Abstract:
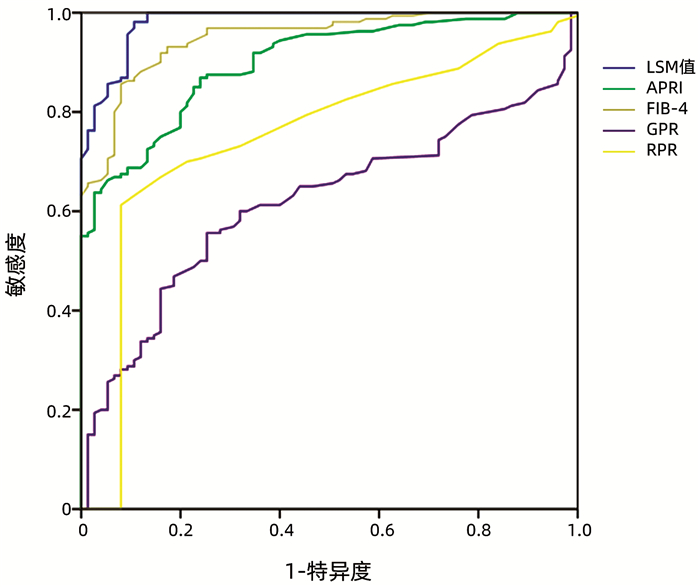
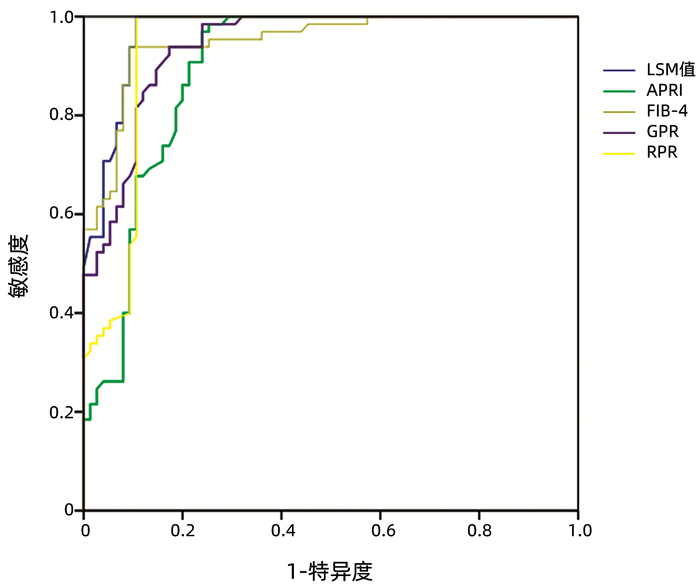
Objective To investigate the association of five noninvasive diagnostic methods for liver cirrhosis, i.e., liver stiffness measurement (LSM) on FibroScan, aspartate aminotransferase-to-platelet ratio index (APRI), fibrosis-4 (FIB-4), gamma-glutamyl transpeptidase-to-platelet ratio (GPR), and red blood cell distribution width-to-platelet ratio (RPR), with traditional Chinese medicine (TCM) syndrome types in patients with compensated hepatitis B cirrhosis. Methods A retrospective analysis was performed for the clinical data of 327 patients who were diagnosed with compensated hepatitis B cirrhosis in The First Affiliated Hospital of Henan University of Chinese Medicine from January 2017 to January 2020, and based on their TCM syndrome type, they were divided into liver depression and spleen deficiency group with 160 patients, liver-gallbladder damp-heat syndrome group with 84 patients, liver-kidney Yin deficiency group with 13 patients, spleen-kidney Yang deficiency group with 5 patients, and blood stasis obstructing the collaterals group with 65 patients. Related data were collected, including clinical data, routine blood test results, liver function, LSM, and color Doppler ultrasound findings of liver, gallbladder, spleen, and pancreas. TCM syndrome differentiation was performed, and the models of APRI, FIB-4, GPR, and RPR were established. A one-way analysis of variance was used for comparison of normally distributed continuous data between multiple groups, and the least significant difference t-test was used for further comparison between two groups; the multiple independent samples Kruskal-Wallis H rank sum test was used for comparison of non-normally distributed continuous data between multiple groups, and the one- way Kruskal-Wallis ANOVA (k-sample) was used for multiple comparison; the binary logistic regression analysis was used to investigate the association between TCM syndrome types and non-invasive diagnosis of liver cirrhosis; the receiver operating characteristic (ROC) curve was used to evaluate the diagnostic capability of five noninvasive methods for predicting TCM syndrome type in compensated hepatitis B cirrhosis. Results The logistic regression analysis showed that in the liver-gallbladder damp-heat syndrome group, aspartate aminotransferase OR=1.981, 95%CI: 1.8225-2.139, P < 0.05), and LSM (OR=2.002, 95%CI: 1.840-2.160, P < 0.05) were influencing factors for compensated hepatitis B cirrhosis; in the liver depression and spleen deficiency group, portal vein width (OR=4.402, 95%CI: 4.050-4.754, P < 0.05), LSM (OR=3.901, 95%CI: 3.589-4.213, P < 0.05), APRI (OR=1.891, 95%CI: 1.740-2.042, P < 0.05), and FIB-4 (OR=1.845, 95%CI: 1.697-1.993, P < 0.05) were influencing factors for compensated hepatitis B cirrhosis; in the blood stasis obstructing the collaterals group, LSM (OR=2.465, 95%CI: 2.268-2.662, P < 0.05), APRI (OR=1.298, 95%CI: 1.194-1.402, P < 0.05), and FIB-4 (OR=1.849, 95%CI: 1.701-1.997, P < 0.05) were influencing factors for compensated hepatitis B cirrhosis. The ROC curve analysis showed that LSM and RPR had a significantly better diagnostic value than the other methods in evaluating liver-gallbladder damp-heat syndrome, and LSM and FIB-4 had a significantly better diagnostic value than the other methods in evaluating liver depression and spleen deficiency; all five noninvasive diagnostic methods had a good value in evaluating the syndrome of blood stasis obstructing the collaterals. Conclusion The five noninvasive diagnostic methods have their own advantages in evaluating different syndrome types, which provide a reference for the diagnosis of TCM syndrome types in patients with compensated hepatitis B cirrhosis.
YU ZJ, ZHAO WX, FENG LX, et al. Value of five noninvasive diagnostic methods for liver cirrhosis in diagnosis of traditional Chinese medicine syndrome types in patients with compensated hepatitis B cirrhosis[J]. J Clin Hepatol, 2022, 38(1): 104-109.. doi: 10.3969/j.issn.1001-5256.2022.01.016.

 Abstract
Abstract HTML
HTML PDF (1982KB)
PDF (1982KB)