Prognosis and adverse reactions of patients with acute-on-chronic liver failure receiving artificial liver support therapy stratified by international normalized ratio
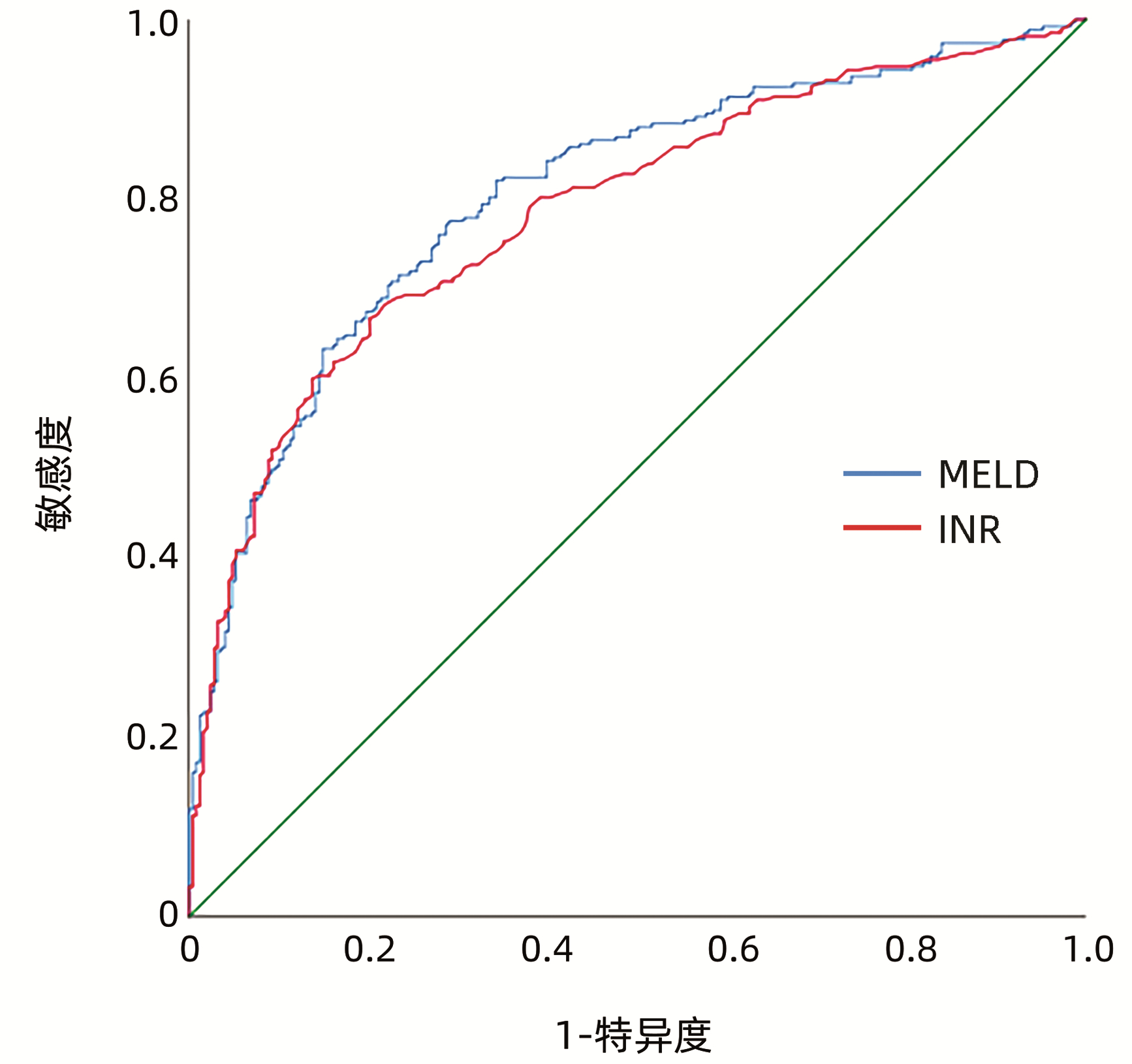
Objective To investigate the prognosis and adverse reactions of patients with acute-on-chronic liver failure (ACLF) receiving artificial liver support therapy stratified by international normalized ratio (INR).Methods A total of 515 ACLF patients who received artificial liver support therapy in Department of Severe liver Disease, The Ninth Hospital of Nanchang, from January 2010 to May 2020 were enrolled, and according to the level of INR, they were divided into group A with 20 patients (INR < 1.5), group B with 115 patients (1.5≤INR < 1.9), group C with 179 patients (1.9≤INR < 2.6), group D with 61 patients (2.6≤INR < 3.2), group E with 75 patients (3.2≤INR < 4.2), and group F with 65 patients (INR≥4.2). All patients received multimodality medical treatment combined with artificial liver support therapy. The one-way analysis of variance was used for comparison of normally distributed continuous data between multiple groups; the Kruskal-Wallis H test was used for comparison of non-normally distributed continuous data between multiple groups。The chi-square test was used for comparison of categorical data between groups. Bonferroni correction was used for further comparison between two groups. and the receiver operating characteristic (ROC) curve was used to evaluate the value of INR and MELD scoring system in predicting the prognosis of ACLF patients.Results As for 90-day mortality rate, there was a significant difference between the six groups stratified by INR (χ2=124.84, P < 0.001); there was no significant difference between groups A(25%), B(25.2%), and C(39.7%) (P > 0.05), and there was a significant difference between groups D/E/F(65.6%, 82.7%, and 92.3%, respectively) and groups A/B/C (all P < 0.05); there was no significant difference between