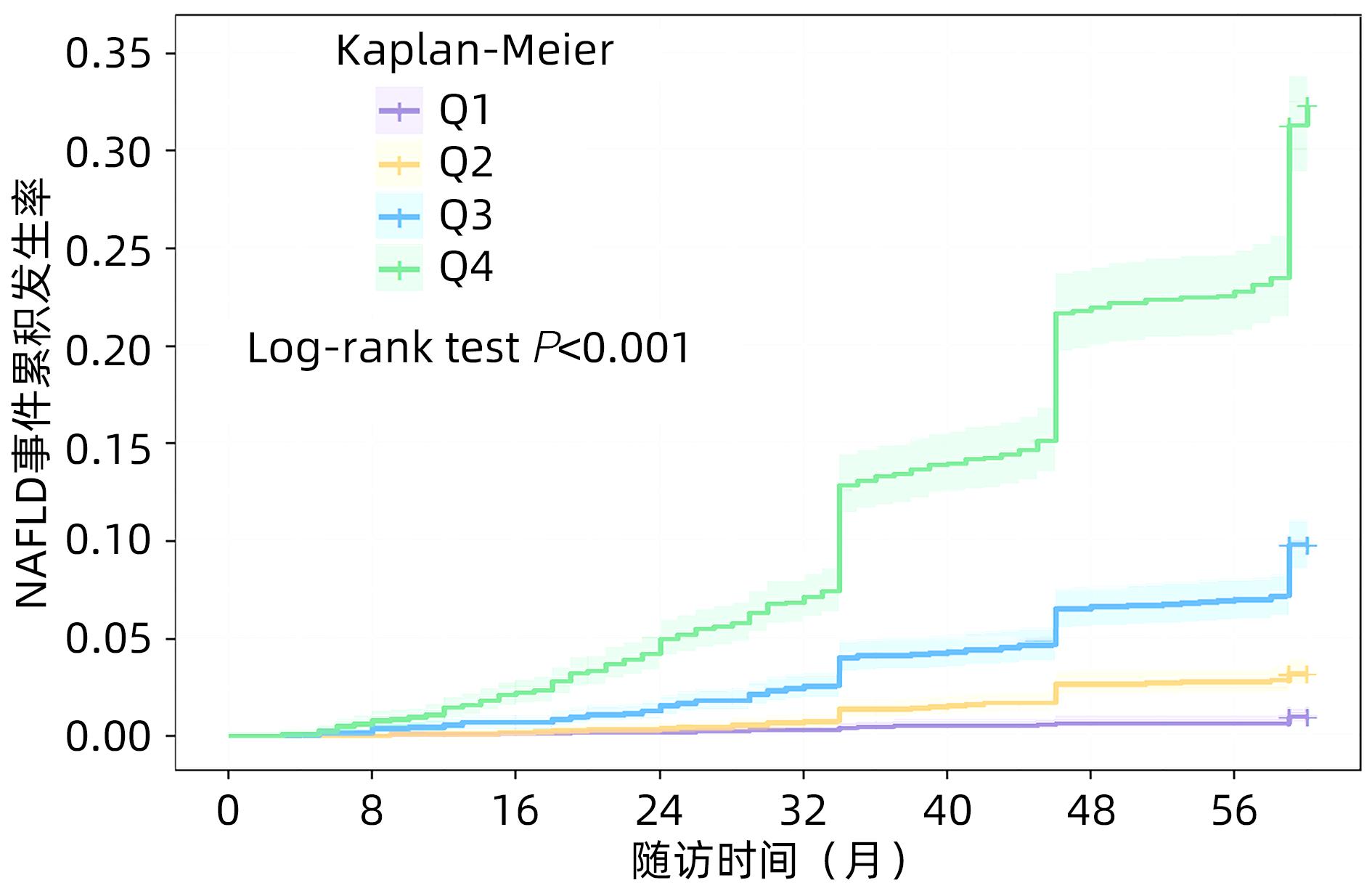
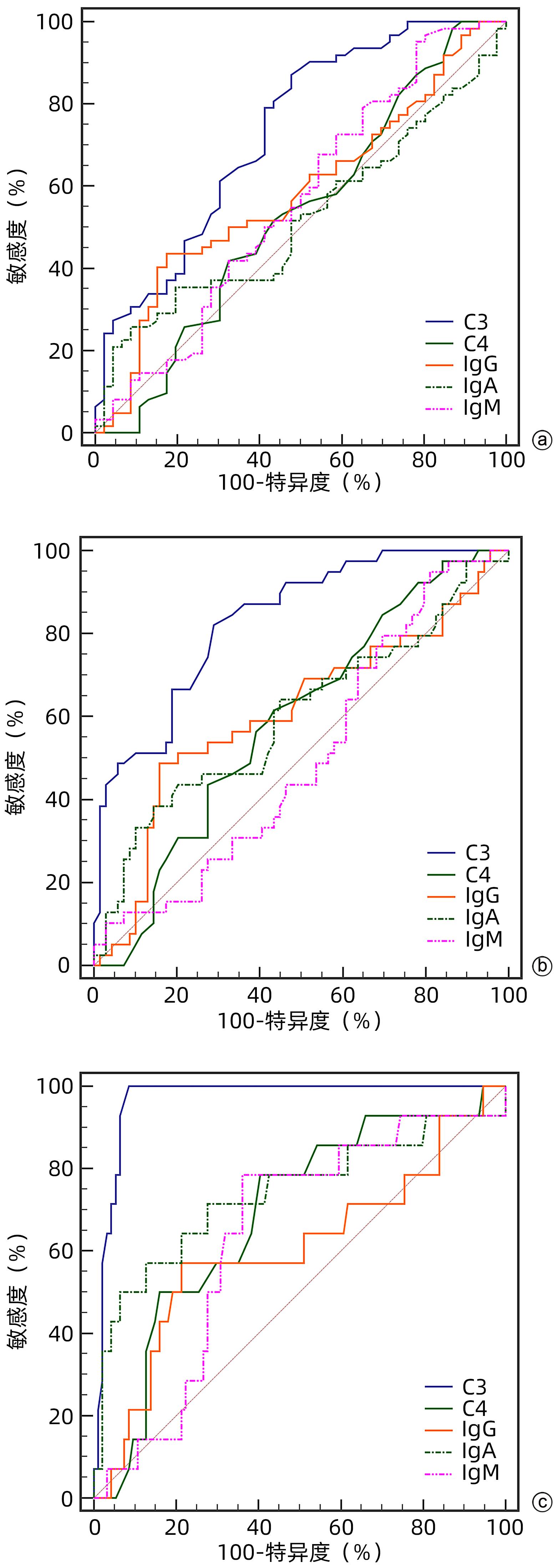
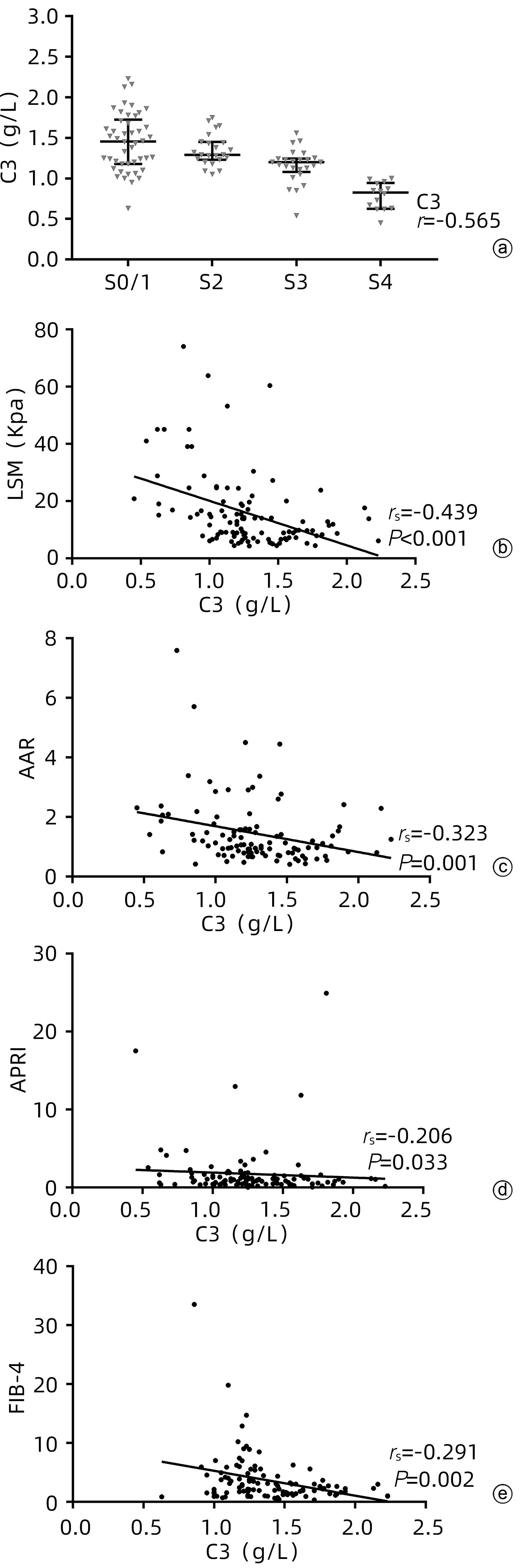
Objective To investigate the value of serum complement C3 level in determining the stage of liver fibrosis in primary biliary cholangitis (PBC). Methods Clinical data were collected from 108 patients with PBC who attended Tianjin Second People’s Hospital and underwent liver biopsy from January 2012 to October 2022. The degree of liver fibrosis (S0-4) was assessed according to the Scheuer scoring system, with ≥S2 defined as significant liver fibrosis, ≥S3 defined as progressive liver fibrosis, and S4 defined as liver cirrhosis. The independent samples t-test was used for comparison of normally distributed continuous data between two groups, and a one-way analysis of variance was used for comparison between multiple groups; the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups, and the Kruskal-Wallis H test was used for comparison between multiple groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The area under the ROC curve (AUC) was used to evaluate the efficacy of complement C3 in the diagnosis of liver fibrosis in patients with PBC. The Spearman correlation analysis was used to investigate the correlation between complement C3 and liver fibrosis stage. Results Among the 108 patients with PBC, there were 87 (80.6%) female patients and 102 patients (94.4%) with positive autoantibody. As for the stage of liver fibrosis, there were 5 patients (4.6%) in S0 stage, 41 (38.0%) in S1 stage, 23 (21.3%) in S2 stage, 25 (23.1%) in S3 stage, and 14 (13.0%) in S4 stage. There was a significant difference in the level of complement C3 between the patients with different liver fibrosis stages (H=42.891, P<0.001). The level of complement C3 gradually decreased with the aggravation of liver fibrosis, with a negative correlation between them (r=-0.565, P<0.001). Liver stiffness measurement (LSM), aspartate aminotransferase/alanine aminotransferase ratio, aspartate aminotransferase-to-platelet ratio index, and fibrosis-4 were negatively correlated with complement C3, with a correlation coefficient of -0.439 (P<0.001), -0.323 (P=0.001), -0.206 (P=0.033), and -0.291 (P=0.002), respectively. The multivariate logistic regression analysis showed that complement C3 level was an independent predictive factor for significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis, while LSM was an independent predictive factor for significant liver fibrosis and progressive liver fibrosis. The ROC curve analysis showed that complement C3 had an AUC of 0.731, 0.832, and 0.968, respectively, in the diagnosis of significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis, with a corresponding cut-off value of 1.445, 1.235, and 1.005, respectively, and complement C3 combined with LSM had an AUC of 0.811, 0.941, and 0.976, respectively, in the diagnosis of significant liver fibrosis, progressive liver fibrosis, and liver cirrhosis. There was a significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of significant liver fibrosis (Z=2.604, P=0.009), and there was also a significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of progressive liver fibrosis (Z=3.033, P=0.002); there was no significant difference in AUC between complement C3 combined with LSM and complement C3 alone in the diagnosis of liver cirrhosis (Z=1.050, P=0.294), while There was a significant difference in AUC between complement C3 combined with LSM and LSM alone in the diagnosis of liver cirrhosis (Z=2.326, P=0.020). Conclusion Serum complement C3 level has a certain clinical value in assessing the degree of liver fibrosis in patients with PBC, and complement C3 combined with LSM can further improve the efficacy of complement C3 or LSM in the diagnosis of liver fibrosis in PBC.
ZHOU H, NIU B, MI YQ, et al. Value of serum complement C3 in the diagnosis of liver fibrosis associated with primary biliary cholangitis[J]. J Clin Hepatol, 2023,39(11): 2596-2606.. doi: 10.3969/j.issn.1001-5256.2023.11.013.

 Abstract
Abstract HTML
HTML PDF (532KB)
PDF (532KB)