Abstract:
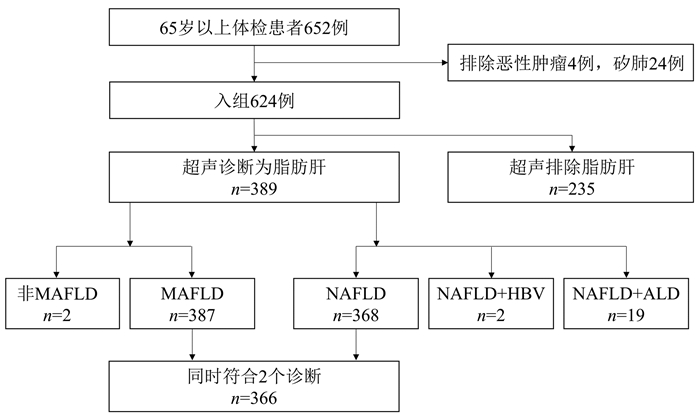
Objective To investigate the population differences of the newly named "metabolic associated fatty liver disease" (MAFLD) and the former name "nonalcoholic fatty liver disease" (NAFLD). Methods From November 2020 to January 2021, a cross-sectional survey was conducted among 624 elderly individuals aged above 65 years in a community in Beijing, China, and related data were collected, including demographic data, past history, laboratory markers, liver ultrasound, and liver elasticity. According to the presence or absence of fatty liver based on ultrasonic diagnosis, the individuals were divided into fatty liver group with 389 individuals and non-fatty liver group with 235 individuals. The independent samples t-test was used for comparison of normally distributed continuous data between the two groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between the two groups; the chi-square test was used for comparison of categorical data between the two groups. Results Among the 389 patients with fatty liver, 387(99.5%) were diagnosed with MAFLD and 368(94.6%) were diagnosed with NAFLD, and there were 19 patients with a history of heavy alcohol consumption and 2 with positive surface antigen. A total of 366 patients met the diagnostic criteria for both MAFLD and NAFLD, accounting for 94.6% of the MAFLD patients and 99.5% of the NAFLD patients. Compared with the non-fatty liver group, the MAFLD group had significant increases in body mass index (BMI) (t=-11.228, P < 0.05), waist circumference (Z=-8.532, P < 0.05), hip circumference (Z=-6.449, P < 0.05), waist-hip ratio (Z=-5.708, P < 0.05), alanine aminotransferase (Z=-5.027, P < 0.05), aspartate aminotransferase (Z=-2.880, P < 0.05), platelet count (t=-3.623, P < 0.05), triglyceride (Z=-8.489, P < 0.05), fasting blood glucose (Z=-3.516, P < 0.05), HbA1c (Z=-2.884, P < 0.05), Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (Z=-0.394, P < 0.05), high-sensitivity C-reactive protein (Z=-4.912, P < 0.05), controlled attenuation parameter (CAP) (t=13.744, P < 0.05), and liver stiffness measurement (LSM) (Z=-7.69, P < 0.05), as well as a significant reduction in high-density lipoprotein cholesterol (HDL-C) (t=6.348, P < 0.001). Meanwhile, MAFLD patients had more metabolic associated diseases, such as overweight, obesity, central obesity, dyslipidemia, and hypertension (χ2=9.978, 65.472, 36.571, 9.797, and 5.128, all P < 0.05). In the MAFLD group, 30.7% of the patients had non-obese fatty liver disease (BMI < 25 kg/m2), and 11.1% had lean fatty liver disease (BMI < 23 kg/m2); compared with the obese MAFLD patients, the non-obese MAFLD patients had significantly lower age (Z=-3.042, P < 0.05), BMI (Z=-15.705, P < 0.05), waist circumference (Z=-9.589, P < 0.05), hip circumference (Z=-10.275, P < 0.05), HOMA-IR (Z=-2.081, P < 0.05), CAP (t=-3.468, P < 0.05), LSM (Z=-3.630, P < 0.05), and NAFLD fibrosis score (t=-4.433, P < 0.05). According to LSM value, advanced liver fibrosis accounted for 3.6% of the MAFLD population, and 10% of the MAFLD population could not be excluded for advanced liver fibrosis. Conclusion The diagnosis of MAFLD can basically cover the NAFLD population in the elderly people, and it is supposed that MAFLD can almost directly replace the concept of NAFLD in similar populations. However, further studies are needed to investigate its application in other populations.
ZHANG S, LIU XH, WANG G, et al. Population differences of metabolic associated fatty liver disease and nonalcoholic fatty liver disease based on a community elderly population[J]. J Clin Hepatol, 2022, 38(3): 547-552.. doi: 10.3969/j.issn.1001-5256.2022.03.011.

 Abstract
Abstract HTML
HTML PDF (1923KB)
PDF (1923KB)