groups D and E and between groups E and F (P > 0.05), and there was a significant difference between groups D and F (P < 0.05). There was no significant difference in the incidence rate of intraoperative adverse reactions between the six groups (χ2=8.956, P=0.111). INR had an area under the ROC curve of 0.786 (95% confidence interval: 0.746-0.825, P < 0.001) in predicting the prognosis of patients with ACLF receiving artificial liver support therapy, with a sensitivity of 66.7% and a specificity of 79.8%.Conclusion INR has a good value in predicting the prognosis of ACLF patients receiving artificial liver support therapy, and the artificial liver has good safety.
慢性乙型肝炎(CHB)相关的慢加急性肝衰竭(acute-on-chronic hepatitis B liver failure,ACHBLF)是在慢性HBV感染引起的CHB基础上出现的急性严重肝功能障碍临床综合征,病死率极高。因我国慢性HBV的高感染率,ACHBLF已成为影响患者生存质量的重要因素[1]。在CHB向ACHBLF进展过程中,存在着患者肝功能急剧恶化,但尚未达到肝衰竭的“肝衰竭前期(pre-ACHBLF)”阶段[2],如能在此阶段进行预警及干预,则有可能预防进一步发展为肝衰竭。
目前普遍认为细胞免疫功能紊乱是ACHBLF发生的病理机制之一,许多免疫细胞如髓系抑制性细胞(myeloid-derived suppressor cells, MDSC)、调节性T淋巴细胞(Treg)、分泌IL-17的CD4 T淋巴细胞(IL-17-producing CD4 T cells,Th17)和细胞毒性T淋巴细胞等在肝衰竭的发病中发挥重要作用[3-5]。尽管既往许多研究已证实肝衰竭发病与免疫密切相关,但pre-ACHBLF阶段的免疫状态及其与疾病进展的关系尚不清楚,因此本研究探讨了MDSC、Th17、Treg和分泌IL-17的CD8 T淋巴细胞(IL-17-producing CD8 T cells, Tc17)在pre-ACHBLF和ACHBLF患者中的表达,以期为ACHBLF的早期治疗提供思路。
Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.
XIAO LL, XU XW, HUANG KZ, et al. Artificial liver support system improves short-term outcomes of patients with HBV-associated acute-on-chronic liver failure: A propensity score analysis[J]. Biomed Res Int, 2019, 2019: 3757149. DOI: 10.1155/2019/3757149.
[3]
FAN Q, LI Z. Liver transplantation for acute-on-chronic liver failure[J]. Ogran Transplant, 2022, 13(3): 333-337. DOI: 10.3969/j.issn.1674-7445.2022.03.008.
ALSHAMSI F, ALSHAMMARI K, BELLEY-COTE E, et al. Extracorporeal liver support in patients with liver failure: a systematic review and meta-analysis of randomized trials[J]. Intensive Care Med, 2020, 46(1): 1-16. DOI: 10.1007/s00134-019-05783-y.
[5]
Liver Failure and Artificial Liver Group, Chinese Society of Infectious Diseases, Chinese Medical Association; Severe Liver Disease and Artificial Liver Group, Chinese Society of Hepatology, Chinese Medical Association. Guideline for diagnosis and treatment of liver failure(2018)[J]. J Clin Hepatol, 2019, 35(1): 38-44. DOI: 10.3969/j.issn.1001-5256.2019.01.007.
Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35(11): 2408-2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.
PORTE RJ, LISMAN T, TRIPODI A, et al. The International Normalized Ratio (INR) in the MELD score: problems and solutions[J]. Am J Transplant, 2010, 10(6): 1349-1353. DOI: 10.1111/j.1600-6143.2010.03064.x.
[8]
MOREAU R, JALAN R, GINES P, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis[J]. Gastroenterology, 2013, 144(7): 1426-1437. DOI: 10.1053/j.gastro.2013.02.042.
[9]
CLÀRIA J, STAUBER RE, COENRAAD MJ, et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure[J]. Hepatology, 2016, 64(4): 1249-1264. DOI: 10.1002/hep.28740.
[10]
RUESCHENBAUM S, CIESEK S, QUECK A, et al. Dysregulated adaptive immunity is an early event in liver cirrhosis preceding acute-on-chronic liver failure[J]. Front Immunol, 2021, 11: 534731. DOI: 10.3389/fimmu.2020.534731.
[11]
ZHANG CX, GENG JW, XIE Q. Global disease burden and regional differences of acute-on-chronic liver failure: a review[J]. Chin Hepatol, 2021, 26(4): 355-358. DOI: 10.3969/j.issn.1008-1704.2021.04.003.
NOVELLI G, ANNESINI MC, MORABITO V, et al. Cytokine level modifications: molecular adsorbent recirculating system versus standard medical therapy[J]. Transplant Proc, 2009, 41(4): 1243-1248. DOI: 10.1016/j.transproceed.2009.03.035.
[15]
XU KL, LEI M, YUAN WF, et al. Effect of dual plasma molecular adsorption system in the treatment of hyperbilirubinemia in patients with liver failure[J]. Traum Crit Med, 2020, 8(2): 91-93, 96. DOI: 10.16048/j.issn.2095-5561.2020.02.08.
WIESNER R, EDWARDS E, FREEMAN R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers[J]. Gastroenterology, 2003, 124(1): 91-96. DOI: 10.1053/gast.2003.50016.
[17]
HERNAEZ R, SOLÀ E, MOREAU R, et al. Acute-on-chronic liver failure: an update[J]. Gut, 2017, 66(3): 541-553. DOI: 10.1136/gutjnl-2016-312670.
[18]
JALAN R, SALIBA F, PAVESI M, et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure[J]. J Hepatol, 2014, 61(5): 1038-1047. DOI: 10.1016/j.jhep.2014.06.012.
[19]
DU L, MA Y, ZHOU S, et al. A prognostic score for patients with acute-on-chronic liver failure treated with plasma exchange-centered artificial liver support system[J]. Sci Rep, 2021, 11(1): 1469. DOI: 10.1038/s41598-021-81019-8.
[20]
MA S, XIE Z, ZHANG H, et al. Characterization of an artificial liver support system-related vasovagal reaction[J]. Biomed Res Int, 2020, 2020: 6313480. DOI: 10.1155/2020/6313480.
WANG F, LU JH, LIU YG, et al. Expression and significance of immune cells in patients with hepatitis B virus-related acute-on-chronic pre-liver failure[J]. J Clin Hepatol, 2023, 39(1): 77-82. DOI: 10.3969/j.issn.1001-5256.2023.01.012.
WANG F, LU JH, LIU YG, et al. Expression and significance of immune cells in patients with hepatitis B virus-related acute-on-chronic pre-liver failure[J]. J Clin Hepatol, 2023, 39(1): 77-82. DOI: 10.3969/j.issn.1001-5256.2023.01.012.
 下载:
下载:







 DownLoad:
DownLoad: